Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2014) Volume 3, Issue 3
Multiple mechanisms have been suggested for the pathogenesis of these multiglandular autoimmune diseases. One of proposed mechanisms in the multiglandular autoimmune disease is initiated by antibodies. However, the results are not definitive and remain controversial. We investigated a woman with multiple autoimmune diseases, in whose serum the mRNA of sodium iodide symporter (NIS) was found by nested reverse transcription polymerase chain reaction (RT-PCR). In this patient, multiple autoimmune diseases were initially developed as thyroiditis, followed by Sjögren syndrome, hepatitis, and finally a diagnosis of atrophic gastritis. NIS is known to be expressed on organs affected by these diseases. The mRNA of NIS was found in the serum of this patient by nested RT-PCR. The pathogenesis of multiglandular autoimmune disease is still not clear. We suggest that anti NIS antibodies can serve as a marker to monitor the pathogenesis of multiglandular autoimmune disease.
<Autoimmune thyroiditis is one of the most common endocrine diseases [1]. It has been reported that autoimmune thyroiditis can have comorbid presentation with other polyglandular autoimmune diseases [2]. Neufeld and Blizzard developed a classification system for polyglandular failure in 1980 [3] and they defined type IIIB patients as having both autoimmune thyroiditis and atrophic gastritis. Centanni et al. [4] reported that about one-third of patients who presented with autoimmune thyroid disease also had atrophic gastritis. Interestingly, some investigations have reported that 20% to 24% of patients with autoimmune thyroiditis also present with Sjögren syndrome [5-8].
Several mechanisms have been suggested for the pathogenesis of this kind of multiglandular autoimmune disease [9,10]. The roles of anti-thyroid peroxidase antibodies and parietal cell antibodies have been proposed as primary diagnostic indicators [11]; however, the results are not definitive and remain a controversial issue in the field [12,13].
The basic mechanisms that regulate active iodide transport to the thyroid gland were identified in 1996 [14]. Jhiang et al. [15] reported the presence of sodium iodide symporter (NIS) on the cell membrane of thyroid follicular cells, which cotransport sodium ions with iodide ions. NIS expression is not restricted to the thyroid. It is also expressed in the salivary gland, mammary gland, gastric mucosa, pituitary gland, pancreas, liver, testis, mammary gland, gastromucosa, prostate, ovary, adrenal gland, heart, thymus, and lung [16,17].
On the basis of these findings, we speculated that an antibody against NIS could serve as a diagnostic indicator in organs affected by autoimmune disease that also express the NIS protein. To the best of our knowledge, no investigations have yet reported on the relationship between anti-NIS antibody and autoimmune disease in the associated organs. Here we report the case of a 60-year-old woman who was sequentially diagnosed with thyroiditis, Sjögren syndrome, autoimmune hepatitis, and atrophic gastritis. Furthermore, increased NIS mRNA transcripts were found in the patient’s serum.
A 60-year-old woman was admitted to the hospital with worsening liver function. She had dark urine that persisted 4 days before admission and a weight loss of 4 kg over a period of 10 days.
The patient was diagnosed with Hashimoto disease about 35 years ago. At that time, the patient’s primary complaint was diffuse goiter with hypothyroidism. On the basis of the clinical and laboratory findings, the patient was treated for a diagnosis of thyroiditis with a 150-200-μg/day dosage of thyroid hormone. Thirteen years after the diagnosis of thyroiditis, the patient visited our clinic complaining of dry mouth (for 3 years) and dry eyes (for 1 year). Physical examination showed dry tongue with papillary atrophy and left parotid gland swelling. Clinically, the patient may have had Sjögren syndrome. Within 1 year, the patient underwent surgery for lacrimal gland obstruction with aggravated xerophthalmia. In addition, the patient had intermittent epistaxis due to dryness of the mucosal membrane in the nose.
The patient had no history of alcohol and/or drug use except for the thyroid hormone treatment. The patient’s familial history was unremarkable. Upon physical examination, there were no visible skin lesions or arthralgia.
Initial laboratory findings showed a white blood cell count of 6000 cells/mm3, hemoglobin levels of 10.5 g/dL, and a platelet cell count of 170 × 103 cells/mm3. The laboratory results are presented in Table 1. The liver function profile showed markedly increased aspartate aminotransferase, alanine aminotransferase, and alkaline phosphatase levels. Total bilirubin and direct bilirubin were also increased above the normal limit. The ratio of albumin to total protein was 0.25. Among serum immunoglobulins (Ig), IgG was increased while IgA and IgM levels were normal. Serum protein electrophoresis was suggestive of polyclonal gammopathy. The markers for viral hepatitis A, B and C were all negative. Thyroid function profile showed decreased thyroid stimulating hormone (TSH) at <0.05 μIU/mL, high levels of free thyroxine (fT4) at 2.4 ng/dL, and normal levels of triiodothyronine at 69 ng/dL. Thyroid-stimulating immunoglobulin was not increased. Serum thyroglobulin and microsomal antibody levels were elevated to 1366 (normal, 0-100 U/mL) and 606 (normal, 0-100 U/mL), respectively. Anti-nuclear antibody, smooth muscle antibody, and mitochondrial antibody were all negative. Rheumatoid factor (RF), anti-Ro antibody, and anti-La antibody were all positive, and the anti-double stranded DNA antibody level was above the upper normal limit. The patient’s urine analysis result was normal. Liver ultrasonography showed diffuse and coarse hepatic echogenicity (Figure 1). There was no evidence of focal lesions in the liver. Ultrasound-guided biopsy of the liver was performed and histological findings revealed a mild degree of portal and periportal hepatitis.
| 2005.7 | After 3 weeks | 2013.7 | Normal range | |
|---|---|---|---|---|
| AST | 1040 | 21 | 22 | 0-40 IU/L |
| ALT | 671 | 21 | 13 | 0-40 IU/L |
| ALP | 208 | 108 | 80 | 30-115 IU/L |
| γ-GT | 112 | 44 | 9 | 8-35 IU/L |
| Total bilirubin | 5.9 | 1.0 | 0.6 | 0.2-1.2 mg/dL |
| Direct bilirubin | 3.8 | 0.5 | 0.1 | 0-0.5 mg/dL |
| Total protein | 10.6 | 8.1 | 9.3 | 6.0-8.0 g/dL |
| Albumin | 2.5 | 3.1 | 3.7 | 3.3-5.2 g/dL |
| IgG | 6860 | 3924 | 4318 | 700-1700 mg/dL |
| IgA | 408 | 389 | 340 | 90-400 mg/dL |
| IgM | 78 | 77 | 36 | 45-230 mg/dL |
| TSH | 0.05 | - | 0.11 | 0.4-4.1 μIU/mL |
| T3 | 69 | - | 106 | 87-184 ng/dL |
| fT4 | 2.4 | - | 1.62 | 0.7-1.8 ng/dL |
AST; aspartate transaminase, ALT; alanine transaminase, ALP; alkaline phosphatase, γ-GT; gamma glutamyl transferase; TSH, thyroid stimulating hormone; T3, triiodothyronine; T4, thyroxine
Table 1: Laboratory values
Figure 1: Ultrasonography of the liver showing diffuse coarse hepatic echogenicity
Plasma cells were observed to be located at the interface of dilated portal veins (Figure 2A) and predominant lymphoplasmacytic infiltration was evident. Clinically, autoimmune hepatitis was suspected on the basis of the international autoimmune hepatitis group scoring system [18].
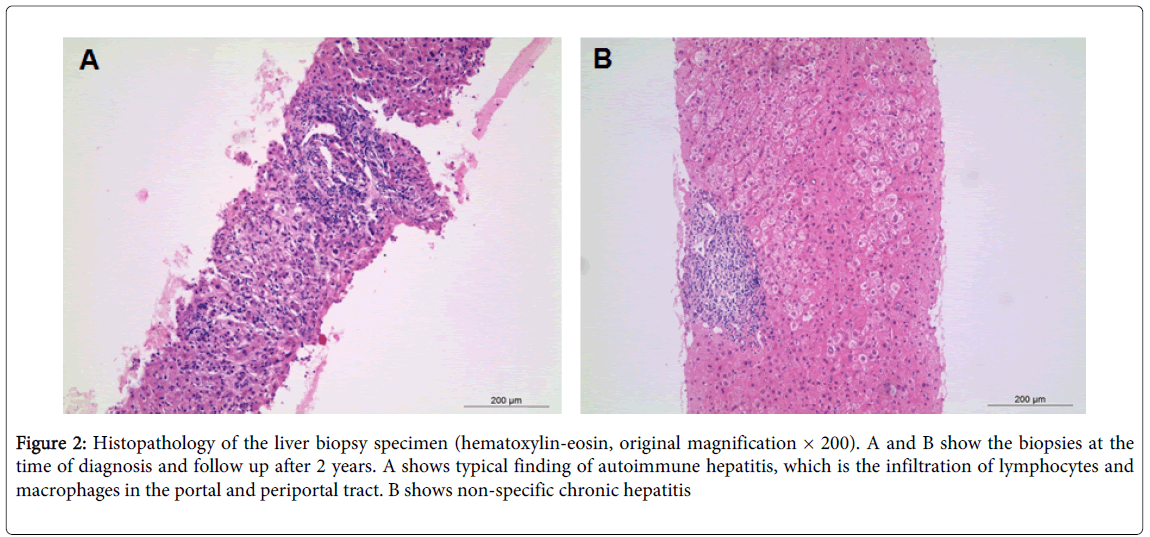
Figure 2: Histopathology of the liver biopsy specimen (hematoxylin-eosin, original magnification × 200). A and B show the biopsies at the time of diagnosis and follow up after 2 years. A shows typical finding of autoimmune hepatitis, which is the infiltration of lymphocytes and macrophages in the portal and periportal tract. B shows non-specific chronic hepatitis
A scan of the salivary gland was performed to evaluate salivary function and investigate the cause of the dry mouth symptom. As can be seen in Figure 3, bilateral parotid and submandibular glands were not visualized. The passage of saliva to the oral cavity was also not shown on the images obtained after stimulation with a sialagogue at 40 minutes after 99mTcO4- injection. The clinical symptoms (dry mouth and eye), serologic findings (positive RF and anti-Ro/La antibodies), and salivary gland scan findings supported a diagnosis of late stage Sjögren syndrome. Liver diseases and connective tissue disease have been reported as the most common diseases in patients with polyclonal gammopathy (61% and 22%, respectively) [19]. Therefore, the polyclonal gammopathy result obtained supported the diagnosis of autoimmune hepatitis and Sjögren syndrome.
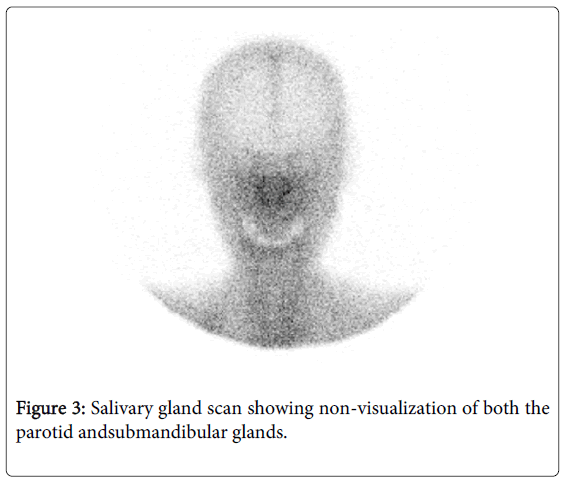
Figure 3: Salivary gland scan showing non-visualization of both the parotid andsubmandibular glands.
At the anterior region of the salivary gland scan, the thyroid gland was not visualized. This finding in combination with high fT4 levels and suppressed TSH levels indicated thyrotoxicosis due to a high dose of thyroid hormone. The patient was immediately taken off thyroid hormone treatment.
The patient was then started on oral prednisolone at a dosage of 40 mg/day to treat the autoimmune hepatitis. Five days later, clinical symptoms and laboratory findings showed an improvement and the patient’s score for autoimmune hepatitis according to the international autoimmune hepatitis group scoring system was 17, indicating autoimmune hepatitis [18]. The patient was discharged with a maintenance dose of prednisolone (30 mg/day). At the 3 week follow up, the serum enzyme levels indicated normalized liver function (Table 1). The patient was gradually tapered from prednisolone at 30 mg/day to 5 mg/day. After 2 years, liver tissue biopsied again. The histology findings revealed chronic inflammation related to hepatitis (Figure 2B) and there was no evidence of autoimmune hepatitis. Serum liver function levels were within normal range and there was no recurred symptom associated with autoimmune hepatitis for the period. The patient was placed on a long-term treatment with prednisolone at 5 mg/day. Since then, the patient has experienced indigestion and was subsequently diagnosed with atrophic gastritis using endoscopic analysis at a different hospital. Currently, the patient is taking thyroid hormone to treat the thyroiditis.
Multiglandular autoimmune diseases have been reported in several studies. About one-fourth of autoimmune disease cases tend to present with additional autoimmune disease [20]. It has been reported that autoimmune thyroid disease is the most common comorbid disease presentation when compared to other autoimmune diseases. The revised classification of multiglandular autoimmune diseases according to Betterle et al. [21] defined type IIIb as autoimmune thyroiditis with the association of other autoimmune disease (atrophic gastritis, pernicious anemia, coeliac disease, chronic inflammatory bowel disease, autoimmune hepatitis, primary biliary cirrhosis, and sclerosing cholangitis), with the exception of Addison disease and/or hypoparathyroidism.
Autoimmune thyroiditis has been shown to be associated with about 30% of cases where atrophic gastritis is listed as the primary diagnosis, while atrophic gastritis coincides in about 40% of patients whose primary diagnosis was autoimmune thyroiditis [4,20]. Autoimmune thyroiditis has been shown to coexist in about 23% of Sjögren syndrome diagnoses [5] and the prevalence of autoimmune thyroiditis among patients with Sjögren syndrome has been reported as 18% to 24%, respectively [7,8,23]. Autoimmune hepatitis is frequently a comorbid presentation with autoimmune thyroiditis (18.3%) and Sjögren syndrome (8.4%) [24].
Some specific proteins have been suggested as a possible causal factor in the pathogenesis of multiglandular autoimmune disease [25,26]. In concurrent autoimmune thyroiditis with atrophic gastritis, antimicrosomal antibody, anti-peroxidase antibody, or antiparietal antibody have been used in an attempt to explain the relation with
Concurrent autoimmune thyroiditis [11]. However, there are not enough cases to support the use of specific antibodies to be indicative of a primary cause. Accordingly, a common autoantigen of multiple organs that are affected by autoimmune diseases should be applied as a diagnostic indicator to better understand the pathogenesis. A similar situation has been suggested for a specific epitope shared between the thyroid and gastric parietal cell [11]. However, evidence regarding its existence remains unclear. From histologic findings, the association between thyroiditis and Sjögren syndrome may be explained, in part, by common epithelial antigens. The pathology of the thyroid glands in autoimmune thyroid disease, and salivary and lachrymal glands in Sjögren syndrome, show similarities such as infiltration by activated T cells and expression of HLA-class II molecules on the epithelial cells. These findings support the hypothesis that these multiglandular autoimmune diseases could share pathogenic mechanisms and antigens, which could clarify their associations. However, there is still no obvious evidence for the pathogenesis of multiglandular autoimmune diseases. The patient in the current study was diagnosed with 4 autoimmune diseases involving the thyroid, salivary gland, stomach, and liver. These organs express the NIS protein on their surface epithelium. The NIS expression observed in the liver was relatively obscure; however, its expression has been reported by Ajjan et al. [16]. NIS is widely known as an autoantigen of autoimmune thyroid disease and its antibodies are often detected at increased levels in patients with autoimmune thyroid disease [27,28]. It is conceivable that multiglandular autoimmune disease could be explored using a single NIS antibody. To the best of our knowledge, there has been little mention of the relationship between anti-NIS antibodies and multiple autoimmune diseases. Initially, the patient in our study was diagnosed with autoimmune thyroiditis in her 20s. After 13 years, the patient developed sialadenitis accompanied with parotid gland swelling, and symptoms of dry eye and dry mouth. At 35 years from the initial diagnosis of thyroiditis, the patient’s autoimmune hepatitis was identified through pathology and other laboratory tests. The patient subsequently experienced indigestion and was diagnosed with atrophic gastritis using endoscopic analysis. There was no sign of infections such as that by Helicobacter pylori. The patient’s gastric antibody or serum gastrin levels were not assessed. However, the patient’s anemia (hemoglobin 10.5 g/dL) might have been indicative of atrophic gastritis [4]. Some researchers have proved sensitive RT-PCR assays to amplify NIS mRNA in patient’s blood [29]. In this research, NIS mRNA was detected in the patient’s serum after the autoimmune hepatitis resolved (Figure 4).
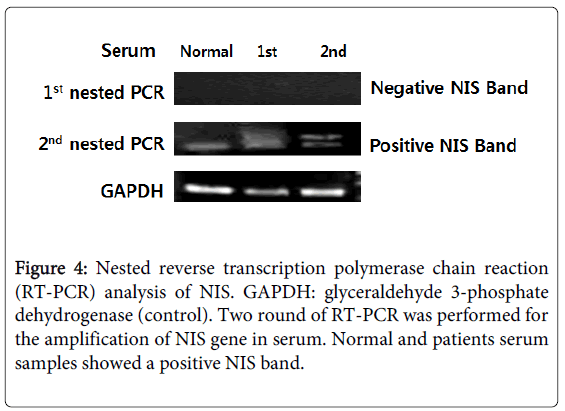
Figure 4: Nested reverse transcription polymerase chain reaction (RT-PCR) analysis of NIS. GAPDH: glyceraldehyde 3-phosphate dehydrogenase (control). Two round of RT-PCR was performed for the amplification of NIS gene in serum. Normal and patients serum samples showed a positive NIS band.
We propose that the pathogenic process may have occurred as follows. Initially, auto-NIS antibodies were produced due to the autoimmune thyroiditis, and then the circulating auto-NIS antibodies might have sequentially attacked the NIS protein of the salivary glands, lacrimal glands, and liver. In addition, it may have been closely connected with atrophic gastritis. In the stomach, the NIS protein is located in parietal cells and auto NIS antibodies can trigger damage to parietal cells. Our suggested pathogenesis related to NIS is incomplete, as we did not measure the auto-NIS antibody level in the patient’s serum.
Herein, we reported on the case of a female patient with autoimmune diseases involving the thyroid, salivary gland, and liver as well as atrophic gastritis. From this study, we suggested that NIS might be closely associated with multiple autoimmune diseases. There are only a few case reports that have investigated concurrent autoimmune hepatitis and Sjögren syndrome in a patient with autoimmune thyroiditis. Furthermore, the relevance of auto-NIS antibodies among multiple autoimmune diseases remains to be investigated.
This work was supported by the National Research Foundation of Korea (NRF) grant for the Global Core Research Center (GCRC) funded by the Korea government (MSIP) (No. 2011-0030680).
The authors have no financial conflicts of interest to be disclosed