Journal of Cancer Science and Research
Open Access
ISSN: 2576-1447
ISSN: 2576-1447
Research Article - (2018) Volume 0, Issue 0
Keywords: Colorectal cancer; Elderly; Chemotherapy, Survival
CRC: Colorectal Cancer; mCRC: Metastatic Colorectal Cancer; FU: Fluorouracil; OS: Overall Survival; PFS: Progression-Free Survival; ADL: Activities of Daily Living; ECOG: Eastern Cooperative Oncology Group; QOL: Quality of Life.
CRC is the third leading cancer in the world, the prevalence of which increases with age [1]. The recent Surveillance, Epidemiology, and End Results (SEER) database reported that CRC cases are mostly diagnosed at the age of 65 and 74 years (median, 67 years). In addition, the mortality rate of CRC is highest in the age group of 75-84 years [2]. Recent advancements in surgical techniques and local and systemic therapies have improved the survival of patients with metastatic Colorectal Cancer (mCRC). However, the survival is still short in elderly patients compared with younger patients [3,4].
Although some patients with CRC who have isolated hepatic metastasis stand a chance of cure, several patients with mCRC are treated with palliation, and systemic chemotherapy constitutes the treatment base. Recently, the combination of Fluorouracil (FU) with Irinotecan or Oxaliplatin has been recommended as the standardized treatment of mCRC. Besides chemotherapy, several targeted drugs can be used, such as vascular endothelial growth factor antibodies (e.g., Bevacizumab, Aflibercept, and Ramucirumab), epidermal growth factor receptor antibodies (e.g., Cetuximab and Panitumumab), and tyrosine kinase inhibitors (Regorafenib). Furthermore, the use of immune checkpoint inhibitors, such as Pembrolizumab and Nivolumab, has been recently approved for patients with Microsatellite Instability (MSI-H).
In the treatment of mCRC, a combination of two antineoplastic drugs is superior to Fluoropyrimidine alone (5-FU and Calcium folinate IV or oral Capecitabine alone) [5,6]. However, these studies did not assess patients aged ≥ 70 years (elderly). A meta-analysis of studies on elderly patients comparing dual therapy and Fluoropyrimidine alone revealed that dual therapy does not exhibit a difference in the Overall Survival (OS) but prolongs the Progression- Free Survival (PFS) [7]. Lately, the addition of Bevacizumab to the standard treatment in elderly patients has exhibited an increase in PFS [8,9]. However, Cetuximab data remain highly limited, as the number of patients aged >70 years is minimal in phase 3 trials [10,11]. Similarly, data on Panitumumab remain unclear for patients aged >80 years [12].
The geriatric oncological assessment is highly complex. The functional, cognitive, social, and psychological status and comorbidities of a patient should be concomitantly evaluated. The functional status is measured with Activities of Daily Living (ADL), which addresses the ability of taking a bath, dressing up, eating, and going from chair to bed independently. Typically, the oncology discipline uses the ECOG performance status score for evaluating patients. In fact, the performance status score alone is not adequate to assess the functional status and physiological reserves. Reportedly, both ADL and ECOG performance status score should be assessed together to estimate the postoperative morbidity, chemotherapy toxicity, and survival [13]. Although the treatment principles for mCRC are similar in elderly and younger patients, chemotherapy toxicity requires consideration because of age-related physiological and functional changes and comorbidities (Table 1).
| Organ-system | Aging-related changes | Potential treatment toxicities |
|---|---|---|
| Bone marrow | Reserve decreases | The risk of neutropenia increases. |
| Liver | Volume of parenchyma decreases | Oxaliplatin-induced fatty liver becomes difficult to tolerate |
| Kidney | Glomerular filtration rate decreases | The risk of prerenal azotemia, Oxaliplatin toxicity |
| Cardiovascular | Coronary artery disease | Coronary vasospasm due to FU |
| Hypertension | Hypertension and arterial thromboembolism due to Bevacizumab | |
| Valve diseases | ||
| Central Nervous System | Cerebral perfusion decreases | Cerebral toxicity due to 5-FU. |
Table 1: Aging-related physiological and functional changes.
To date, a few studies have reviewed the effect of chemotherapy on the Quality Of Life (QOL) in elderly patients with mCRC. In the MRC FOCUS 2 study, 459 patients not eligible for full-dose chemotherapy because of advanced age or fragility were randomized to 5-FU +Calcium folinate or Capecitabine ± Oxaliplatin therapy [14]. Of note, initial doses were reduced by 20% in all groups. Owing to the evaluation, the addition of Oxaliplatin to the treatment led to a statistically significant increase in response rates, prolonged PFS and OS non-significantly, but exerted a detrimental effect on QOL. In particular, as patients aged >80 years are excluded from several treatment-related studies; studies on treatment approaches in these patients are warranted. Typically, treatment options for elderly patients are limited because of the risk of adverse effects of the treatment on QOL. Moreover, shorter life expectancy and comorbidities render the disease management challenging.
Of note, chemotherapy and addition of biological drugs are recommended for the treatment of healthy elderly patients, similar to younger patients [15]. In the first and second lines of treatment, 5-FU/ Capecitabine+Irinotecan (FOLFIRI/XELIRI) or Oxaliplatin (FOLFOX/ XELOX) ± biological drug are appropriate treatment options. However, no particular recommendation exists for the third line of treatment. While young patients are considered more suitable for multiline treatments, older patients are usually under-treated.
This study aims to elucidate whether multiline chemotherapy prolongs survival in patients aged ≥ 70 years with an ECOG performance score of 0 or 1 by maintaining treatment as long as tolerated and to investigate treatment approaches in elderly patients by assessing factors that affect the survival.
We retrospectively evaluated the medical records of 136 patients (age ≥ 70 years) who presented to our clinic between May 2009 and January 2018. We recorded patients’ age, sex, tumor histology, tumor location, genetic analysis results, performance scores (according to the ECOG score), body mass index, initial CEA levels, adjuvant treatment history, surgical interventions (colon surgery or metastasectomy), metastasis locations, comorbidities, treatment history, adverse effects, and final status (Table 2). In addition, PFS and OS were estimated based on the treatments they received.
| n=136 | 1-2 Line Chemotherapy(n=90) | >2 Line Chemotherapy (n=46) |
|---|---|---|
| Sex | ||
| Male (n=100) | 58 (58%) | 42 (42%) |
| Female (n=36) | 20 (55.5%) | 16 (44.5%) |
| Median Age | 75 | 76 |
| Histology | ||
| Adenocarcinoma (n=115) | 64 (55.6%) | 51 (44.4%) |
| Mucinous (n=12) | 6 (50%) | 6 (50%) |
| Signet Ring Cell (n=9) | 4 (44.4%) | 5 (55.6%) |
| KRAS wild (n=98) | 40 (40.8%) | 48 (59.2%) |
| NRAS wild (n=132) | 56 (42.4%) | 76 (57.6%) |
| BRAF wild (n=80) | 35 (43.7%) | 45 (56.3%) |
| Triple Wild (n=59) | 25 (42.4%) | 34 (57.6%) |
| Metastasectomy (n=23) | 11 (12%) | 12 (26.1%) |
Table 2: Patients’ medical record.
In this study, we used the SPSS 15 statistical package program to analyze the obtained data. OS was evaluated as the time between the onset of metastasis and the death of a patient because of any cause. In addition, we assessed OS using the Kaplan – Meier method and evaluated the difference in the survival time between the groups using the log-rank method. We considered P<0.05 as statistically significant.
All procedures followed the ethical standards of the responsible institutional committee on human experimentation and the 1964 Declaration of Helsinki and its later amendments. Furthermore, we obtained informed consent from all patients.
In this study, we enrolled 136 patients (median age, 75 (range: 70-83) years; 69.1% males and 30.9% females), and the median followup period was 38.5 months (95% Confidence Interval (CI): 27.8-49.2 months). The tumor histological assessment revealed that 84.6% of the tumors were adenocarcinoma, 8.8% were mucinous, and 6.6% were signet ring cell carcinoma. In addition, we analyzed the KRAS and NRAS mutations in all patients; KRAS was wild-type in 72% and mutant in 28% of patients, whereas NRAS was wild-type in 97.1% and mutant in 2.9% of patients. Of all patients, 69.1% were panRAS wildtype (KRAS and NRAS). BRAF mutation was analyzed in 82 patients (60%) but detected in only 1.5%. In addition, 59 patients (43.4%) harbored wild-type KRAS, NRAS, and BRAF (triple wild-type) mutations. When the location of tumors was considered, the tumor was located in the right colon in 14%, left colon in 58.8%, and the rectum in 27.2% of patients. All patients exhibited an ECOG performance score of 0 and 1. While 65.4% of patients were primarily operated, 29.4% received adjuvant chemotherapy, and 16.9% were metastasectomized. Considering the location of metastasis, we detected metastasis in the liver in 65.4%, lung (s) in 25.7%, peritoneum in 25%, bone in 9.6%, and ovary (s) in 1.5% of patients, whereas local recurrence was noted in 2.2% of patients. Of the 136 patients, 1, 2, 3, 4, 5, 6 and 7 lines of chemotherapy were received by 45 (33.1%), 45 (33.1%), 26 (19.1%), 5 (3.7%), 11 (8.1%), 3 (2.2%), and 1 (0.7%) patients, respectively (Table 3).
| Variable | N (%) |
|---|---|
| Median age (years) (range) | 75 (70-83) |
| Sex | |
| Male | 94 (69.1) |
| Female | 42 (30.9) |
| Histology | |
| Adenocarcinoma | 115 (84.6) |
| Mucinous | 12 (8.8) |
| Signet ring cell carcinoma | 9 (6.6) |
| KRAS wild type | 98 (72.1) |
| NRAS wild type | 132 (97.1) |
| PanRAS wild type | 94 (69.1) |
| BRAF mutated | 2 (1.5) |
| Triple wild type | 59 (43.4) |
| (KRAS, NRAS, BRAF wild type) | |
| Tumor Location | |
| Right | 19 (14) |
| Left | 80 (58.8) |
| Rectum | 37 (27.2) |
| ECOG PS 0-1 | 136 (100) |
| Surgery | |
| Primary | 89 (65.4) |
| Metastasectomy | 23 (16.9) |
| Metastasis Site | |
| Liver | 89 (65.4) |
| Lung | 35 (25.7) |
| Peritoneum | 34 (25) |
| Ovary | 2 (1.5) |
| Bone | 13 (9.6) |
| Locally Recurrent | 3 (2.2) |
| Chemotherapy Line Number | |
| 1 | 45 (33.1) |
| 2 | 45 (33.1) |
| 3 | 26 (19.1) |
| 4 | 5 (3.7) |
| 5 | 11 (8.1) |
| 6 | 3 (2.2) |
| 7 | 1 (0.7) |
| Adjuvant Chemotherapy Recipients | 40 (29.4) |
| First Line Chemotherapy | |
| 5-FU with Irinotecan | 60 (44.1) |
| 5-FU with Oxaliplatin | 74 (54.4) |
| First Line Biologic Agent | |
| Bevacizumab | 15 (11) |
| Cetuximab | 44 (32.4) |
| Cetuximab Recipients | 62 (45.6) |
| Bevacizumab Recipients | 108 (79.4) |
Table 3: Demographic characteristics of the study sample (n=136).
In this study, the median survival was 20.5 months (95% Cl: 16-25 months). The median duration of the stabilized disease was 10 months (range: 1-53 months). The assessment of the factors that affect OS revealed that the survival was 11 months for the signet ring cell histology, which was significantly shorter than that for other histological types (P=0.01). In addition, the survival was significantly prolonged in patients with a primary lesion operated on (P=0.04) and those who underwent metastasectomy (P=0.01). In patients with panRAS wild-type, OS was 23.3 months, whereas it was 15.5 months in patients with have RAS mutation although the difference was not statistically significant (P=0.10). OS was 36.7 months in triple wildtype (KRAS, NRAS, and BRAF wild-type) and 20.9 months in nontriple wild-type, and the difference was statistically significant (P=0.024). The assessment of the effect of comorbidities on the survival revealed that diabetes mellitus and hypertension did not affect OS; OS was 12 and 22 months in patients with and without coronary artery disease, respectively, and the difference was statistically significant (P=0.004).
In this study, 44.1% of patients had first received Irinotecan chemotherapy, whereas 54.4% of patients had received Oxaliplatin chemotherapy as the first line of treatment (Table 1). The median OS was 23.3 months for patients who started receiving Irinotecan, whereas the median OS was 18.1 months for patients who started receiving Oxaliplatin. However, the difference was not statistically significant (P=0.09). Furthermore, two patients received Capecitabine alone combined with a biological drug. Although 59 patients (43%) were eligible for both biological agents, 15 (11%) received Bevacizumab and 44 (32%) received Cetuximab (Table 1). The use of Bevacizumab or Cetuximab as the first line of treatment did not affect the survival. The categorization of the number of chemotherapy lines the patients received revealed that the median OS was 13.1 months for 90 patients who received one or two lines of chemotherapy, 34.1 months for 46 patients who received >2 lines of chemotherapy, and the difference was statistically significant (P=0.001) (Figure 1).
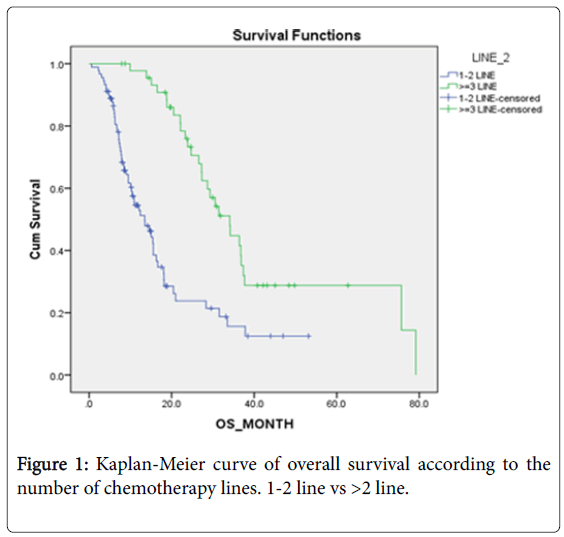
Figure 1: Kaplan-Meier curve of overall survival according to the number of chemotherapy lines. 1-2 line vs >2 line.
Of 62 patients who received Cetuximab, skin toxicity was observed in 53 (85%). Of 108 patients who received Bevacizumab, hypertension was observed in 20 (18%). Considering the adverse effects of chemotherapy, we observed myelotoxicity in 47% of patients, gastrointestinal toxicity in 20% who received Irinotecan, and neuropathy in 12% who received Oxaliplatin (Table 4). Of note, no treatment-related death was noted. At the time of documentation, 62.5% of patients had died and 37.5% were still alive.
| Variable | N (%) |
|---|---|
| Cetuximab-Panitumumab Dermatoxicity | 53 (85.5) |
| Hypertension due to Bevacizumab | 20 (18.5) |
| Myelotoxicity due to chemotherapy | 64 (47.1) |
| Diarrhea due to Irinotecan | 20 (20.6) |
| Neurotoxicity due to Oxaliplatine | 14 (12.2) |
Table 4: Side-effects of treatment.
Although CRC is an advanced age disease, the recent substantial prolongation of the survival is not proportionally reflected in the elderly population. We assume that the underlying cause in the elderly is the presence of more comorbidity, difficulty to access a medical oncologist because of lower social support, and under-treatment because of concerns about adverse effects even when placed on a medical oncological follow-up.
Ho et al. concluded that <50% of elderly patients with advanced mCRC received systemic palliative therapy [16]. The National Institute on Aging and the National Institutes of Health have grouped the elderly into the following three categories: young-old (65-75 years), old-old (76-85 years), and oldest-old (>85 years) [17]. However, in most clinical studies, the cut off value for being old is 70 years. Whether elderly patients should receive chemotherapy remains unclear to date. The estimated life expectancy, age-related physiological and functional changes, and comorbidities warrant assessment before treatment initiation. In addition, the estimated life expectancy (particularly <2 years) affects the decision of starting treatment for mCRC. The age-related loss of functional reserve in organ systems is closely associated with patients’ tolerance to chemotherapy and the benefit of treatment. Moreover, reduced kidney and liver functions, as well as cardiac and bone marrow reserves and the changes in the motility of the gastrointestinal tract, exacerbate the risk of treatment-related toxicity.
As age-related changes vary for each patient, chronological age provides limited information about patients. Thus, the review of systems should be preferred over the chronological age for elderly patients to determine the extent of benefit and the ability to tolerate the treatment. In this study, we assessed 136 patients with mCRC (age ≥ 70 years) who had an ECOG performance status score of 0 or 1 and received systemic treatment. All patients, excluding two, started treatment with combination chemotherapy. Of note, the treatment was maintained as long as the ECOG performance status score was 0 or 1. While 66.2% of patients could receive only one or two line(s) of chemotherapy ± biological drugs, 33.8% received ≥ 3 lines of treatment. The median OS was 13.1 months in patients who received one and two line(s) of chemotherapy, whereas it was 34.1 months in those who received >2 lines of chemotherapy; the difference was statistically significant (P=0.001). In addition, the median OS was 34.1 months for patients who received >2 lines of chemotherapy, which was consistent with the OS of the general population in mCRC studies.
When one or two line(s) of chemotherapy were compared with >2 lines of chemotherapy, the dramatically better survival in patients who received >2 lines of chemotherapy was questioned to determine whether patients in this group had tumors with good prognosis. No difference existed between groups regarding sex, age, histology, KRAS– NRAS–BRAF mutations, and comorbidities. In addition, metastasectomy was significantly higher in patients who received >2 lines of chemotherapy (12% vs 26.1%, P=0.04). Furthermore, metastasectomy improves survival; thus, higher metastasectomy rates in patients who received >2 lines of chemotherapy should have affected the results in this group of patients, but we think that it is not sufficient to illustrate the apparent OS difference with this finding.
When treatment-related toxicities were evaluated, myelotoxicity was observed in 47% of patients, whereas gastrointestinal toxicity was observed in 20% of patients receiving Irinotecan, and neuropathy was observed in 12% of patients who received Oxaliplatin. Of note, no treatment-related death was observed. Since the treatment was maintained only in patients who could maintain an ECOG performance score of 0 or 1, we can state that QOL did not decrease in 33.8% of patients who were eligible for the third line of the treatment. Failure to maintain treatment after the second line because of progression in these patients despite the good performance status would be a suboptimal treatment approach.
In our opinion, it will be enlightening for a common clinical dilemma whether the treatment of elderly patients should be terminated after two lines of systemic therapy. In the literature, we could not extract a single retrospective or prospective study with a similar design. As there is no randomized controlled study to reveal how many lines of chemotherapy elderly patients with mCRC should receive, we believe that our study is promising with respect to maintaining palliative systemic therapy in patients with an ECOG performance status score of 0 or 1, as it demonstrates a significant difference in survival rates.
None.
None.