Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2014) Volume 4, Issue 1
Context: Pancreatic hydatid disease is rare, occurring in less than 2% of all patients with hydatid disease. Multiple hydatid cysts of the pancreas have not been reported before.
Case report: A 63 year old lady presented with chronic epigastric pain without weight loss, vomiting or jaundice. CT scan revealed multiple small cystic pancreatic lesions. There was no extra-pancreatic disease. Endoscopic ultrasound showed 10 cysts distributed throughout the pancreas with the largest being 1.3 cm. The aspirated fluid was mucin free, low in amylase and CEA. FNAC showed refractile structures and membranous remnants consistent with a hydatid cyst. The cyst distribution would have warranted a total pancreatectomy for complete extirpation. As the cysts were uncomplicated and relatively asymptomatic, a conservative non-operative approach was chosen. She has shown symptomatic improvement and has stable disease after 6 months with Albendazole treatment.
Conclusion: Endoscopic ultrasound is useful in the diagnosis of pancreatic hydatid disease. In selected cases, non-operative management is an option that needs to be considered.
Keywords: Hydatid cyst, Pancreatic hydatid, PAIR
Hydatid cyst or cystic echinococcosis is a zoonotic disease which may affect almost any visceral or peripheral tissue. The liver and lungs act as the primary filtering beds with their vast capillary network and hence are the commonest tissues to be affected. Pancreatic hydatid cysts are rare with a reported frequency of 0.1-2% of all cases of hydatid disease [1-5]. There have been only a few case reports of pancreatic hydatid disease and all previous reports are of solitary cysts. We report a patient who presented with multiple hydatid cysts confined to the pancreas, which to the best of our knowledge is the first such report in recorded literature.
A 63 year-old lady presented with epigastric pain of many years, which had increased in frequency and severity over the previous 18 months. It was a dull pain, of mild to moderate severity, worse post-prandially, with no radiation to the back. There was no associated vomiting, loss of appetite or weight loss. There was no history of fever or jaundice. Prior to her presentation she had been given a diagnosis of irritable bowel syndrome. She had also undergone an upper and lower GI endoscopy which had shown 2 small gastric polyps which were histologically, non-functional, benign neuroendocrine tumours.
There was mild peripheral eosinophilia. Liver function tests, amylase and CA19-9 were within normal limits. A CT scan revealed small pancreatic cysts and a few calcifications in the pancreas (Figure 1). However, there was no pancreatic or biliary ductal dilatation or a mass lesion. An Endoscopic Ultrasound (EUS) showed 10 cystic lesions spread throughout the pancreas, ranging in size from a few millimetres to 1.3 cm (Figure 2). They had thin walls. Two of the larger cysts had imaging features, consistent with daughter cysts within them. There was no ductal communication. There was no pancreatic ductal dilatation and there were no parenchymal features of chronic pancreatitis. The calcifications seen on CT were in the wall of the splenic artery. EUS guided needle aspiration and cytology showed clear fluid with no mucin. It also revealed refractile structures consistent with parasitic body and membranous remnants reminiscent of a cyst wall in keeping with a hydatid cyst. The fluid CEA was low at 10.1 micrograms/l. IgG antibodies to E. granulosus tested by Enzyme-Linked Immunosorbent Assay (ELISA) were negative. A CT scan of the chest and the abdomen did not reveal hydatid cysts elsewhere in the body. The patient did not recall any close contact with dogs previously, or exposure to sheep. But she had lived in Ghana for more than 10 years, twenty seven years ago, and she might have had the exposure there.
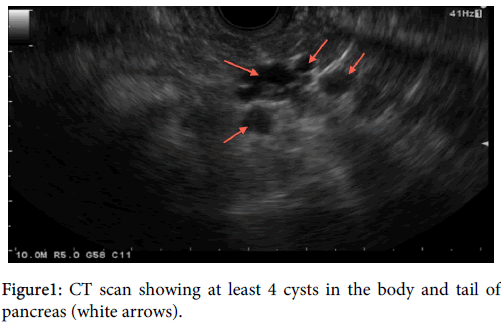
Figure 1: CT scan showing at least 4 cysts in the body and tail of pancreas (white arrows).
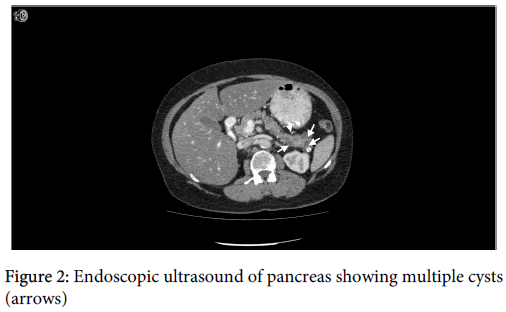
Figure 2: Endoscopic ultrasound of pancreas showing multiple cysts (arrows)
As the cysts were multiple and distributed throughout the pancreas, a complete surgical eradication of the disease burden would warrant a total pancreatectomy with or without a splenectomy. As the cysts were small and uncomplicated, it was decided to treat them medically with albendazole at the dose of 10 mg/kg/day for 6 months. She has shown symptomatic improvement on follow up and the disease has remained stable.
Echinococcusgranulosus which is the most common causes of the human hydatidosis is primarily a canine tapeworm, residing in the intestines of dogs as a short flat parasite. But it uses sheep, pigs and cows as an intermediary host, in its life cycle, taking up a cystic larval stage (hydatid) in their tissues. Man is an accidental intermediary host, suffering the infestation from dog faecal contamination [1,6]. Hydatid disease is common in farming communities where dogs have access to raw meat of the intermediary hosts, thereby sustaining the chain of transmission. Australia, South America, the Middle East, the Mediterranean countries and Wales in the United Kingdom have a high prevalence [1,6].
The first case of retroperitoneal hydatid cyst was reported by Lockhart in 1958 and the first case of primary hydatid cyst of the pancreas was published in English literature by Kattan in 1985 [7,8]. Occurring in up to 2% of all patients with hydatidosis, Pancreatichydatid cysts are commonly located in the head of pancreas (57%), followed by the body (24-34%) and the tail (16-19%) [9]. In about 90% of the patients with pancreatic hydatid, the pancreas remains the only organ affected, while 10% of patients have extra-pancreatic disease as well [10]. Although it is a disease of the young and middle aged, it is known to present in the extremes of age, with youngest reported patient to date being 3 years old [11]. The size of clinically significant pancreatic cysts varies from a few millimeters to more than a foot in diameter [12]. Hematogenous route is the most likely mode of pancreatic seeding by hydatid, but other routes such as spread via pancreaticobiliary ducts and local peripancreatic lymphatic invasion are possible [13]. Pre-operative diagnosis is not always achieved although presence of hydatid elsewhere, peripheral eosinophilia and a positive hydatid serology are useful.
The classical imaging features of hydatid cysts include a multi-vesicular cyst containing daughter cysts, ‘hydatid sand’ (layering of scolices in the cyst), ‘water lily sign’ (floating membrane within the cyst), Cyst wall calcification and hyper-intense cyst wall on plain CT [14]. The performance characteristics of the various cross sectional imaging modalities as applied to pancreatic hydatid is unknown, as most published accounts are of single cases or at best, small case series. The diagnostic sensitivity of abdominal ultrasound in abdominal echinoccosis in general ranges from 93-98% [15], but it may be less accurate with pancreatic lesions, due to the difficulty in visualisation of the pancreas. Endoscopic ultrasound provides more detailed morphological information as well as the opportunity for biochemical and cytological sampling which helps in differentiating hydatid cysts from other cystic pancreatic lesions [16].
In the case of uncomplicated cysts, the presentation is often insidious or chronic, with varying combination of symptoms including central abdominal or epigastric pain of many weeks to months, abdominal mass, early satiety, anorexia, and vomiting and weight loss.
Complicated cysts may have a more acute or subacute presentation. This includes obstructive jaundice from head of pancreas lesions [4,17,18]; duodenal stenosis; duodenal fistula [3]; pancreatic abscess [19]; variceal bleeding from sinistral portal hypertension consequent to splenic vein thrombosis [3]; anaphylactic shock from rupture; sepsis from secondary infection; acute pancreatitis (9 case reports to date) [10,20,21]; chronic pancreatitis and symptomatic cysto-enteric fistula [3,5,22].
The surgical options for management of pancreatic hydatid are enucleation, partial cystectomy with or without a drainage procedure (cystoenterostomy) and pancreatic resection (Pancreaticoduodenectomy, segmental resection, distal pancreatectomy or total pancreatectomy). The size, location and presence of communication with the main pancreatic duct, determines the choice of procedure. Splenic conservation should be the goal whenever possible. Spillage of cyst contents, with viable scolices, into the abdominal cavity carries a risk of anaphylaxis, dissemination and recurrence of hydatid. Various scolicidal agents such as hypertonic saline, cetrimide, betadine, EUSOL and silver nitrate have been used in sterilising the cysts peroperatively. Use of packs soaked with the scolicidal agents to cover the immediate operative field, is also a common prophylactic measure to minimise the effects of any potential spill.
Filice et al. described a Percutaneous technique of image guided targeted alcohol injection and aspiration of hepatic hydatid [23]. This method has since been refined and the PAIR technique of Puncture Aspiration Injection and Re-Aspiration is a standard practice for hepatic hydatid. Currently, there is only one reported instance of a successful use of PAIR technique for pancreatic hydatid [2]. Karaman et al. have recently reported a percutaneous catheter drainage technique in a patient with pancreatic hydatid, which they claim has the added advantage of draining the cyst contents better than needle aspiration alone [24].
The differential diagnosis of a pancreatic hydatid cyst should include the more common lesions such as pancreatic pseudocyst; serous cystadenoma; mucinous cystadenoma; Intraductal pancreatic mucinous neoplasm (IPMN); cystic pancreatic metastasis and pancreatic lymphangioma. Morphological features on EUS combined with cytology and biochemistry of the cyst fluid is successful in achieving an accurate diagnosis in the vast majority of patients.
Pancreatic hydatid disease although a rarity, is important because it enters the differential diagnosis of a much more common clinical problem of cystic pancreatic lesions. Endoscopic ultrasound with its capabilities for fluid sampling for biochemistry and cytology is a very useful discriminant. In selected patients, as the one presented here, there is a role for non-surgical management.