Medicinal & Aromatic Plants
Open Access
ISSN: 2167-0412
ISSN: 2167-0412
Research Article - (2015) Volume 0, Issue 0
Pathophysiology of spinal cord injury has classically bad prognosis in primary and secondary processes. This process causes inflammation, deformity and cell loss. It has been shown that Melissa officinalis is a useful herbal plant in the prevention of various neurological diseases. The present study evaluated the effects of three doses of Melissa officinalis on spinal cord injury. Thirty five adult male wistar rats were used in this study. The weight-drop contusion method was employed to induce spinal cord injury in rats. Three doses of Melissa officinalis (50, 100 and 150 mg/kg) were intraperitoneally injected once a day for 14 days in all treatment groups and all injections started one day after injury. After neurological and electrophysiological evaluations, rats were sacrificed for histological and immunohistochemistry assessments. Our results showed motor function was improved in groups received 100 and 150 mg/kg of Melissa officinalis and sensory recovery was better in 150 mg/kg of Melissa officinalis treated group compared to spinal cord injury group (p<0. 01, p<0. 001 respectively). Mean cavity area in 100 and 150 mg/kg (p<0. 01) significantly decreased compared to spinal cord injury group. In addition, three doses of Melissa officinalis considerably prevented loss of lower motor neurons in the ventral horn of spinal cord (p<0. 05, p<0. 01). Also, Melissa officinalis (100 and 150 mg/kg) prevented of astrogliosis effectively (p<0. 01). Furthermore, the findings showed a significant augmentation of EMG recruitment index in groups which treated by 100 mg/ kg (P <0. 01) and 150 mg/ kg (P <0. 001) of Melissa officialis. The results showed that Melissa Officinalis could be considered as a neuroprotective agent in spinal cord injury.
Spinal cord injury (SCI) causes severe damage to function of motor and sensory neurons and may leads to paraplegia and tetraplegia [1]. Overall prognosis of pathology of SCI is poor. SCI pathophysiology is a biphasic procedure includes primary and secondary processes. The primary process is related to physical deformation and energy deprivation, while the secondary process involves cascades of biological and cellular processes which more often triggered by the primary process [2]. Astrogliosis is an important cellular response to SCI, in which, axonal regeneration is prevented by a barrier. Marked up regulation of glial fibrillary acidic protein (GFAP) is principal biomarker for this process [3]. Therapeutic strategies aim at attenuation of astrogliosis during the initial phase after SCI [4].
Various therapeutic approaches are now accessible for SCI, but many of them are expensive and lead to various side effects [5]. Therefore, there have been some interests to finding natural agents in order to prevention of the inflammation and degeneration of neural cells after SCI [6]. Melissa officinalis (MO) usually known as lemon balm (family: Lamiaceae) is one of the oldest and still most popular medicinal plants. The leaves of MO have been used traditionally to prepare tea in order to calming and anti-spasmolytic effects [7]. Pharmacological investigations have shown that the most commonly known therapeutic properties of MO extract are sedative, carminative, antispasmodic, antibacterial, antiviral, anti-inflammatory, antioxidant, and neuroprotective [7]. Chemical constituents with antioxidative activity can be found at high concentrations in this plant, and can be responsible for its preventive effects in various degenerative conditions [8] such as ischemic brain injury [9] and Alzheimer disease [10]. Hassanzadeh et al. have reported that aqueous extract of MO can provide neuroprotection against ecstasy induced neurotoxicity in hippocampal primary culture [11]. In addition, it has been reported that oral administration of MO can increase cell proliferation and differentiation by decreasing serum corticosterone levels and also by increasing GABA levels in the mouse dentate gyrus [12]. This study aimed to evaluate the effects of MO in preventing harmful effects which triggered by neural damage, and also it can promote neurological functions after SCI.
Animals
After obtaining the approval of the Institutional Review Board of our university, all experiments were carried out in accordance with the Guidelines of the Animal Care and use ethics committee of Baqiyatallah University of medical sciences. Thirty five adult male wistar rats weighting 190-220 g were maintained under standard laboratory conditions. Animals were housed in an environment of 21 ± 2°C with a relative humidity of 50-10% and a 12-h light- dark cycle. Food and water were always available.
Surgical procedure for SCI
In order to making SCI the animals were anesthetized with 80 mg/kg ketamine hydrochloride and 10 mg/kg xylazine hydrochloride intraperitoneally. Weight-drop contusion method was conducted to induce SCI in rats. The skin and subcutaneous tissues in the thoracolumbar T12-L1 region were incised. The paravertebral muscle fascia was penetrated, and muscles were peeled laterally using blunt dissection forceps. The spinal cord segment at T12-L1 level was exposed by total laminectomy. The animals were subjected to an impact of 10 g weight (stainless steel rod, 3 mm diameter tip) dropped vertically in the center of the exposed spinal cord from the height of 25 mm. In sham group, all mentioned procedures were carried out, except the spinal cord contusion. The final procedure was incision suturing [13].
Core body temperature of animals was maintained at 36.5-37.5°C during and after the study procedures. The rats were treated with gentamicin (40 mg/kg, intramuscular injection) twice a day for the first 3 days as prophylaxis against urinary tract infection. The urinary bladders were pressed three times a day until bladder function returned to normal. The rats were also injected subcutaneously with 25 ml/kg lactated Ringer’s for a couple of days after SCI as once a day [14].
Plant collection and extractions: The plant was obtained from commercial source. The dried leaves powder of MO was macerated at room temperature in 70% ethanol (1 g/10 ml) and extracted for a week. On the seventh day, the ethanolic extract was filtered and the extract was evaporated under reduced pressure to remove the ethanol. The dry extract was suspended in the normal saline and thus alcoholic extract of MO, at minimum (50 mg/kg), moderate (100 mg/kg), and maximum (150 mg/kg) doses were prepared [8].
Animal groups and MO administration
Rats were randomly divided into six groups as follows: Group І: intact group (n=5), group ІІ: sham rats were subjected to laminectomy without SCI (n=5), group ІІІ: Rats were subjected to laminectomy and SCI (n=5), group ІV: Rats were subjected to laminectomy, SCI and treated with 50 mg/kg MO (SCI-M50) (n=6), group V: Rats were subjected to laminectomy, SCI and treated with 100 mg/kg MO (SCI-M100) (n=7). Group VІ: Rats were subjected to laminectomy, SCI and treated with 150 mg/kg MO (SCI-M150) (n=7). MO was daily injected intraperitoneally into treatment rat groups starting 1 day after injury for 14 days.
Neurological examination
For assessment of neurological function the Basso-Beattie- Bresnahan (BBB) scale was used for open field motor testing in all rat groups. The BBB scale is a 21 point scale ranging from zero to 21 [15], rating locomotion on aspects of hind limb function such as weight support, stepping ability, coordination and toe clearance [13]. All functional scores were obtained on days 1, 7, 14, 21, 28, 35, 42, 49 and 56 by two investigators blinded to group identity. The final score of each animal was the mean value of both examiners.
Behavioral tests were performed for evaluating pain by means of hot water test for the hind limbs after SCI (scores were obtained on days 1, 7, 14, 21, 28, 35, 42, 49 and 56). The response to heat stimulation was measured by the latency of hind limb paw withdrawal to hot water of 50°C. Both paws of rats were placed in a hot water container respectively. Six trials obtained for each rat (3 trial for each paw), and average of this trials were recorded, and non-responders were removed from the hot water container after 60 Sec [16].
Electrophysiological evaluations
Electromyographic activity is associated with spontaneous functional recovery after SCI in rats. EMG recorded as an index of recovery of recruitment patterns of muscular units. Spontaneous rest activity was bilaterally recorded from flexor muscles of hind limb. One day prior to sacrifice of animals EMG recording was done by 23 gauge needles for 10 seconds. The EMG signal was amplified (Grass, Astro- Med Inc., West Warwick, RI, USA), digitized (5 kHz, Digi-data 1322A; Axon instruments, Foster City, CA, USA), and filtered (30–300Hz) [17]. After recording, 10 seconds of recording were compressed to 1 second by EMG software in order to acquire recruitment index of motor units. Quantitative assessment of spontaneous activity was scored on an ordinal scale, for instance 0 to ++++[18].
Histology and immunohistochemistry
On day 57, all rats were anesthetized with an intraperitoneal injection of 100 mg/kg sodium pentobarbital and intracardially perfused with 0.9% saline followed by 10% buffered formalin. A spinal cord segment at the level of T12-L1 was dissected, post-fixed in 10% buffered formalin overnight, cryoprotected in 30% sucrose for 48 h and were sectioned serially in the transverse plane, using a cryostat (B1155800 sakura) at 10 μm thickness. All sections were processed for hematoxylin and eosin staining and examined under light microscopy [13]. Standard immunocytochemistry for the glial scar (glial fibrillary acidic protein) was performed for all of the sections. Briefly, sections from formalin- fixed, paraffin embedded spinal cord tissues were dewaxed, rehydrated, and retrieval of antigens was performed. After incubation with 3% H2O2 in ethanol, and then normal non-immune goat serum, the sections were incubated with rabbit anti-active GFAP polyclonal antibody at a dilution of 1:200 at 4°C, followed by biotinylated goat anti-rabbit IgG for 20 min at room temperature, and subsequently incubated with streptavidin–peroxidase. PBS replaced primary antibody as the negative control. DAB chromogen was applied for visualization of peroxidase activity. Finally, the sections were counterstained with hematoxylin [19].
Morphometric analysis
The lesion area, including the cavity and surrounding damaged tissue was then measured by using an image analyzing software (Motic 2.1, Italy, Cagli). In addition, the number of lower motor neurons and the number of positive GFAP astrocyte perikaryons in ventral horn were measured. Five sections from each case were counted, and mean values were obtained for each animal. Only those cells that showed clearly discernible nucleus were counted. Cell counting analyses were carried out by two observers who were blind to the specific experimental conditions of the analyzed tissues on images acquired at 40x and 400x magnifications [3].
Statistical analyses
Data obtained from motor and sensory functions at each time point and electromyographic activity between different groups were analyzed using two-way analyses of variance (ANOVA). The histomorphometric and immunostaining data were analyzed using one-way analyses of variance (ANOVA). In both tests, ANOVA was followed by Post Hoc Bonferroni’s multiple comparison tests. Data have been presented as the mean ± SEM. A significance level of 0.05 was predetermined for all statistical analyses.
In all experiments there were no significant differences between sham and intact groups. Furthermore, significant differences have been shown between intact and SCI groups (p< 0. 001) in all experiments. Indeed, this significance was main index for SCI model induction.
Neurological function results
Melissa Officinalis extracts improve motor function after Spinal Cord Injury: In order to evaluation of effect of MO treatment on motor function Basso-Beattie-Bresnahan (BBB) was measured. While SCI resulted in immediate paraplegia (loss of hind limb movement), the SCI group showed significant decrease in locomotion scores in comparison with intact group. Application of two-way ANOVA showed a significant interaction between variables such as MO treatment (50, 100, 150 mg/kg), and days [F (5, 29) =8. 543, p=. 000]. An application of post-hoc Bonferroni’s multiple comparison test revealed significant improvement in motor function following MO treatment on all test days except 1th day, post-injury in dose 100mg/kg (p<0.001) and revealed significant improvement on day 28, 35, 42 (p<0. 01), 49 and 56 (p<0. 001) for dose 150 mg/kg. MO in 50 mg/kg was not significant (Figure 1).

Figure 1: Effect of Melissa officinalis (MO) treatment on motor function after SCI. Three different doses of MO (50, 100, 150 mg/kg) were injected (once a day, i.p.) for 14 days after injury. Data are represented as mean of BBB score ± SEM, (n=5-7) and analyzed by two way ANOVA followed by post-hoc Bonferroni’s multiple comparison test. ***P<0. 001 versus intact. ##P<0. 01 and ###P<0. 001 versus spinal cord injury.
Melissa Officinalis extracts increase sensory Function after SCI: Statistical evaluations revealed that the mean of latency time of response to painful stimulus (50°c water) was significantly decreased in 150 mg/kg MO treatment group compared to SCI group. Two-way ANOVA showed a significant interaction between variables such as MO treatment (50, 100, 150 mg/kg), and days [F (5, 29) = 5. 482, p =0.000]. Application of post-hoc Bonferroni’s multiple comparison test revealed significant improvement in sensory function following MO treatment. Although MO in 50 and 100 mg/kg was not significant, 150 mg/kg was significant on days 35 (p<0. 01), 42, 49 and 56 (p<0. 001) on post-injury. In the other word, the best sensory recovery was shown in the 150 mg/kg MO treated group (Figure 2).

Figure 2: Effect of Melissa officinalis (MO) treatment on sensory function after SCI. Three different doses of MO (50, 100, 150 mg/kg) were injected (once a day, i.p.) for 14 days after injury. Data are represented as mean of latency time ± SEM, (n=5-7) and analyzed by two - way ANOVA followed by post-hoc Bonferroni’s multiple comparison test. ***P<0. 001 versus intact. #P<0. 05 and ###P<0. 001 versus spinal cord injury.
Histological results
Melissa Officinalis extracts decrease cavity formation after Spinal Cord Injury: One of the most important problems after spinal cord injury is the formation of cavity. It is a serious obstruction against the regeneration of axons from proximal to distal segment of the injury. Spinal cord segments from the intact group showed undamaged white and gray matter. Statistical evaluations revealed that the mean of cavity size in term of μm2 was significantly reduced in MO treatment groups. Application of one-way ANOVA showed significant differences between SCI and MO-treated SCI groups [F (5, 29) =27. 69, p=0. 000]. Also post-hoc Bonferroni’s multiple comparison test illustrated significant decrease in mean cavity area in 100 and 150 mg/kg (p<0. 01). Although, the mean cavity area decreased in 50 mg/kg of MO compared to SCI group, however, this difference was not significant (Figure 3).

Figure 3: Effect of Melissa officinalis (MO) treatment on cavity formation after SCI. Three different doses of MO (50, 100, 150 mg/kg) were injected (once a day, i.p.) for 14 days after injury. Data are represented as mean of cavity area ± SEM, (n=5-7) and analyzed by one- way ANOVA followed by post-hoc Bonferroni’s multiple comparison test. ***P<0. 001 versus intact. ##P<0. 01 versus spinal cord injury.
Melissa Officinalis extracts prevent loosening of motor neuron cells in ventral horn of spinal cord after its Injury: Statistical evaluations revealed that MO treatment prevented cell loss significantly in comparisons with SCI group. Application of one-way ANOVA showed significant differences between SCI and MO-treated SCI groups [F (5, 29) =42. 38, p=0.000]. And post-hoc Bonferroni’s multiple comparison test illustrated that all three doses of MO includes 50, 100, and 150 mg/kg (p< 0. 05, p< 0. 01) prevented cell loss significantly (Figure 4).

Figure 4: Effect of Melissa officinalis (MO) treatment on cell loss in ventral horn of spinal cord after injury. Three different doses of MO (50, 100, 150 mg/kg) were injected (once a day, i.p.) for 14 days after injury. Data are represented as mean of number of ventral horn motor neurons ± SEM (n=5-7) and analyzed by one- way ANOVA followed by post-hoc Bonferroni’s multiple comparison test. ***P<0. 001 versus intact. #P< 0. 05 and ##P<0. 01 versus spinal cord injury.
Immunohistochemistry results
Melissa Officinalis extracts inhibit the formation of astrogliosis after SCI: Statistical evaluations showed that MO treatment prevented formation of astrogliosis in the ventral horn of spinal cord significantly in comparisons with SCI group. Application of one-way ANOVA showed significant differences between SCI and MO-treated SCI groups [F (5, 29) =20. 80, p=0. 000]. In addition, post-hoc Bonferroni’s multiple comparison test revealed that astrogliosis significantly decreased in 100 and 150 mg/kg of MO compared to SCI group, however the difference was not significant at 50 mg/kg of MO compared to SCI group (p<0. 01) (Figure 5).
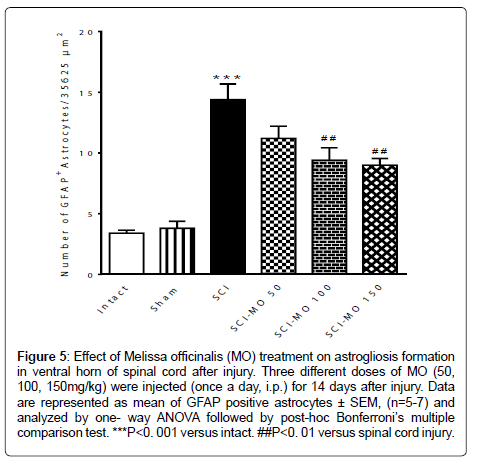
Figure 5: Effect of Melissa officinalis (MO) treatment on astrogliosis formation in ventral horn of spinal cord after injury. Three different doses of MO (50, 100, 150mg/kg) were injected (once a day, i.p.) for 14 days after injury. Data are represented as mean of GFAP positive astrocytes ± SEM, (n=5-7) and analyzed by one- way ANOVA followed by post-hoc Bonferroni’s multiple comparison test. ***P<0. 001 versus intact. ##P<0. 01 versus spinal cord injury.
Electrophysiological results
Melissa Officinalis extracts improve hind limbs EMG: By application of two-way ANOVA although, no significant difference between right and left hind limb had shown, MO treatment was significant [F (5, 29) =56. 71, p=0. 000]. An application of post-hoc Bonferroni’s multiple comparison test showed significant augmentation of EMG signals following MO treatment in doses of 100 mg/kg (p<0. 01) and 150mg/kg (p<0. 001) (Figure 6).
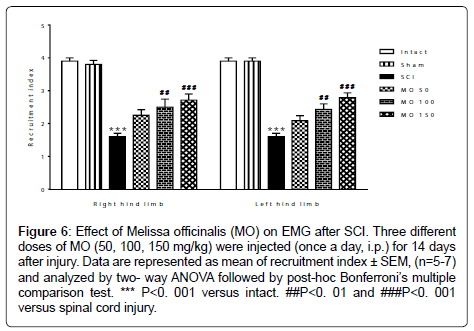
Figure 6: Effect of Melissa officinalis (MO) on EMG after SCI. Three different doses of MO (50, 100, 150 mg/kg) were injected (once a day, i.p.) for 14 days after injury. Data are represented as mean of recruitment index ± SEM, (n=5-7) and analyzed by two- way ANOVA followed by post-hoc Bonferroni’s multiple comparison test. *** P<0. 001 versus intact. ##P<0. 01 and ###P<0. 001 versus spinal cord injury.
The aim of present study was to investigation of neuroprotective effect of Melissa officinalis in spinal cord injury. In this study, weightdrop contusion method was used to make SCI at T12-L1 level of spinal cord. This process causes gliosis, connective tissue deposition, demyelination, and cysts formation [3]. Our observation based on loosening of tissue and formation of cavity in white and gray matter was agree with previously studies [20,21]. We also showed that, within 1 day after SCI, the rats were paraplegic and unable to walk on the hind limb. One purpose of the study was to examine the effect of MO on neurological functions in SCI. The results showed that MO could promote the motor and sensory functions significantly. One possible explanation for this improvement is that MO has an acetilcolinestrase inhibitory property [22], anticholinesteras increases the residence time of acetylcholine in the synapse. So, this allows rebinding of the transmitter to nicotinic receptors. It thus gives acetylcholine the competitive advantage over the neuromuscular blocking agent [23]. Findings have shown that MO has neuroprotective effect on ischemic damage mediated by the inhibition of oxidative stress, followed by the inhibition of apoptosis [9]. Oxidative stress is a hallmark of injury of SCI that result in disruption of spinal neuronal ion homeostasis, mitochondrial dysfunction, enhancement of glutamate-mediated excitotoxicity, and microvascular perfusion deficits [24].
Therefore, alleviating oxidative stress may be an effective way for treatment of SCI. MO has powerful antioxidant effects and these effects probably are exerted through the rosmarinic acid and the benzodioxole present in the extract. In addition, compounds such as acid linoleic acid and carnosic acid are also present in the extract all of which have antioxidant properties [22]. So, another possible explanation for the improvement of neurological functions by MO is the antioxidant properties of this plant.
In the present study, three doses of Melissa officinalis which were injected Intra Peritoneal 1 day after injury for 14 days, resulted in positive effect on recruitment of motor units in spinal cord and then on locomotor recovery at all the time points. In addition, we found that the positive effect of MO on recovery of neurological functions was not dose dependent. Although, our findings revealed a causal relationship between MO and neuroprotection, the involvement of other endogenous factors cannot be ruled out.
Inflammatory responses play an important role in regulating of the pathogenesis of acute and chronic SCI, and seems to play a fundamental role in nerve injury and contribute to the control of the regenerative response [25]. Inflammation can leads to the loss of cells as well as scar formation and finally in the reduction of neuronal function [26]. The present results showed that the MO can reduce cell loss as well as scar formation and then improve the sensory and motor functions. One possible explanation for this is that MO has anti-inflammation property, which has also been observed in the previous study [27]. Its anti-inflammatory effects are due to rosmarinic acid and flavonoids and terpenoids present in the extract. Probably flavonoids have more effective role by facilitating prostaglandin synthesis [27].
Another purpose of the study was to examine the inhibition of astrogliosis by MO. Findings showed that MO significantly decreased GFAP+ astrocytes in comparison with SCI group. Reactive astrogliosis is a cellular response associated with injury of the nervous system. It is the activation of astrocytes and precursor that play pro-inflammatory role in the lesion site that form barrier to axonal regeneration. As a result, the inhibition of astrogliosis formation can help to promote axonal regeneration and neurological functions after SCI. Decreasing of GFAP+ astrocytes may be related to inhibition of pro-inflammatory cytokines and reactive oxygen species (ROS) by MO, which two these factors are key mediators of reactive astrogliosis in SCI [3].
SCI causes motor and sensory dysfunction, tissue destruction, and cell death, formation of astrogliosis and degeneration of axons. The present results indicate that MO treatment promotes the locomotor and sensory recovery and also reduces formation of astrogliosis, cell death and structural destruction in spinal cord injury. Since MO offers neuroprotection, probably by anti-oxidative and anti-inflammative properties, the potentials of this herbal as a candidate with therapeutic applications in SCI can be suggested.
The authors would like to thank from Neuroscience Research Center of Baqiyatallah University of Medical Sciences for supporting this research.