Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2017) Volume 6, Issue 4
Background: TSH assays have long been showing discordances, especially in the upper limit of the reference range. There is thus a need to improve TSH measurement and detection of thyroid dysfunction. This study aimed at evaluating the ability of new TSH assays to detect early thyroid deficiency in a healthy population with no suspicion of thyroid disorders.
Methods: We selected 797 subjects without declared hyperthyroidism, hypothyroidism, goiter, personal or familial thyroid dysfunction, thyroid autoimmunity or medication among 1,623 individuals recruited in a multicenter prospective study (2012-2014). Hypothyroidism-related clinical signs (hCS) were collected, TSH and thyroid hormones levels measured by routine tests and 4 new assays based on calibration with a biologically active recombinant TSH. Analysis was performed as a function of gender and age (<60 y and ≥ 60 y).
Results: Expression of hCS appeared to vary as a function of gender and age in healthy individuals. The cohort displayed a higher percentage of males with no hCS in both <60 y (45.9%) and ≥ 60 y (33.9%) but a high percentage of females with at least 3 hCS in both <60y (29.7%) and ≥ 60y age groups (39.7%). FT3 and FT4 levels were different in males and females <60 y (p<0.05 and p<0.01 respectively) in contrast to TSH values. When we analyzed the population with elevated TSH (>97.5th centile), FT4 levels were found to be slightly reduced and the expression of hCS increased (median, 2.0 vs. 1.0) when TSH was measured by the new assays compared to the routine assay. Detection of subclinical TSH was particularly improved in elderly women.
Conclusion: New assays measuring bioactive TSH exhibited a good correlation with expression of hCS and FT4 levels, especially in ≥ 60 y women. Such assays may improve the monitoring of elderly people as well as the whole healthy population, especially in the context of environmental hazards.
<Keywords: TSH immunoassays; Bioactive TSH; Recombinant TSH; Hypothyroidism; Thyroid disorders
AACE: American Association of Clinical Endocrinologists; BSA: Bovine Serum Albumin; CHO: Chinese Hamster Ovary cells; FT3: free triiodothyronine; FT4: free thyroxine; GalNAc: N-acetylgalactosamine; HAMA: Human Anti-Mouse Antibodies; hCS: hypothyroidismrelated clinical signs; IFCC: International Federation of Clinical Chemistry; IQR: InterQuartile Range; IS: International Standard; mAbs: monoclonal antibodies; NACB: National Academy of Chemical Biochemistry; recTSH: recombinant Thyroid-Stimulating Hormone; rgTSH: recombinant glycoengineered Thyroid-Stimulating Hormone; SCH: subclinical hypothyroidism; T3: triiodothyronine; T4: thyroxine; TPO: thyroperoxidase; TPOAbs: anti-thyroperoxidase antibodies; TSH, Thyroid-Stimulating Hormone; y: years
Clinical evaluation of thyroid deficiency
Hypothyroidism also called Underactive Thyroid is a very common deficiency of the thyroid in which the endocrine gland does not produce sufficient amount of thyroid hormones (T3 and T4). Diagnosing hypothyroidism early enough should provide rapid access to treatment and have a positive impact on the daily life of the population. Since the concentration of TSH may increase by a factor of 100 when the concentration of FT4 is only reduced by a factor 2 [1], TSH is a much more informative than FT4 and is defined as the first-line marker of thyroid deficiency. When TSH level is beyond the upper limit of the reference range, hypothyroidism may be envisaged. Assessment of FT4 level will then determine the biological significance of this dysfunction [2]. Therapy with levothyroxine will be usually considered for patients with a persistent serum TSH level of more than 8 mIU/L [3].
In 1-11% of cases, moderately elevated TSH levels remain associated with normal values of FT4. This frequent situation is recognized as SCH [4-10] and has been depicted as the most common thyroid dysfunction in aging [11]. 80% of the patients with SCH display a serum TSH <10 mIU/L [3]and management of these patients will then rely on individual factors including anti-TPO antibodies, symptoms of hypothyroidism, atherosclerotic cardiovascular disease or heart failure [3,12].
Calibration of TSH immunoassays
Discrepancies among TSH measurements have been observed through all the generations of assays and extensively debated over the past decades [13-15]. Today, (41-55)% of assays still present unacceptable analytic bias and there is both a clinical and a regulatory need for ensuring that different TSH assays deliver similar values [15]. Previous work of our laboratory pointed out that calibration together with the epitope specificity of anti-TSH antibodies may explain such broad variations [13,15-17].
TSH is a glycoprotein hormone in which glycosylation governs altogether the immunological behavior, bioactivity and serum half-life [18]. The current 3rd IS 81/565 primary calibrator has been extracted from pituitaries and is mainly composed of GalNAc-sulfated glycoforms that are biosynthetic intermediates of low biopotency [16]. Indeed, such glycoforms are rapidly cleared from the circulation by a liver GalNAcsulfate lectin receptor [19] leaving in the circulation essentially longlived sialylated TSH forms [20-22] which escape hepatic clearance [23]. Previous studies of our laboratory [16,17,24,25] as well as those of others [26,27] have shown that the binding of anti-TSH antibodies may be altered by changes in TSH glycosylation. The lack of immunological similarity between immunoreactive TSH present in the calibrator and in clinical samples has been shown to impact TSH measurements [16]. Highly sialylated recombinant TSH however proved to display immunological identity with serum TSH, especially from hypothyroid patients [17]. Recently, we could demonstrate that combining a defined selection of TSH epitopes to a calibration based on glycoengineered TSH is able to abolish discrepancies among assays and achieve harmonization of TSH values as now requested by regulatory bodies [28].
Upper limit of the reference range for TSH values
The distribution of serum TSH concentrations in euthyroid patients without clinical signs of thyroid dysfunction reveals a relatively long “tail” to the highest values [29] often explained by high values of TSH in patients recovering from non-thyroid pathologies (meningitis, head trauma or curative treatments based on interferons, iodine or lithium), TSH-receptor polymorphism (TSH variable sensitivity), rare inactive TSH or occult autoimmune thyroid dysfunction [30]. The distribution becomes Gaussian after logarithmic transformation. The 95% reference interval is determined, thus defining the low and upper limits i.e. 2.5th and 97.5th centile respectively.
The current upper limit of 4.12 mIU/L largely based on NHANES III data [5] has not been universally accepted [12]. Some authors have proposed that it should be decreased to either 3.0 mIU/L (AACE) [31] or 2.5 mIU/L (NACB) [32] arguing that the current 4.12 mIU/L value was influenced by the inclusion of individuals with underlying factors such as occult autoimmune thyroid disease [33], a possible interfering medication, a family predisposition to thyroid diseases or pregnancy [34]. The NACB then defined rigorous selection criteria to establish TSH reference intervals: at least 120 rigorously screened normal euthyroid volunteers who have no detectable thyroid autoantibodies, anti-TPO or anti-thyroglobulin antibodies, no personal or family history of thyroid dysfunction, no visible or palpable goiter, no medications (except estrogen) and no pregnancy [32]. Despite these strict criteria, variable upper limit values ranged from 2.12 mIU/L to 5.28 mIU/L [35]. These findings could nevertheless be influenced by variable assays and ethnic origins.
Manufacturers indicate a variable upper limit for TSH values (Roche Elecsys: 4.20 mIU/L; Abbott AxSYM 4.64 mIU/L; Siemens ADVIA Centaur: 4.78 mIU/L; Beckman Access: 3.50 mIU/L; Ortho Clinical Diagnostics Vitros: 4.68 mIU/L) and recommend for each laboratory to establish its own reference interval more adapted to the local population [36]. Today, only 10% of laboratories use their own reference interval, 60% a “suitable” interval and the remaining 30% apply the value indicated by the manufacturer [37]. Recruitment of the adequate number of healthy people representative of the local population as well as the cost of the study remain limiting for the laboratory medicine and the references provided by the manufacturer or established by another laboratory remain most often in use [38]. As a result, standardization of TSH assays has been now requested by regulatory bodies.
Aim of the study
To get a novel insight into the variation of TSH levels, we have explored clinical and biological parameters of a cohort of healthy individuals as a function of gender and age using newly designed assays. We also analyzed the correlation between hCS expression and FT4 levels in individuals detected with elevated TSH levels (i.e. TSH >97.5th centile of the cohort) to establish if early SCH detection could be better diagnosed by these assays based on the measurement of bioactive TSH.
Selection of the healthy cohort
The clinical study was agreed by the Committee of Protection of the People and registered at ClinicalTrials.gov (NCT01997554). This study has also been cleared by the local Institution Ethics Review Board for human studies. Serum samples were obtained at the time of inclusion (no follow-up). Each serum sample was tested for TSH (IRMA Beckman-Coulter, IM3712-IM3713, reference range: 0.17-4.05 mIU/L), FT4 (IM1363, Beckman Coulter), FT3 (IM1579, Beckman Coulter) and anti TPO antibodies (RIA, ThermoFisher Scientific B.R.A.H.M.S). Age, sex, medical treatments as well as the absence/presence of hCS were reported for each patient as described by Zulewski and colleagues [39]. Our study did not include the ankle reflex for practical questions, and was based on the analysis on 11 other hCS. The presence or absence of each hCS was recorded by clinicians to limit biases due to self-reporting by subjects
Figure 1 shows our process to recruit healthy subjects in the Departments of Endocrinology and Geriatrics of the Lyon Sud Hospital, and in the Departments of Endocrinology and Nuclear Medicine of the Chambery Hospital (France). In this study, the healthy status of participants was based on NACB recommendations (exclusion of hyperthyroid, hypothyroid, goiter, personal or familial thyroid dysfunction, thyroid auto-immunity and medication). The cohort was finally based on 797 individuals and was equally distributed among males and females.
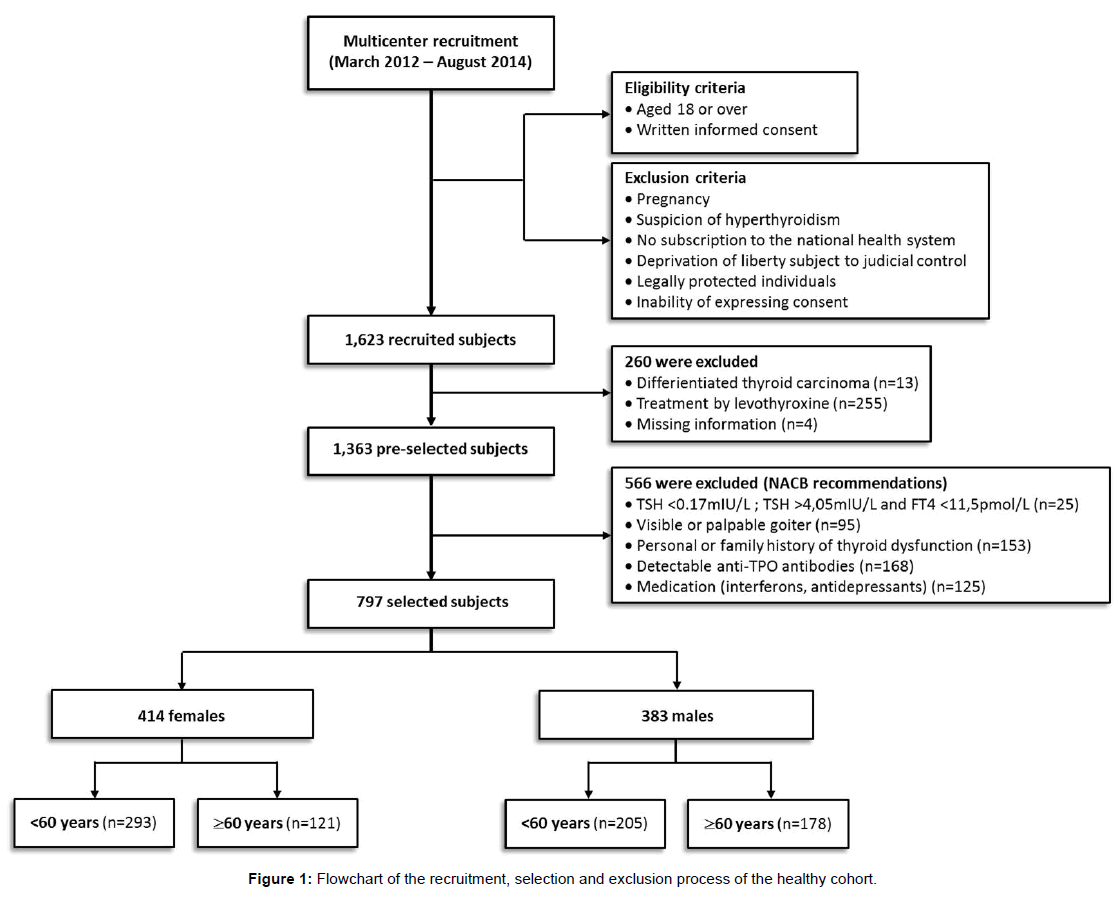
Figure 1: Flowchart of the recruitment, selection and exclusion process of the healthy cohort.
TSH measurements with the new assays
Calibration-A recombinant glycoengineered hormone (rgTSH) has been produced by cotransfection of the α- and β-TSH genes in a CHO cell line expressing a highly active sialyltransferases [40]. Stably triply transfected clones have been selected and rgTSH producedin a chemically defined medium (Life Technologies).Mass estimation of rgTSH was carried out by Amino Acid Analysis (Alphalyse) of a purified recombinant preparation followed by immunological assessment. rgTSH bioactivity has been measured in CHO cells expressing the recombinant human TSH-receptor and was found 3-fold more active than a commercial preparation in stimulating cAMP production [28].
Assays procedure - Anti-TSH mAbs were coated on microplates and further incubated with TSH samples supplemented with a 50 mM phosphate buffer pH7.5 containing 5% BSA and a HAMA blocking reagent (Fitzgerald Industries International) to avoid interferences with circulating antibodies. Bound TSH was revealed with inhouse biotinylated (Roche) anti-TSH mAbs and HRP-streptavidin (ThermoFisher Scientific). Detection was performed with UltraTMB (ThermoFisher Scientific). Optical density was measured at 450 nm (Biochrom). TSH concentrations were determined on standard curves based on 6 values in duplicates (4-PL model).
Data collection
Demographical, clinical and biological data were entered in specifically designed Case Report Forms by the Clinical Research Assistant in charge of this study. The presence of correctly filled consent forms for all enrolled patients was followed by periodic and exhaustive monitoring by the HCL-DRCI law Department. The elaboration of an electronic database was outsourced to a private company (ClinInfo).
Statistical analysis
Measures of significance between groups were calculated using analysis of variance (ANOVA). Calculations were performed using Analysis ToolPak (Microsoft Excel add-in program).
Expression of hCS in the healthy cohort
Expression of overall hCS - Males and females appeared to express a distinct expression pattern of hCS. Most of males exhibited no sign (40.3%) (Figure 2A) but females conversely presented at least 3 hCS (32.6%) (Figure 2D). When the distribution of these signs was analyzed as a function of age, a striking difference was found between the two genders. Indeed, the percentage of males with no sign decreased progressively until ≥ 80y group (from 57.7% to 18.8%, for age groups ≤ 29 y and ≥ 80 y respectively) while the percentage of males with 2 hCS steadily increased from 19.2% to 46.9%, for age groups ≤ 29 y and ≥ 80 y respectively. The percentage of males with at least 3 hCS also increased until (70-79) y group (from 11.5% to 31.4%, for age groups ≤ 29 y and (70-79) y respectively) (Figure 2B). In contrast, the percentage of females with at least 3 signs remained relatively elevated over years ((30.2-45.3)% compared to (12.7-30.2)% with no signs) (Figure 2E) except for age groups ≤ 29 y and 70-79 y where the percentage of individuals with no sign was the highest. These findings indicated that in our normal cohort, hCS are frequent in females independently of their age but they are rather related to aging in males. Gender as a primary cause of hCS was further confirmed by a higher percentage of males without signs in both Figures 2C and 2F).
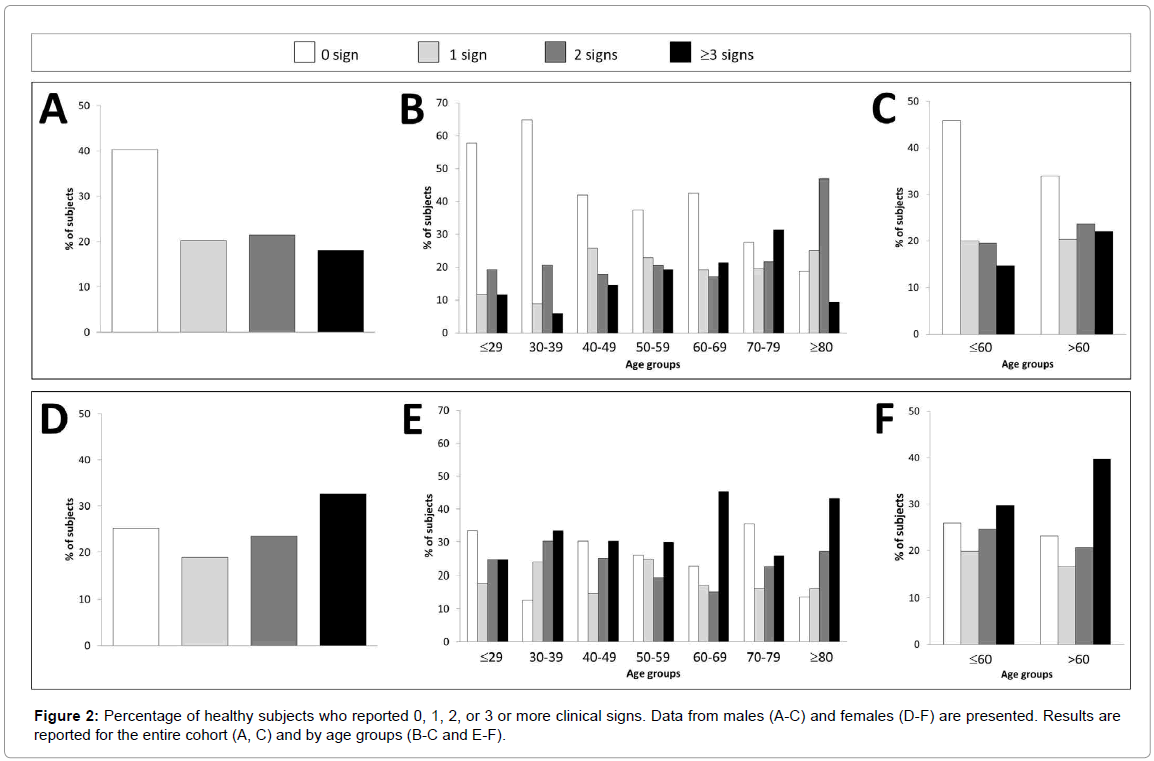
Figure 2: Percentage of healthy subjects who reported 0, 1, 2, or 3 or more clinical signs. Data from males (A-C) and females (D-F) are presented. Results are reported for the entire cohort (A, C) and by age groups (B-C and E-F).
Expression of individual hCS-We further analyzed individually 11 of the clinical signs commonly recognized for hypothyroidism [39]. The percentage of individuals with impairment of hearing was increased with aging for both genders (p<0.01). In contrast, hoarseness of voice, dry skin and slow movement were more specific for older males (p<0.05), and periorbital puffiness more specific for older females (p<0.05) (Figure 3A). We also observed that hoarseness of voice (p<0.05) and cold skin (p<0.01) were more represented in younger females while dry skin and constipation (p<0.01) was increased in females whatever the age group (Figure 3B). Overall, these findings indicated that hCS displayed a variable expression both in number and in nature as a function of gender and age. It was thus of primary importance to understand how they relate to representative biological features, namely TSH and thyroid hormones levels.
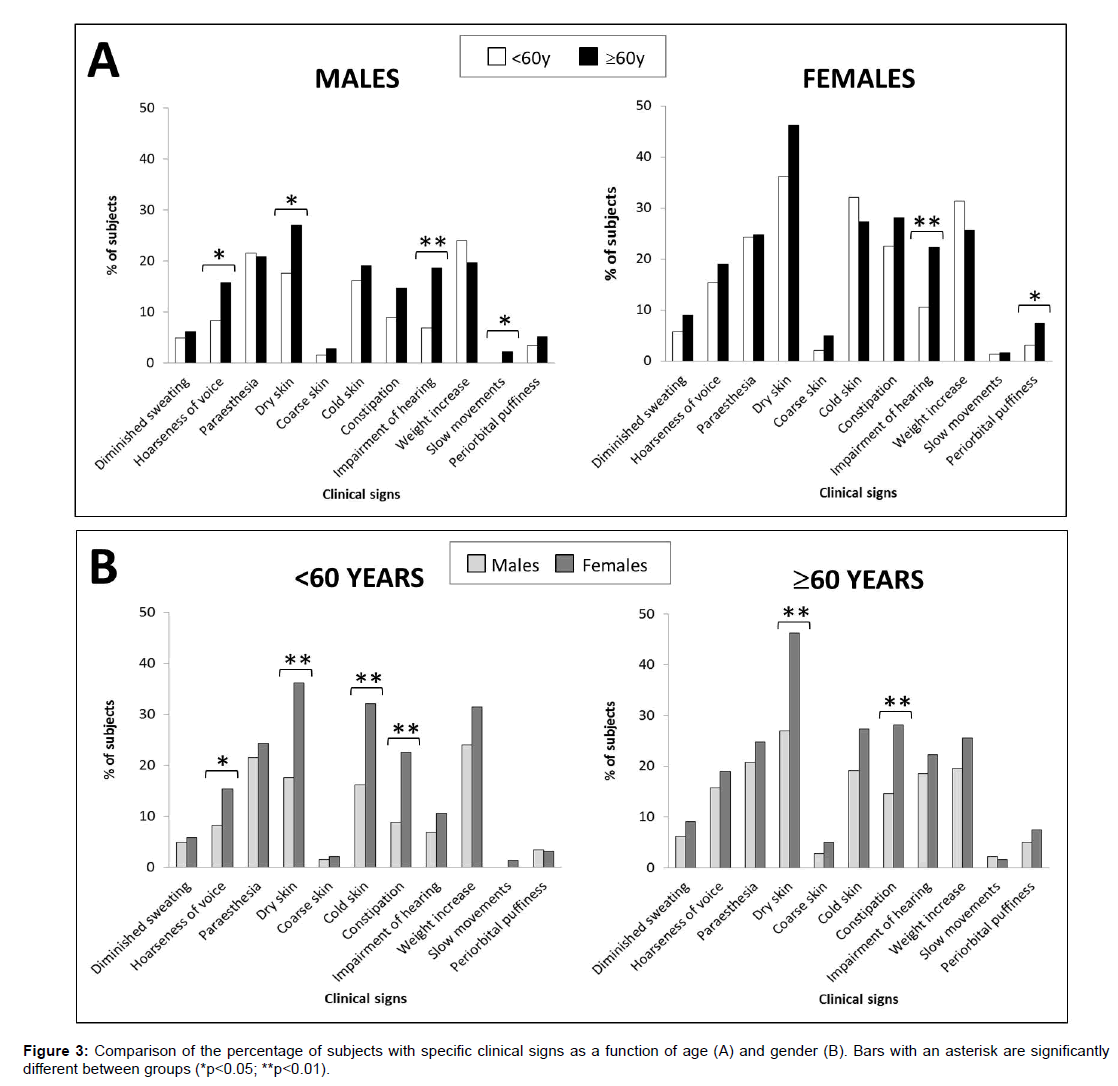
Figure 3: Comparison of the percentage of subjects with specific clinical signs as a function of age (A) and gender (B). Bars with an asterisk are significantly different between groups (*p<0.05; **p<0.01).
Biological parameters of the healthy cohort
Routine measurements for thyroid function testing i.e. TSH and thyroid hormones were analyzed as a function of gender and age (Figure 4). TSH levels in males decreased from ≤ 29 y to (40-49) y age group (p<0.05) and then increased until >80 y group (p<0.01). In contrast, TSH levels were rather constant in females, from (18-29) y to (40-49) y age group but dramatically increased until (70-79) y (p<0.01). The lowest levels were clearly found beyond 80 y (Figure 4A). FT4 levels were not different between both genders (p>0.05) and did not vary much with aging (p=0.34 and p=0.54 for males and females respectively) except for the population Figure 4B). In contrast, FT3 decreased with age for males and females (p<0.01) and a difference was observed between both genders for the groups ≤ 29y (p<0.05) and (40-49) y (p<0.01) as well as for the population Figure 4C). As a consequence, the FT3/FT4 ratio decreased with age for both males and females (p<0.05) (Figure 4D). Overall, the biological features agreed with hCS in that hormone levels also display high variability according to gender and age. Based on these considerations, we wanted to understand how diagnosis of hypothyroidism could be univocally defined in males as well as in females independently of their age.
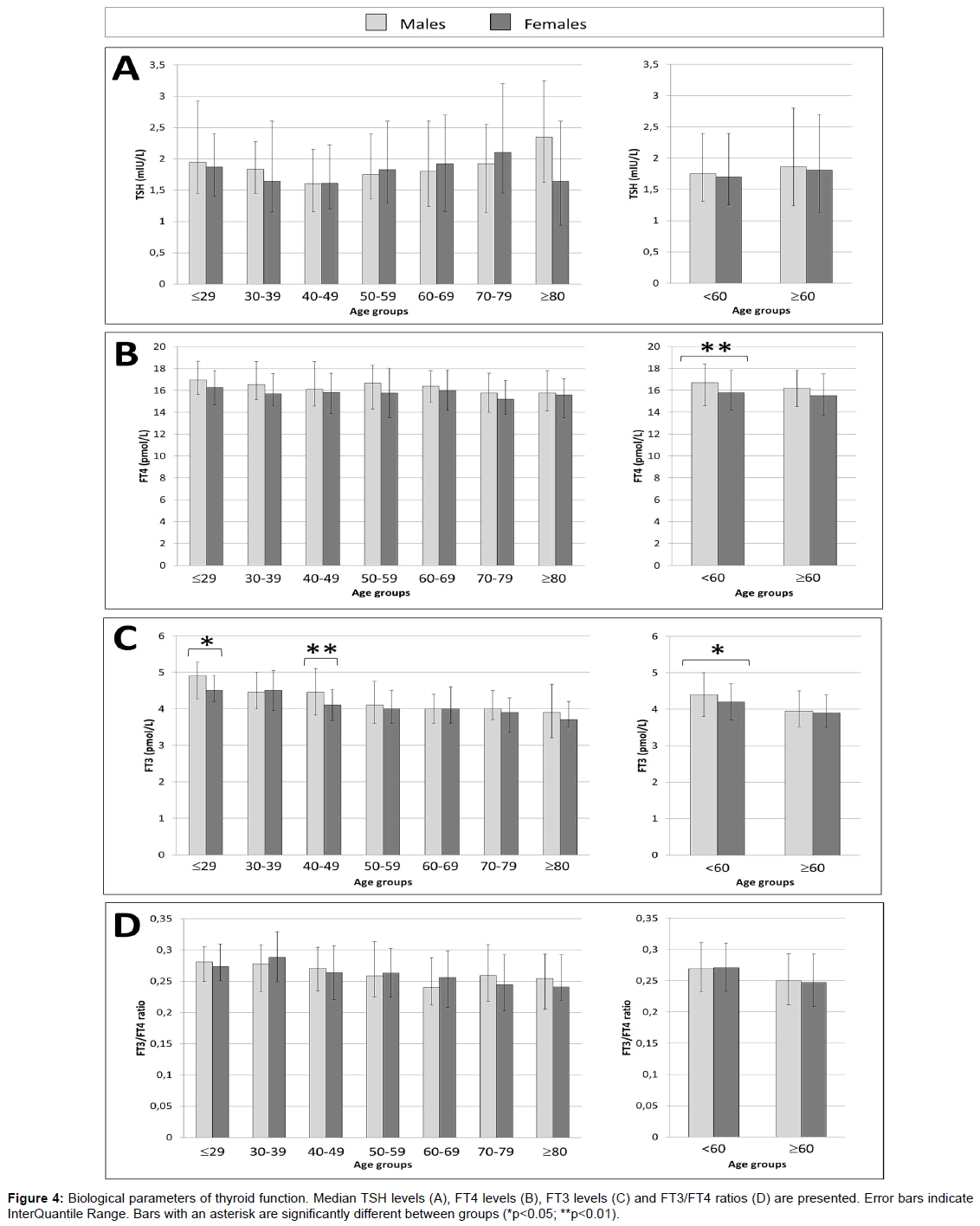
Figure 4: Biological parameters of thyroid function. Median TSH levels (A), FT4 levels (B), FT3 levels (C) and FT3/FT4 ratios (D) are presented. Error bars indicate InterQuantile Range. Bars with an asterisk are significantly different between groups (*p<0.05; **p<0.01).
Measuring bioactive TSH improves early detection of thyroid dysfunction
We recently published on several new assays measuring bioactive rgTSH and delivering harmonized values [28]. 4 out of 7 of them have been evaluated in this study. They were all compared to a commercial assay of IRMA generation used to harmonize all the samples collected from various hospitals. These assays were calibrated with rgTSH and designated as A to D: they all bind the same antigenic clusters in TSH although through distinct epitopes [28].To define the upper limit of the reference range for each of the 5 assays, we calculated the 97.5th centile based on NACB recommendations (Supplementary Table 1) [32]. We then analyzed the clinical and biological parameters of individuals diagnosed with elevated TSH for each assay, i.e. with TSH >97.5th centile. The number of subjects in each case was rather limited (≤ 20 individuals) as in IRMA, allowing us a comparative if not statistical analysis.
As shown in Table 1, the number of hCS remained unchanged below the 97.5th centile for all assays. However, there was a trend to display increased expression of hCS in individuals beyond the 97.5th centile when TSH was measured by the all 4 new assays (2.0 with new assays vs. 1.0 with routine assay). Results were similar when males (0- 1.0 with new assays vs. 0.5 with routine assay) and females (2.0-4.0 with new assays vs. 2.0 with routine assay) were analyzed independently. Clinical signs correlated with biological measurements (Table 2). The FT4 levels were found reduced or with decreased IQR in individuals with elevated TSH based on A-D assays. Males and females displayed similar effects.
| £ 97.5th centile | >97.5th centile | £ 97.5th centile | >97.5th centile | £ 97.5th centile | >97.5th centile | |
|---|---|---|---|---|---|---|
| ALL | MALES | FEMALES | ||||
| IRMA | 1.0 (0-3.0) (n=778) |
1.0 (0-2.5) (n=19) |
1.0 (0-2.0) (n=375) |
0.5 (0-1.3) (n=8) |
2.0 (0-3.0) (n=403) |
2.0 (1.0-4.5) (n=11) |
| Assay A | 1.0 (0-3.0) (n=777) |
2.0 (0-3.3) (n=20) |
1.0 (0-2.0) (n=372) |
1.0 (0-2.0) (n=11) |
2.0 (0-3.0) (n=405) |
2.0 (2.0-5.0) (n=9) |
| Assay B | 1.0 (0-3.0) (n=777) |
2.0 (0-4.0) (n=20) |
1.0 (0-2.0) (n=373) |
0 (0-1.8) (n=10) |
2.0 (0-3.0) (n=404) |
4.0 (2.0-4.8) (n=10) |
| Assay C | 1.0 (0-3.0) (n=777) |
2.0 (0-4.0) (n=20) |
1.0 (0-2.0) (n=373) |
0 (0-1.8) (n=10) |
2.0 (0-3.0) (n=404) |
4.0 (2.0-4.8) (n=10) |
| Assay D | 1.0 (0-3.0) (n=777) |
2.0 (0.8-4.0) (n=20) |
1.0 (0-2.0) (n=374) |
1.0 (0-2.0) (n=9) |
2.0 (0-3.0) (n=403) |
3.0 (2.0-4.5) (n=11) |
Table 1: Number of clinical signs. Results are given as median (IQR).
| £ 97.5th centile | >97.5th centile | £ 97.5th centile | >97.5th centile | £ 97.5th centile | >97.5th centile | |
|---|---|---|---|---|---|---|
| ALL | MALES | FEMALES | ||||
| IRMA | 16.1 (14.3-17.9) (n=778) |
14.8 (13.8-18.7) (n=19) |
16.4 (14.6-18.2) (n=375) |
15.7 (13.4-19.2) (n=8) |
15.8 (14.1-17.7) (n=403) |
14.7 (14.1-17.1) (n=11) |
| Assay A | 16.1 (14.3-17.9) (n=777) |
15.1 (14.2-16.1) (n=20) |
16.4 (14.6-18.2) (n=372) |
15.4 (14.5-17.7) (n=11) |
15.8 (14.1-17.8) (n=405) |
14.7 (14.2-14.8) (n=9) |
| Assay B | 16.1 (14.3-17.9) (n=777) |
14.8 (13.4-16.1) (n=20) |
16.4 (14.6-18.2) (n=373) |
15.7 (13.6-18.3) (n=10) |
15.9 (14.1-17.8) (n=404) |
14.7 (13.5-15.0) (n=10) |
| Assay C | 16.1 (14.3-17.9) (n=777) |
14.8 (13.7-16.1) (n=20) |
16.4 (14.6-18.2) (n=373) |
15.7 (13.6-18.3) (n=10) |
15.9 (14.1-17.8) (n=404) |
14.7 (14.1-15.0) (n=10) |
| Assay D | 16.1 (14.3-17.9) (n=777) |
14.8 (13.6-16.7) (n=20) |
16.4 (14.6-18.2) (n=374) |
15.4 (13.5-19.0) (n=9) |
15.8 (14.1-17.8) (n=403) |
14.7 (14.1-15.5) (n=11) |
Table 2: FT4 levels (pmol/L). Results are given as median (IQR).
We further identified which age group may better account for an elevation in TSH associated with a slight reduction in FT4 and increase expression of hCS. Table 3 shows that when TSH was measured with the new assays, females ≥ 60 y showed a median number of 2 clinical signs (1 sign with IRMA) combined to 14.0-14.6 median FT4 levels (14.7 with IRMA).When we compared the distribution of these older females with 0-2 vs. ≥ 3 clinical signs, it was clear that the new assays definitely better correlated with hCS than IRMA (Figure 5). We thus concluded that measuring an elevated level of bioactive TSH provides a better agreement between increased expression of clinical signs and decreased FT4 levels.
| £97.5th centile | >97.5th centile | £97.5th centile | >97.5th centile | ||||
|---|---|---|---|---|---|---|---|
| Clinical signs | FT4 (pmol/L) | ||||||
| ALL SUBJECTS | |||||||
| IRMA | 2.0 (0-3.0), n=286 | 1.0 (0-2.0), n=13 | 16.1 (14.3-17.8), n=286 | 14.7 (13.5-16.0), n=13 | |||
| Assay A | 2.0 (0-3.0), n=286 | 2.0 (0-2.0), n=13 | 16.1 (14.3-17.8), n=286 | 14.6 (13.7-15.9), n=13 | |||
| Assay B | 2.0 (0-3.0), n=287 | 2.0 (0-3.3), n=12 | 16.1 (14.4-17.8), n=287 | 14.0 (13.1-15.9), n=12 | |||
| Assay C | 2.0 (0-3.0), n=286 | 2.0 (0-3.0), n=13 | 16.1 (14.4-17.8), n=286 | 14.0 (13.2-15.9), n=13 | |||
| Assay D | 2.0 (0-3.0), n=287 | 2.0 (0.8-3.8), n=12 | 16.1 (14.4-17.8), n=287 | 14.1 (13.4-15.5), n=12 | |||
| MALES | |||||||
| IRMA | 1.0 (0-2.0), n=172 | 0.5 (0-1.0), n=6 | 16.3 (14.6-17.8), n=172 | 14.5 (13.1-15.9), n=6 | |||
| Assay A | 1.0 (0-2.0), n=171 | 1.0 (0-1.5), n=7 | 16.3 (14.6-17.8), n=171 | 15.4 (13.6-16.2), n=7 | |||
| Assay B | 1.0 (0-2.0), n=171 | 0 (0-1.5), n=7 | 16.3 (14.7-17.8), n=171 | 13.7 (13.2-16.2), n=7 | |||
| Assay C | 1.0 (0-2.0), n=171 | 0 (0-1.5), n=7 | 16.3 (14.7-17.8), n=171 | 13.7 (13.2-16.2), n=7 | |||
| Assay D | 1.0 (0-2.0), n=171 | 1.0 (0.5-2.5), n=7 | 16.3 (14.7-17.8), n=171 | 13.6 (13.2-15.9), n=7 | |||
| FEMALES | |||||||
| IRMA | 2.0 (1.0-3.0), n=114 | 2.0 (1.0-4.0), n=7 | 15.6 (13.7-17.5), n=114 | 14.7 (14.1-17.5), n=7 | |||
| Assay A | 2.0 (1.0-3.0), n=115 | 2.0 (2.0-5.0), n=6 | 15.8 (13.7-17.8), n=115 | 14.4 (14.1-14.7), n=6 | |||
| Assay B | 2.0 (1.0-3.0), n=116 | 4.0 (2.0-6.0), n=5 | 15.7 (13.9-17.7), n=116 | 14.2 (13.2-14.7), n=5 | |||
| Assay C | 2.0 (1.0-3.0), n=115 | 3.0 (2.0-5.5), n=6 | 15.8 (13.9-17.8), n=115 | 14.1 (13.4-14.6), n=6 | |||
| Assay D | 2.0 (0-3.0), n=116 | 2.0 (2.0-6.0), n=5 | 15.7 (13.7-17.7), n=116 | 14.2 (14.0-14.7), n=5 | |||
Table 3: Clinical and biological parameters of elderly females (≥60y) diagnosed with elevated TSH levels. Results are given as median (IQR).
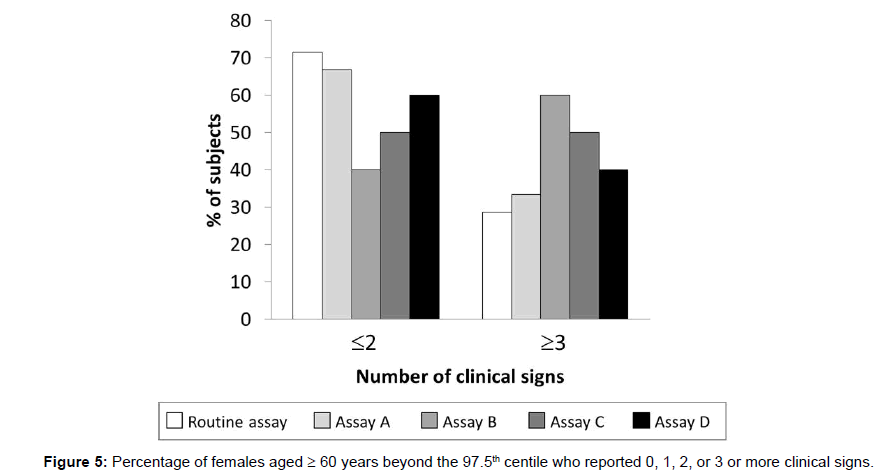
Figure 5: Percentage of females aged ≥ 60 years beyond the 97.5th centile who reported 0, 1, 2, or 3 or more clinical signs.
This study addressed the need for refined TSH assays to better monitor the thyroid status and allow early diagnosis of subclinical hypothyroidism. We have designed and validated new TSH assays which appeared to deliver harmonized values and better correlate to clinical signs of hypothyroidism.
Thyroid status of the healthy population
We selected herein a healthy cohort with no suspicion of thyroid deficiency as defined by the NACB. As anticipated, we could notice that expression of hCS differed as a function of gender and age. A higher percentage of females with at least 3 hCS was observed while a higher percentage of males did not show any sign. hCS appeared as soon as 30 y of age in females but only at 70 y of age in males. These clinical features were in agreement with a significant lower FT3 (p<0.05) and FT4 levels (p<0.01) found in <60 y females compared to <60 y males leading to hypometabolism together with hoarseness of voice, dry and cold skin, and constipation in young females. Interestingly, the TSH level was not particularly affected by reduced thyroid hormone levels. This may reflect a different regulation of the hypothalamo-pituitary-thyroid axis between both genders. TRH causes a dose-dependent increase in serum TSH concentration, which is almost 2-fold higher in women than men and related to decreased hypothalamic somatostatin secretion or diminished dopamine tonus [41]. Nocturnal surge amplitude is also found reduced in females [42] as frequently found in patients with Non-Thyroidal Illness Syndrome [43], a disease characterized by normal TSH levels and low thyroid hormones.
We also observed that expression of hCS increased with aging for both genders. These clinical signs are well recognized to be part of the aging process. Indeed, signs such as hoarseness of voice [44], dry skin [45], impairment of hearing [46] and periorbital puffiness [47] which were highlighted in the older participants have also been described in aging. Aging was also correlated with a TSH increase starting at 40 years of age (p<0.01) and decreasing FT3 levels (p<0.01) in both genders without modification of FT4 levels. This led to a decreased FT3/FT4 ratio with aging, suggestive of reduced bioactivity for TSH: increased TSH is needed to maintain the same level of T4 in the circulation. This finding is in agreement with the recent Busselton Health Study [48]. TSH levels in the elderly population may not always reflect an active TSH level and there is a clear need for revisiting the current threshold to allow a clear indication of thyroid deficiency.
Correlation of new TSH assays with clinic and biology
In earlier studies, we have investigated various calibrators of TSH assays [17] including the use of a recombinant glycoengineered calibrator to measure bioactive TSH [28]. To achieve similar immunological behavior between this preparation and serum TSH, we designed new sandwich assays based on defined selection of epitopes. Assays A-D have been selected to bind the Main Immunogenic Region [16] as in most marketed assays since it is a quite large area with at least 5 distinct epitopes. The new assays also bind a remote cluster which is not necessarily targeted in routine tests [28]. Such assays were found to display enhanced binding to serum TSH over the whole range of TSH level [28], indicating that they were able to bind all forms of TSH, more preferably sialylated TSH as it raises upon hypothyroidism [16,17,28]. Interestingly, these assays identified individuals with elevated TSH (>97.5th centile) who show an increased number of hCS and decreased FT4 levels compared to the routine assay. It is worth noting that assays A-D but not IRMA have been calibrated with a highly sialylated calibrator which mimics serum diseased TSH and thus provide a more accurate estimation than the pituitary 3rd IS 81/565 TSH used as primary calibrator. As a result, detection limits of TSH in the upper range appeared improved. Of special interest, these findings were gender-independent with improved detection for both males and females. In the older population, especially females, assays A-D detected an increased proportion of women with at least 3 hCS while the routine test indicated at most 2 signs. Such assays thus appeared more performant to diagnose a subclinical range of TSH in a healthy population, more particularly in elderly women.
Developing new assays will improve early diagnosis of thyroid dysfunction
Diagnostic of thyroid disorders are primarily based on the TSH reference range and defining a consensus upper limit has long been debated [35]. In light of the difficulties encountered by laboratories to define such a reference range for their local population, an indirect approach based on a posteriori study of the patient data already collected and stored in the laboratory database was suggested [38] possibly combined to statistical analysis [49]. In our opinion, such issue will remain unsolved as long as TSH assays show analytic bias [15]. Efforts are currently done by the IFCC Committee for Standardization of Thyroid Function Tests which recently proposed a mathematical recalibration to harmonize values among manufacturers [50,51]. However, this approach does not take into account the pathophysiological polymorphism of this hormone which may lead to underestimate TSH level in some assays. Refined TSH assays would be of primary interest for clinicians facing TSH values that poorly reflect TSH activity at the thyroid. TSH secreted by the pituitary adenomas was reported to change of glycosylation, leading to variable activation of the thyroid receptor [52,53]. During hypothyroidism, TSH is increasingly sialylated and current tests may miss some of these glycoforms and not provide optimal measurement of hormone level to treat the patients [16]. In the elderly population and more especially in women, measuring bioactive TSH could allow identifying patients developing SCH from those whose hypothalamic-pituitary axis compensates a decrease in TSH activity due to aging. These assays may be informative as well during pregnancy. Trimester-specific TSH reference ranges have been defined for pregnant women as a large decrease in TSH is observed during the first trimester followed by a steadily increase until delivery. However, TSH decrease during pregnancy was recently correlated with active TSH increase [54].
Nowadays people are daily exposed to many thyroid-disrupting chemicals [55]. Combined with the radioactive fallout of Nuclear Power Plant Accidents [56] and exposition to mobile phones [57], early detection of thyroid dysfunction may be of wide interest to monitor the overall population on a long-term range. Since regulatory bodies now request that TSH values should be harmonized and calibrated in mass units, our new assays nicely fit the new regulatory constraints and can serve such follow up because they can improve the detection limits.
New TSH assays proved to be efficient in discriminating subjects with subclinical range of TSH based on clinical (hCS expression) and biological (FT4 levels) parameters. They were particularly interesting for the elderly population in which bioactive TSH may decrease upon aging. This study could then demonstrate that better accuracy in TSH testing can be achieved by changing of calibrator and using epitopedefined antibodies. Such assays were able to overcome the technical limitations which have been accumulating over years and assay generations because of the use of a primary calibrator which did not adequately reflect the polymorphism of serum TSH and which lost activity over years of storage. These new assays may act in second line to prevent repeated monitoring and thus favor monitoring of thyroid dysfunction at the lowest cost and be a valuable help in preventive medicine.
We warmly thank Dr Karim Chick for constant interest and fruitful discussion, Dr Anne-Sophie Gauchez and Dr Anne Charrié for active participation in the clinical team. We are also very grateful to Dr Elisabetta Kuczewski for clinical assistance, the Departments of Endocrinology and Geriatrics of the Lyon Sud Hospital and the Departments of Endocrinology and Nuclear Medicine of the Chambery Hospital for motivation in recruiting subjects and valuable contribution in routine assay measurements. We are also grateful to Chloé Iss for technical contribution in the measurements of TSH.
The collection of blood samples was supported by the French National Research Agency (ANR) under the TSH TESTING program via the BIOTECS program ANR-10-BIOT-0013: the clinical work was entirely supported by public funds (salaries by hospitals and reagents by ANR) and Siamed’Xpress received funding for the assays and the production of glycoengineered TSH. The clinical validation described in this manuscript was entirely supported by Siamed’Xpress. The National Agency had no influence on the execution and writing of this article.
Siamed’Xpress is a startup company which holds two patents, one on methods for producing sialylated therapeutic proteins (PCT/EP2014/001904) of which CR is inventor, and one on the screening of glycoform-specific antibodies (PCT/EP2005/001160) of which SDA and CR are co-inventors. None of them relate to the clinical study described in the manuscript. The clinical validation presented in this study is not patented. Since Pr.C. Ronin is a founder and shareholder of Siamed’Xpress and S Donadio-Andréi a R&D manager at the company, potential conflict of interest is thus declared.