Endocrinology & Metabolic Syndrome
Open Access
ISSN: 2161-1017
ISSN: 2161-1017
Research Article - (2018) Volume 7, Issue 3
Background: Thyroid hormone is necessary for normal brain growth, myelination, normal neuronal connections and physical growth. The most critical period for the effect of thyroid hormone on brain development is the first few months of life. No data from Cameroon that described the iodine status and thyroid function of the Cameroonian pregnant women and neonates is available. This study determined the newborn Thyroid Stimulating Hormone levels at the Yaounde Gyneco-Obstetric and Paediatric Hospital-Cameroon and demonstrated the association between perinatal factors and newborn TSH levels.
Subjects and method: A descriptive cross-sectional study was done from the 10th January to 10th March 2017. On the third day of life, the heel prick blood obtained and dropped on a filter paper was analyzed for TSH using the commercial Human Neonatal TSH ELISA Kit (Catalog number EL10012N from Anogen, Yes Biotech Laboratories Ltd. Canada). The mean Thyroid Stimulating Hormone levels of the newborns were determined and, considering the perinatal factors and one-way analysis of variance were used to determine any correlation between the Thyroid Stimulating Hormone values and perinatal factors.
Results: 180 newborns were recruited during the study period. The Thyroid Stimulating Hormone values were normally distributed, within the range of [1.17-2.57 μIU/ml]. The mean Thyroid Stimulating Hormone value for the subjects was 1.59 ± 0.22 μIU/ml. 96.11% were within [-2SD and + 2SD]. Only high birth weights have been found to be associated with the high Thyroid Stimulating Hormone levels.
Conclusion: This study presented the normal reference values for Thyroid Stimulating Hormone in Cameroonian newborns at the Yaounde Gyneco-Obstetric and Pediatric Hospital Cameroon. Using this result, no neonates in the study had values pointing to a Congenital Hypothyroidism diagnosis.
Keywords: Congenital hypothyroidism; Thyroid stimulating hormone (TSH); Newborns; Yaounde Gyneco-Obstetric and Pediatric hospital (YGOPH); Cameroon
Congenital hypothyroidism is an abnormality of development and/or function of the thyroid gland, anomaly present at birth. The thyroid gland is normally located at the base of the neck. Congenital hypothyroidism is most often due to an abnormality of the thyroid gland (the thyroid is not capable of producing thyroid hormones in sufficient quantity), much more rarely to a secondary abnormality (the hormone TSH, insufficiently secreted by the pituitary gland, fails to stimulate the thyroid to make thyroid hormones). The main function of the thyroid gland is to synthesize T4 and T3. The only known physiologic role of iodine (or iodide [I−] in its ionized form) is in the synthesis of these hormones; the recommended dietary allowance of iodine is 30 μg/kg/24 hr for infants, 90-120 μg/24 hr for children, and 150 μg/24 hr for adolescents and adults. For pregnant and lactating women, the daily iodine needs are 250 μg/day [1].
The chemical form of iodine ingested, reaches the thyroid gland as iodide. Thyroid tissue has avidity for iodide and is able to trap, transport, and concentrate it in the follicular lumen for synthesis of thyroid hormone. The most critical period for the effect of thyroid hormone on brain development is the first few months of life. Thyroid hormone deficiencies contribute to severe retardation of growth and maturation of almost all organ systems. Most infants with congenital hypothyroidism (CH) are asymptomatic at birth. Clinical picture is fully developed by 3 to 6 months of age, at this time therapy cannot restore neurodevelopment to hundred percent normal. The prevalence of CH ranges from 1:3500 to 1:4000 in Europe and in USA but it is much lower in the African American population at 1 in 11,000 [2-4]. Children of mothers with mild to moderate iodine deficiency have been known to have sub-optimal cognitive and behavioral functioning [5,6] an endemic iodine deficient zone was described in a District of west Cameroon in 1991. Therefore, we cannot extrapolate those results to the entire population of Cameroon because that District is not representative of the entire country [7]. There is a need to study the iodine status of Cameroonian population especially of pregnant women and thyroid function of Cameroonian neonates. In a country with a low income and talking about newborn, screening program must be viewed as big challenge. In most centers where newborn screening is practiced, estimated blood spot T4 (thyroxine) or TSH (Thyroid Stimulating Hormone) or both can be used. Some authors have found that the use of estimated TSH for screening was shown to be more sensitive and more specific in the diagnosis of CH [8-10]. The age at which the blood spot sample is taken may vary between centers, with the majority taking blood from a heel prick after 48 hours of age. This will minimize the false positive high TSH due to the physiological neonatal TSH surge and dynamic T4 and T3 changes in the first or second days after birth [10].
However, in Cameroon, as in many developing economies, babies are discharged home with their mothers on the third day (72 h) after delivery; for this reason a newborn-specific reference range must be developed for the country concerned. We screened healthy newborn babies born in Yaounde Gyneco-Obstetric and Paediatric Hospital- Cameroon and tried to establish TSH reference range.
A descriptive cross-sectional study was done at the YGOPH Cameroon from the 10th January to 10th March 2017. Populated by 23.3 million people, Cameroon is a low-middle income country. Located in Central Africa, it borders with Gabon, Equatorial Guinea, Nigeria, Central African Republic (CAR) and Tchad. It has a surface area of 475442 km2. Ethical approval was obtained from the ethics and research committee of the Gyneco-obstetric and Paediatric Hospital of Yaounde, Cameroon. First day post-delivery, the mothers or legal guardian were informed about the study stating its objectives, benefits and risks involved, to obtain their consent. Having received the mother’s informed consents they were examined for goiter following which a physical examination was carried out on each neonate enrolled before the sample collection on the third day of life. Other information such as name, gestational age, mode of delivery, Apgar score, weight, head circumference and length of baby, social status of mother, were collected on the data sheet prepared for the study and blood sample was taken from babies who were admitted in the postnatal ward of the maternity unit and who fulfilled the inclusion criteria: Apparently healthy neonates in their third day of life for whom the mothers gave their consent.
The sample collection and storage
Blood collected from a heel prick on day three and placed on concentric circle on a filter paper. The commercial Human Neonatal TSH ELISA Kit, catalog number EL10012N was obtained from Anogen Yes Biotech Laboratories Ltd. 2355 Derry Road East, Unit 23 Mississauga, Ontario Canada L5S 1V6.
Each filter paper was named with a code number corresponding to the baby’s name and mother’s phone number on the collection form. The filter papers were allowed to dry at room temperature for at least four hours before being kept in an envelope ready for transportation to the collaborating laboratory-stored in the refrigerator while awaiting the laboratory analysis.
Data and statistical analyses
The samples were analysed for Thyroid Stimulating Hormone using the commercial Human Neonatal TSH ELISA Kit. The TSH cut-off for this Kit was 10 μIU/ml, the lowest reportable TSH value is approximately 0.03 μIU/ml with 95% confidence and the highest is 150 μIU/ml. Measures of statistical location like mean, frequencies, and standard deviations were generated using the Statistical Package for Social Sciences (SPSS) version 20 and R software’s. A one-way analysis of variance test (ANOVA) was used to compare the means of the TSH levels according to maternal (age, parity and occupation), newborn (Apgar score, gestational age, gender, birthweight, length, head circumference) characteristics and mode of delivery. Probability (p) value less than or equal to 0.05 was interpreted as statistically significant. Normality of TSH distribution was assessed using the Kolmogorov-Smirnov test.
In Table 1 the mean age group of the mothers was 20-30 years and a range of 17 to 50years. Concerning the parity, multiparity (>2) was most represented (60%). About 30% were self-employed followed by government employees (27%). 18% of babies were delivered by caesarean section of which emergency caesarean section constituted the majority of cases (70%) mainly due to fatal distress.82% of newborns were delivered by vaginal route.
| Mother’s age groups (n=180) | Frequency (n) | Percentage (%) |
| 20-30 years >30 years |
11 103 66 |
6 57 37 |
| Mother’s occupation (n=180) | ||
| State employee Student Housewife Independent |
48 34 44 54 |
27 19 24 30 |
| Parity (n=180) | ||
| Primiparous Multiparous High multiparous |
40 108 32 |
22 60 18 |
| Mode of delivery (n=180) | ||
| Vaginal route Caesarean section |
147 33 |
82 18 |
| Caesarean section (n=33) | ||
| Emergency caesarean section Elective caesarean section |
23 10 |
70 30 |
Results: One hundred and eighty (180) babies were recruited during the study period (2 months)
Table 1: The demographic characteristics of the study population.
The female to male ratio of the study population (Table 2) was of 1:1. Term babies were 161 (89%). The mean birth weight was 3205 ± 513 g with a range of 1900 g to 4600 g. The mean birth length was 50 ± 2 cm and mean head circumference was 35 ± 2 cm. The mean gestational age was 39 weeks 2 days ± 1 week 5 days. Eighty four percent (84%) of babies had birth weight between 25003990 g. Babies having an Apgar score of ≥ 9/10 at the first minute of life represented 67%.
| Gender (n=180) | Frequency(n) | Percentage (%) | ||||
|---|---|---|---|---|---|---|
| Female Male |
90 90 |
50 50 |
||||
| Gestational age (n=180) | ||||||
| Preterm (<37w) Term (37-41w) Posterm (≥ 42w) |
12 161 7 |
7 89 4 |
||||
| Weight category (n=180) | ||||||
| Low birthweight(<2500g) Normal birthweight(2500-3999 g) Large birthweight(≥ 4000 g) |
18 151 11 |
10 84 6 |
||||
| Apgar score at the 1st min of life (n=180) | ||||||
| 7/10 8/10 ≥ 9/10 |
20 40 120 |
11 22 67 |
||||
| Mean | Standard Deviation | Minimum | Maximum | |||
| Birth weight (g) | 3205 | 513 | 1900 | 4600 | ||
| Head circumference (cm) | 35 | 2 | 30 | 39 | ||
| Birth length (cm) | 50 | 2 | 43 | 54 | ||
| Gestational age at birth W=week, d=day |
39w2d | 1w5d | 33w0d | 44w2d | ||
Table 2: Characteristics of newborn babies.
The figure 1 above shows the distribution of TSH values. We obtained a symmetrical, bell shaped curve meaning that our results follow the normal law of the Kolmogorov-Smirnov statistic. We found that 77.78% of newborns had TSH values between -1 and + 1 SD (1.371.81 μIU/ml), 96.11% between - 2 and + 2SD (1.15-2.03 μIU/ml). The boxplot in figure 2 is showing that there is not a big variation in TSH value and the outliers are not so many.
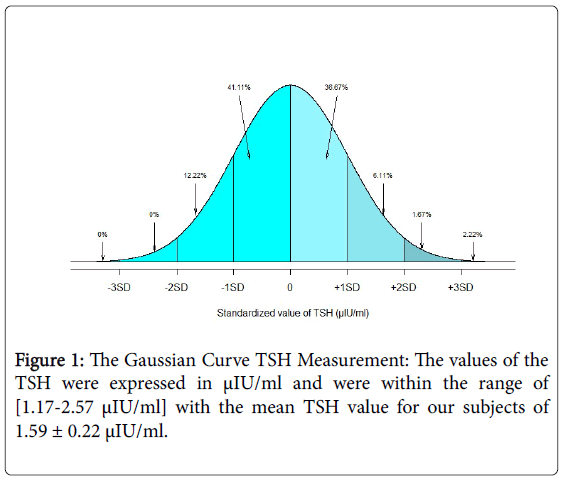
Figure 1: The Gaussian Curve TSH Measurement: The values of the TSH were expressed in μIU/ml and were within the range of [1.17-2.57 μIU/ml] with the mean TSH value for our subjects of 1.59 ± 0.22 μIU/ml.
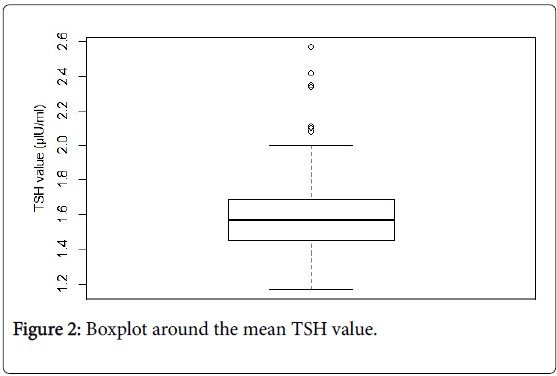
Figure 2: Boxplot around the mean TSH value.
In Table 3 Babies born from mothers who are students high multiparous and aged less than 20 years have had a high mean TSH value compare to the others but the difference was not statistically significant (p>0.05).
| TSH Value (µIU/ml) | ||||
|---|---|---|---|---|
| (95%CI) | ||||
| Mean | SD | Minimum | Maximum | |
| Mother’s occupation (p-value=0.551) |
||||
| State employee | 1.59 | 0.21 | 1.25 | 2.42 |
| Student | 1.63 | 0.28 | 1.17 | 2.57 |
| Housewife | 1.60 | 0.22 | 1.25 | 2.34 |
| Independent | 1.56 | 0.19 | 1.21 | 1.99 |
| Parity (p-value=0.0798) | ||||
| Primiparous | 1.63 | 0.26 | 1.17 | 2.57 |
| Multiparous | 1.56 | 0.20 | 1.21 | 2.42 |
| High multiparous | 1.64 | 0.22 | 1.21 | 2.10 |
| Age of the mother (p-value=0.326) | ||||
| 1.640.301.312.35 | ||||
| 20 -30 Y | 1.60 | 0.22 | 1.17 | 2.57 |
| >30 Y | 1.58 | 0.22 | 1.21 | 2.10 |
Table 3: Relationship between the TSH value and maternal factors.
Babies delivered by caesarean section and from whom the caesarean section was planned (elective) table 4 had a mean TSH value higher than those delivered vaginally but the difference was not statistically significant (p>0.05).
| TSH Value (µIU/ml) | ||||
|---|---|---|---|---|
| (95%CI) | ||||
| Mean | SD | Maximum | Minimum | |
| Mode of delivery (p-value=0.086) | ||||
| Vaginal | 1.58 | 0.20 | 1.17 | 2.42 |
| Caesarean section | 1.65 | 0.30 | 1.21 | 2.57 |
| Reason for emergency cesarean section (p-value=0.55) | ||||
| Emergence caesarean section | 1.64 | 0.33 | 1.21 | 2.57 |
| Elective caesarean section | 1.67 | 0.22 | 1.44 | 2.10 |
Table 4: Relationship between the TSH value and mode of delivery.
There was no difference between the mean TSH value of girls and boys as shown in Table 5 (1.59 μIU/ml respectively); babies delivered with an Apgar score of 7/10 and ≥ 9/10 at the 1st minute, term babies have had a higher mean TSH value compare to others babies but the difference was not statistically significant. However macrosomic babies (birth weight ≥ 4000 g) had a higher mean TSH value compare to low birthweight and normal birthweight babies and the difference was statistically significant with a pFigure 3.
| TSH Value (µIU/ml) | ||||
|---|---|---|---|---|
| (95%CI) | ||||
| Mean | SD | Minimum | Maximum | |
| Gender (p-value=0.674) | ||||
| Female | 1.59 | 0.23 | 1.21 | 2.42 |
| Male | 1.59 | 0.22 | 1.17 | 2.57 |
| Apgar Score (p-value=0.436) | ||||
| 7/10 | 1.60 | 0.16 | 1.37 | 2.10 |
| 8/10 | 1.55 | 0.20 | 1.25 | 2.34 |
| ≥ 9/10 | 1.60 | 0.24 | 1.17 | 2.57 |
| Gestational age (p-value=0.631) | ||||
| Preterm | 1.53 | 0.21 | 1.32 | 2.10 |
| Term | 1.60 | 0.22 | 1.17 | 2.57 |
| Post-term | 1.54 | 0.19 | 1.23 | 1.71 |
| Birthweight (p-value=0.0261) | ||||
| Low birthweight | 1.59 | 0.22 | 1.32 | 2.10 |
| Normal birthweight | 1.58 | 0.21 | 1.17 | 2.57 |
| Macrosomia | 1.77 | 0.26 | 1.31 | 2.35 |
Table 5: Relationship between the TSH value and newborn factors.
Preliminary analyses were performed to ensure no violation of the assumptions of normality, linearity and homoscedasticity. In Table 6 we founded that there was a weak correlation between the birthweight and the mean TSH value only (r=0.138, n=180, p<0.05) and a shared variance of 1.9%.
| Birth weight | Head circumference | length | ||
|---|---|---|---|---|
| n=180 | ||||
| TSH value | r=0.138 p.value=0.0261 |
r=0.0165 p-value=0.8259 |
r=0.0214 p-value=0.7755 |
Table 6: Correlation analysis between the TSH value and newborn anthropometric characteristics.
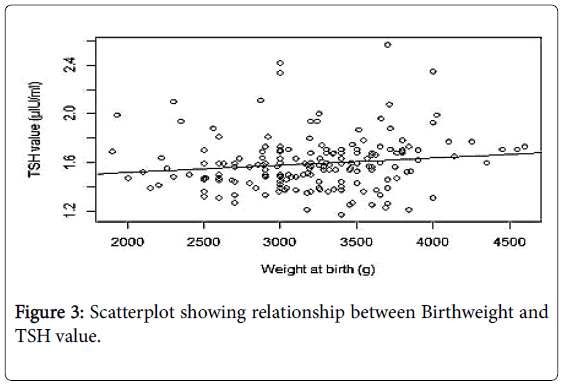
Figure 3: Scatterplot showing relationship between Birthweight and TSH value.
The final sample size for the evaluation of TSH was 180. The TSH’s curve follows the curve of the normal law. 96.11% were within -2SD and +2SD. These findings are contrary to those found by Iroro [11] in Nigeria where their TSH was not normally distributed, because of the big sample size (n=1767) and the heel prick blood obtained at different age (from the 1st to the 5th day of life). The TSH value of our study population was within the range of [1.17-2.57 μIU/ml] with the mean TSH value for our subjects of 1.59 ± 0.22 μIU/ml; This value is lower than the one found in Lithuania in 2010(3.12 ± 1.04 μIU/ml) [12], and in Benin [13] (10.25 μIU/ml) or Sokoto [14] (2.52 μIU/ml) in Nigeria. This can be explained by the fact that Lithuania, Sokoto and Benin are considered regions of mild iodine deficiency. Our mean TSH values were however low compared to the one from Germany (3.11 μIU/ml) in 2011 [15] and Netherlands in 2012 [16] (3.75 μIU/ml). Some factors such as different ethnic group, different nutrients in diet could explain the observed difference.
None of the neonates had values associated with Congenital Hypothyroidism diagnosis (Thyroid Stimulating Hormone level >40 μIU/ml). However, given our small sample size, it was difficult to conclude that there were no cases of congenital hypothyroidism in our population or that our population was not iodine deficient. This highlights the need for a further study using a larger sample size.
Performance of a one-way ANOVA analysis to adjust for maternal age, maternal occupation, parity and TSH was opposite to that found in Lithuania where maternal age was related to neonatal TSH levels in newborns (older maternal age in pregnancy was associated with elevated newborn bloodspot TSH levels) [12]. According to the worldwide database, it is well known that older pregnant women carry a higher risk of having a baby with an abnormality. These findings strongly suggest a very early impairment in the first stages of embryo development with a consequent involvement of different organs and structures [17-19]. The difference may be explained by the small representation of mother aged >30 years (37% only, the majority of mothers in our study were relatively young) in our study. Although we did not confirm this and therefore it is a confounder, the possibility that our mothers were not iodine deficient may be a factor. The national policy on fortification of salt with iodine may also be responsible for this observation. Utilization of iodized salt for the prevention of goiter was officially launched by the Ministry of Public Health of Cameroon in June 1991. This may not be an issue because fortification of salt with iodine is global.
Our results showed that babies born by caesarean section had a higher mean TSH value compared to those born vaginally though there were no association between the mean TSH level and the mode of delivery with a P>0.05. The expectation was to have an increase of the TSH level in babies born by vaginal route. It is another source of stress as it has been documented that in situation of stress we have an increase of the TSH value. Various researches on the effect of mode of delivery on thyroid function have documented conflicting reports. Babies delivered by caesarean section are significantly more likely to have TSH levels greater on day 3 than those delivered vaginally. A marked elevation in neonatal TSH has been documented with topical iodine antiseptic use on the neonate in some reports [20-22]. As we do not use iodine antiseptic for umbilical cord care, may be iodine preparation have crossed the placenta via he mother’s skin during the pre-operatory care for caesarean section (time of cleansing and extraction long enough to allow this to happen).
No sex-differences were found for mean TSH levels in our study. This result was different from the one found by Korada et al in United Kingdom where male gender have had a higher median TSH value [23]. This difference can be explained by the high proportion of male gender in their study compared to ours.
There were no effects of gender, Apgar score at birth and gestational age on TSH levels. Our results do not correlate with those found by Ingrida [12] and Mc Elduff et al. [20] where gestational age was related to neonatal TSH levels in newborns without CH. They found that longer gestation at birth was associated with elevated newborn bloodspot TSH levels. It is known however, that as gestational age increases, the fetus increases the synthesis of both T4 and TSH [24]. This difference may be explained by the small representation of postterm babies (7%) in our study.
Regarding our results, a relationship between birth weight and mean TSH level was established at the p<0.05, macrosomic babies had a higher mean TSH level compared to the other babies. Higher birth weights were associated with high TSH values however, only about 2% of the variability in TSH values can be explained by changes in birth weight alone. This weak correlation and low-shared variance can be explained by the small size of our sample. This result is opposed to Korada et al. findings where higher TSH were found in the lowest birth weight categories [23] This difference can be explained by the fact that all gestational age where included in the study also inclusive of preterm. It is well known that premature babies are high risk of morbidity and mortality, and illness is another shape of stress [25]. In Turkey, no correlation was found between the TSH level and gender, birth weight and mode of delivery [26]. Iroro in Nigeria in later years did not find any association between the TSH values and perinatal factors.
Normal reference values of TSH was obtained in the neonate studied (<40 μIU/ml). Birth weights were observed to influence the newborns TSH levels. High birthweight was associated with elevated TSH values. None of the infant had values associated with CH diagnosis. This cannot be a categorical statement by our study or that our study population was not iodine deficient. There is a need for further studies using larger sample size taking from other part of the country.
A limitation observed for his study is recruitment of the potential mother at delivery and not during their antenatal visit .If this was done more mothers would have participated in the study.
The Director of the Paediatric Endocrinology Training Center for West Africa; the Yaounde Gyneco-Obstetric and Paediatric Hospital- Cameroon, the members of the staff who assisted in sample collection. A great respect to Pr. Tetanye Ekoe, Pr. Chiabi Andréas, Dr Mah Evelyn, Dr. Ngo Um Sap Suzanne, Dr Njiki Mina , Dr Iroro Yarhere, Dr for their assistance to this study.