Journal of Depression and Anxiety
Open Access
ISSN: 2167-1044
ISSN: 2167-1044
Research Article - (2014) Volume 3, Issue 3
We investigated the plasma levels of 3-methoxy-4-hydroxyglycol (MHPG) in patients who failed to paroxetine treatment and switched to milnacipran. The aim of the present study is to predict responders to serotonin noradrenaline reuptake inhibitor (SNR) who were resistant to selective serotonin reuptake inhibitor (SSRI) based on the plasma MHPG levels. The HAMD17 scores decreased from 17.0 ± 2.2 to 9.5 ± 2.5 after 4 weeks of milnacipran treatment. Eight of 20 (40%) patients were responded 4 weeks after milnacipran treatment. Five of 20 (25%) became remission. Plasma MHPG was changed neither in responders (from 4.9 ± 0.7 ng/ml to 5.6 ± 0.8 ng/ml) (t=-1.604, p=0.132) nor in nonresponders (from 5.1 ± 1.3 ng/ml to 5.3 ± 1.2 ng/ml) (t=-0.363, p=0.719). No difference was found in the change of plasma MHPG before and 4 weeks after milnacipran administration in two groups (t=1.894, p=0.073). These results suggest that the change of plasma MHPG level was not related to the improvement when switching from paroxetine to milnacipran.
Keywords: Milnacipran; Paroxetine; 3-methoxy-4-hydroxyphenylglycol; Major depressive disorder
Monoamines play still an important role for pathophysiology of mood disorders. 3-methoxy-4-hydroxyphenylglycol (MHPG), a major metabolite of noradrenaline, partially reflects brain noradrenaline activity. About 10-30% of plasma MHPG derived from brain [1]. We previously reported that patients with lower plasma MHPG had a better response to milnacipran, a serotonin-noradrenaline reuptake inhibitor (SNRI), and those with higher plasma MHPG had a better response to paroxetine, a selective serotonin reuptake inhibitor (SSRI). In addition, patients who responded to milnacipran increased plasma MHPG and those who responded to paroxetine decreased plasma MHPG [2]. However, few studies were found demonstrating the changing dynamics of plasma MHPG when switching SSRI to SNRI. Therefore, we investigated the plasma MHPG levels in patients who failed to paroxetine treatment and switched to milnacipran. The aim of the present study is to predict responders to SNRI who were resistant to SSRI based on the plasma MHPG levels.
Twenty patients who met major depressive disorder using DSM-IV-TR and failed to paroxetine treatment at least 4 weeks enrolled in the study. Nine were male and 11 were female. Age ranged from 22 to 74 (mean ± standard deviation: 46 ± 13) yrs. The average maximum dose of paroxetine was 98 ± 36 mg/day. The method for switching paroxetine to milnacipran was used cross titration. The severity of depression was evaluated using the 17-item Hamilton Rating Scale for Depression (HAMD17). Only those patients with a HAMD17 score = 14 were eligible for the study. Exclusion criteria were any history of neurological disease or other physical disease, and comorbidities with other mental disorders (no evidence of schizoaffective disorder, bipolar disorder or Axis II, personality disorders or mental retardation). All subjects were given complete information about the procedures. Written informed consent was obtained from all subjects via forms approved by the local Ethics Committee of the University of Occupational and Environmental Health. The present study was one-armed naturalistic and observation study.
Blood sampling was performed before and 4 weeks after staring milnacipran. The subjects’ plasma MHPG levels were also analyzed by HPLC-ECD, according to the method of Minegishi and Ishizaki [3]. In brief, the plasma was separated by centrifugation at 600×g at 4°C. Extraction was performed under a vacuum using Bond-Elut columns (Varian, Palo Alto, CA) prepacked with 100 mg of C18-bonded silica (40 µm) in a 1-mL capacity disposable syringe. The columns, which were inserted into a vacuum chamber connected to an aspirator, were prepared by washing with 1 mL methanol followed by 1 mL of water. After the addition of 50 µL of a solution of vanillyl alcohol (ref. 43; internal standard equivalent to 5 ng/mL) to 1 mL of plasma, the samples were passed through the columns, followed by 0.75 mL of water to rinse off both residual samples and easily eluted hydrophilic compounds.
The adsorbed materials were eluted with 200 µL of methanol to a 0.1 M phosphate buffer (pH 4.8) mixture (40:60, v/v). A 20-µL portion of this solution was injected into the HPLC system. The detection limit was 0.5 ng/mL, and the calibration curve was linear up to 40 ng/mL. The intra- and inter-assay coefficients of variation were 6% and 8%, respectively. The recovery rate was more than 80%.
Student’s t-test was used to compare two groups and correlations with clinical variables were performed using Peasons’ correlation. A significant value of p<0.05 was judged as statistically significant. All analyses were carried out using SPSS version 19.0 (SPSS Inc, Chicago, IL, USA).
The HAMD17 scores decreased from 17.0 ± 2.2 to 9.5 ± 2.5 after 4 weeks of milnacipran treatment. Eight of 20 (40%) patients were responded 4 weeks after milnacipran treatment. Five of 20 (25%) became remission. Plasma MHPG levels in all patients did not change before (5.0 ± 1.4 ng/ml) and 4 weeks after milnacipran treatment (5.4 ± 1.3 ng/ml) (t=-0.999, p=0.323, Cohen’s d=0.326). No difference was found in baseline plasma MHPG between responders (4.9 ± 0.7 ng/ml) and nonresponders (5.1 ± 1.3 ng/ml) to milnacipran treatment (t=-0.704, p=0.488, Cohen’s d=0.861). Plasma MHPG was changed neither in responders (from 4.9 ± 0.7 ng/ml to 5.6 ± 0.8 ng/ml) (t=-1.604, p=0.132, Cohen’s d=0.040) nor in nonresponders (from 5.1 ± 1.3 ng/ml to 5.3 ± 1.2 ng/ml) (t=-0.363, p=0.719) (Figure 1). In addition, no difference was found in the change of plasma MHPG before and 4 weeks after milnacipran administration in two groups (t=1.894, p=0.073). No correlation between the changes in plasma MHPG and the changes in subscale in HAMD17 (activity) (r=0.188, p=0.413) (Figure 2).
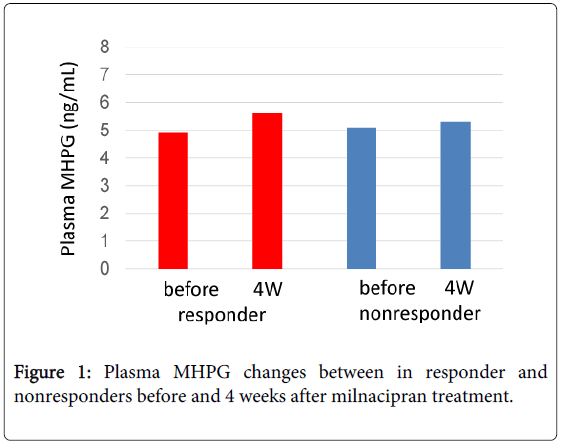
Figure 1: Plasma MHPG changes between in responder and nonresponders before and 4 weeks after milnacipran treatment.
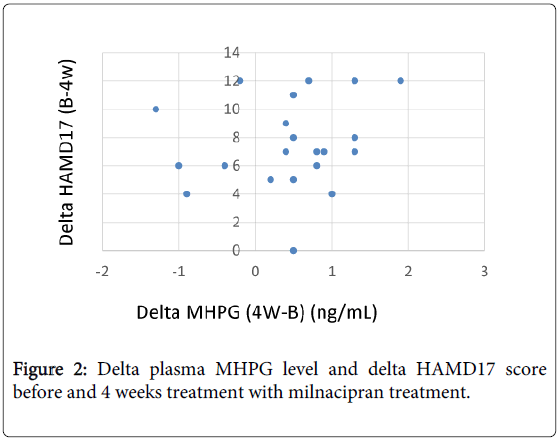
Figure 2: Delta plasma MHPG level and delta HAMD17 score before and 4 weeks treatment with milnacipran treatment.
The plasma MHPG level was not altered from changing from paroxetine treatment to milnacipran treatment in the all patients. The baseline plasma MHPG level with the non-responders to paroxetine treatment was not different between responders and non-responders to milnacipran treatment. The result suggests that the baseline plasma MHPG level did not predict the response to milnacipran after switching from paroxetine. No difference was found in the change of plasma MHPG before and 4 weeks after milnacipran administration in two groups. Taken together, it is not possible that the change of plasma MHPG level was not related to the clinical improvement when switching from paroxetine to milnacipran.
We previously reported that plasma MHPG level in patients who had better response to milnacipran was lower than in those who did not respond to milnacipran [2]. The result in the present study was not in accordance with our previous study [2]. However, patients in the present study were treated with paroxetine at least 4 weeks, which had influenced the plasma MHPG level. Eight of 20 patients who failed to paroxetine treatment responded to treatment with milnacipran, plasma MHPG level in responders was however not increased 4 weeks after milnacipran treatment. Also baseline plasma MHPG could not be a biological marker in prediction for improvement after switching from paroxetine to milnacipran. It is possible that effect of paroxetine treatment before switching to milnacipran influence the results. Several factors influencing response to milnacipran have been recently studied. Yoshida et al. [4] reported that noradrenaline transporter polymorphism, but not that of serotonin transporter is associated with rapid response to milnacipran. We previously reported that patients with low pretreatment levels of plasma MHPG have a better response to milnacipran [2]. These genomic and neurochemical data indicate that milnacipran has an impact on the noradrenergic system. We recently reported that duloxetine also increased plasma MHPG level in patients with major depressive disorder [5]. The present study had several limitations. First, we used cross titration when changing from paroxetine to milnacipran, and did not set the washout periods. Second, this study was open design and without control group. The sample size was very small and heterogeneous. The study design was one-armed naturalistic and observation. Therefore results from present preliminary study might not be robust. Thus, further study should be performed to reconfirm the results. In conclusion, the change of plasma MHPG level was not related to the improvement when switching from paroxetine to milnacipran.