Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Research Article - (2018) Volume 7, Issue 2
Background: Two point CUS (2-CUS) for the diagnosis of symptomatic proximal DVT overlooks calf vein thrombosis (CVT) indicating the need to repeat 2-CUS after one week, which is not cost-effective. Complete CUS (CCUS) of all deep veins from the groin to the ankle in a single procedure will pick up CVT, proximal DVT and isolated ileo femoral DVT plus alternative diagnoses, which is cost-effective.
Methodology: We evaluated the combined use of non-invasise 2-CUS versus complete compression ultrasonography (CCUS) and quantitative Elisa D-dimer levels (500, 1000 and 1500 ng/mL) in prospective large management studies between 1998 and 2018 in view of the literature on DVT diagnosis and prevention of DVT recurrence and the post-thrombotic syndrome.
Results: Complete compression ultrasonography (CCUS) followed by a sensitive D-dimer test and clinical score assessment is a safe and cost-effective non-invasive strategy to exclude and diagnose deep vein thrombosis (DVT) and alternative diagnoses (AD) in patients with suspected DVT. Rapid and complete recanalization on serial CUS within 3 months post-DVT with no residual venous pathology (RVP-) is associated with low risk of DVT recurrence (1.2% patient/years) and PTS on the basis of which both anticoagulation MECS can be withdraw at 4 months postDVT. Delayed and incomplete recanalization with RVP+ on CUS at 3 months post-DVT is associated with the presence of reflux due to valve destruction, a high risk of DVT recurrence. Symptomatic PTS at 6 to 12 months postDVT have a clear indication to wear MECS for symptomatic relief of PTS symptoms and to extend anticoagulation for one to several years to prevent DVT recurrence. Wearing MECS does not prevent DVT recurrence, reflux and outlet obstruction in symptomatic PTS patients in the original Prandoni and the two large COX and IDEAL prospective randomized clinical studies. The Lower Extremity Thrombosis (LET) extension classification identifies patients with CVT LET class I, proximal DVT LET class II and iliofemoral DVT LET class III at time of acute DVT diagnosis. The higher the LET class the higher the risk of DVT recurrence and PTS.
Conclusion: The Villalta score for PTS is not sensitive and specific enough to stratefy for DVT recurrence risk for the indication of extended anticoagulation in post-DVT patients after discontinuation of anticoagulation. Wearing MECS relieves subjective signs of PTS, does not reduce DVT and PE recurrence rate and has no influence on the natural history of PTS. The two randomized clinical trials CaVent and ATTRACT comparing catheter directed thrombolysis followed by anticoagulation versus anticoagulation alone were neither inferior nor superior to anticoagulation for the treatment of acute proximal popliteal-femoral and iliofemoral DVT.
Keywords: Deep vein thrombosis; Lower extremity thrombosis extension; DVT recurrence; Post-thrombotic syndrome; D-dimer; Clinical score; Medical elastic stockings
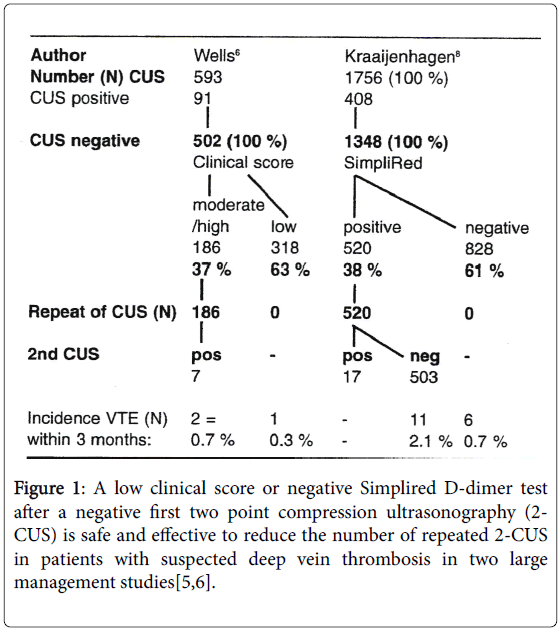
The annual incidence of a first episode of proximal deep vein thrombosis (DVT) is about 2 to 4 per 1000 inhabitants per year [1]. Clinical score for predicting pre-test probability followed by objective testing for DVT are of huge importance. Proximal DVT is life threatening and can be treated effectively with anticoagulants. The requirements for a safe diagnostic strategy should be based on an overall post-test incidence of DVT and pulmonary embolism (Venous Thromboembolism: VTE) of less than 1% during 3 months follow-up. As compared to venography [2], a normal or negative two point compression ultrasonography in the groin and popliteal region (2- CUS, Figure 1) has a similar high specificity and negative predictive value of 98-100% for proximal DVT but overlooks calf vein thrombosis (distal DVT). Two large management studies in 1998 showed that the post-test incidence of VTE after a first negative 2-CUS in patients with suspected DVT was very low, 1.7 and 2.9% with a negative predictive value of 98 and 97% respectively (Table 1) [3,4] indicating the need to perform a second 2-CUS on day 7, which was positive in 1.1 and 2.3% respectively and 0.6% slipped through the two CUS evaluations. Therefore, the negative prediting value of 99.4% of repeated 2-CUS testing appears to be effective but costly [3,4].
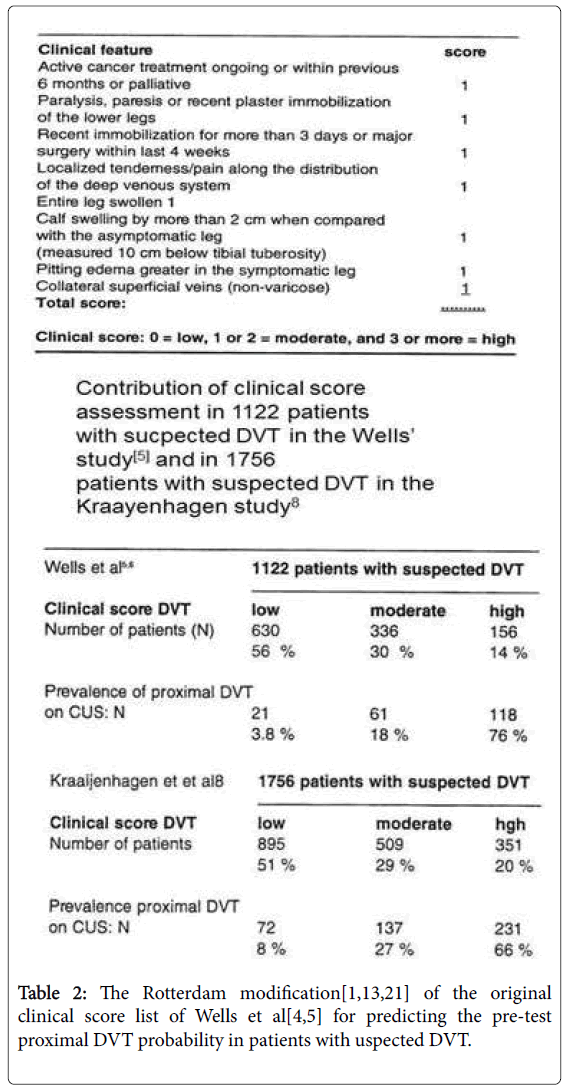
Based on a checklist of 8 clinical features 2 by an experienced clinician, the pretest clinical probability according to the Rotterdam modification of the Wells’ clinical score for proximal DVT (Table 2) could be estimated as low, moderate and high [1,5-7]. The incidence of proximal DVT in the low, moderate and high clinical score group was 3.8%, 18% and 76% and 56%, 30% and 18% of 1122 patients with suspected DVT in the original Wells’ studies belonged to the low, moderate and high clinical score group respectively (Table 2) [5,6]. The incidence of proximal DVT in the low, moderate and high clinical score group was 8%, 27% and 66% and 51%, 29% and 20% of 1756 patients with suspected DVT belonged to the low, moderate and high clinical score group respectively in the Kraayen hagen study (Table 2) [8]. The combination of a first negative 2-CUS and low clinical score (asymptomatic according to the check list) in the study of Wells excluded DVT with a post-test prevalence of 0.3%, thus obviating the need for serial 2-CUS testing (Figure 1). Patients with a first negative 2-CUS and moderate to high clinical score (symptomatic) the incidence of DVT on repeated 2-CUS testing was 3.8% indicating the need for repeated 2-CUS testing or the use of a D-dimer test. This strategy could reduce the number of repeated 2-CUS testing by 63% (Figure 1)[1,6,8,9,10].
Kraayen hagen et al. demonstrated that the combination of a first negative 2-CUS and a negative qualitative Simplired D-dimer test reduced the post-test incidence from 2.1% after serial 2-CUStesting to <1% without the need of repeated 2-CUS testing on the basis of which anticoagulation therapy could be safely withheld (Figure 1)[1,8]. This strategy reduced the number of repeated 2-CUS testing from 77% to 30%. Patients with a first negative 2-CUS and a positive Simplired Ddimer test are candidates for serial CUS testing.
Michiels, Maasland, Moossdorff and Schroyens performed between 1998 and 2002 a pilot study in 1046 patients with suspected DVT and could demonstrate that the combination of a first negative 2-CUS and an ELISA VIDAS D-dimer of less than 500 ng/L excluded both DVT and PE (VTE) with a sensitivity and negative predictive value of 99.9% irrespective of clinical score assessment (unpublished data, Figure 2) [11]. The combination of a first negative 2-CUS and an ELISA VIDAS test result of Figure 2)[11]. The combination of the ELISA VIDAS D-dimer measurement of Figure 2) [12-17]. The combination of a negative qualitative D-dimer test (Simplify R) and low clinical score without CUS testing is not safe enough to exclude DVT in routine daily practice [13,15]. A first negative CUS and a negative sensitive D-dimer test (ELISA VIDASR5,6,9] with a D-dimer level of VIDASR 11], Tinaquant R 12] or negative Simplify R test [8] indeed did safely exclude deep vein thrombosis with a NPV of near to 100% in prospective outcome studies (Table 3) [11-15]. Patients with persistent suspicion of DVT after a first 2-CUS and/or increased D-dimer levels (VIDASR >1000 ug/ml, Tinaquant R>500 ug/ml, positive Innovance, HemosIL Sta Lia test or Simplify R) are candidates for repeated CUS of the legs after one week [1,13-18].

Figure 2: The 2002 Rotterdam ERASMUS deep vein thrombosis (DVT) study design and results in the first cohort of 1069 patients with suspected deep vein thrombosis (DVT) safely exclude and diagnosed DVT with a sensitivity and specificity near to 100 % by the sequential use of CUS, D-dimer testing and clinical score assessment. A negative ELISA VIDAS D-dimer (
| First 2-CUS to diagnose DVT | N | Percent | |||
|---|---|---|---|---|---|
| Total number of outpatients with suspected DVT | 1330 | 100% | |||
| First 2-CUS positive for DVT | 271 | 20.40% | |||
| Proximal DVT | 239 | 18.00% | |||
| Distal Subpopiteal Thrombosis | 32 | 2.40% | |||
| First and Second 2-CUS positive for DVT 271 ± 25 | 296 | 22.30% | |||
| Test performance for DVT exclusion | Sens | Spec | NPV | ||
| First CUS negative irrespective of DD | 97.4 | 79.60% | 97.50% | ||
| VIDAS DD negative99.30% 36.20% 99.50% | |||||
| VIDAS DD93.30% 66.20% 97.40% | |||||
| VIDAS DD99.10% 66.50% 99.10% | |||||
| First 2-CUS negative for DVT | 1059 | 100% | |||
| Alternative diagnosis (AD): | |||||
| Bakers Cyste | 33 | 3.10% | |||
| Muscle hematoma | 27 | 2.50% | |||
| Old DVT | 21 | 2.00% | |||
| Superficial thrombophlebitis | 83 | 7.80% | |||
| Total AD on first negative 2-CUS | 154 | 14.50% |
Conclusion: A first E-CUS in 1330 patients with suspected deep vein thrombosis (DVT) was positive for proximal DVT in 18%, distal DVT in 2.4% and alternative diagnosis in 11.6%.
Table 3: Diagnosis and exclusion of deep vein thrombosis (DVT) and alternative diagnosis (AD) by the sequential use of two points compression ultrasonography (2-CUS) and the sensitive ELISA VIDAS D-dimer assay irrespective of clinical score assessment in the Rotterdam Erasmus DVT study [15].
2-CUS versus Complete CUS (CCUS), ELISA D-dimer and clinical score
2-CUS for the diagnosis of symptomatic proximal DVT overlooks calf vein thrombosis (CVT) and isolated thrombi in the femoral and iliac veins [3-7]. One fourth to one third of CVT do progress into a more proximal DVT within one week indicating the need to repeat 2- CUS within one week, which is not cost-effective (Table 1) [3,4,8,19]. Extended CUS to the subpopliteal trifurcation area (E-CUS, Figure 3) still overlooks calf vein thrombosis [19-21]. Complete compression ultrasonography (CCUS, Figure 3) examination of all deep veins from the groin to the ankle in a single procedure will pick up both proximal DVT and isolated subpopliteal and CVT and alternative diagnoses (AD) [22-25]. We used since 2005 CCUS in the setting of Primary Care Medicine by skilled, specially trained echo graphists for examining leg vein thrombosis from the groin to the fossa polplitea (Figure 3) [15]. The patient must sit upright with legs hanging down to maximize venous filling of the calf veins. In this position CCUS was applied to identify venousthrombosis in the popliteal, posterior tibial, personal, gastrocnemius (medial and lateral) and the soleal (lateral and medial) veins. The accuracy of CCUS for the diagnosis of acute distal and proximal DVT was high with a negative predictive value (NPV) of 99.5% in four large management studies with a prevalence of DVT from 14%–33% (Table 4) [22-25]. The prevalence of all DVT, proximal DVT and distal DVT in 3240 patients with suspected DVT were 20.2%, 10.0% and 10.2% respectively (Table 4) [10-13]. Of the 1772 patients included in the MASTER registry for the presence of DVT in the lower limbs, 170 (9.6%, range zero to 24%) had an isolated CVT on CCUS examination [26].
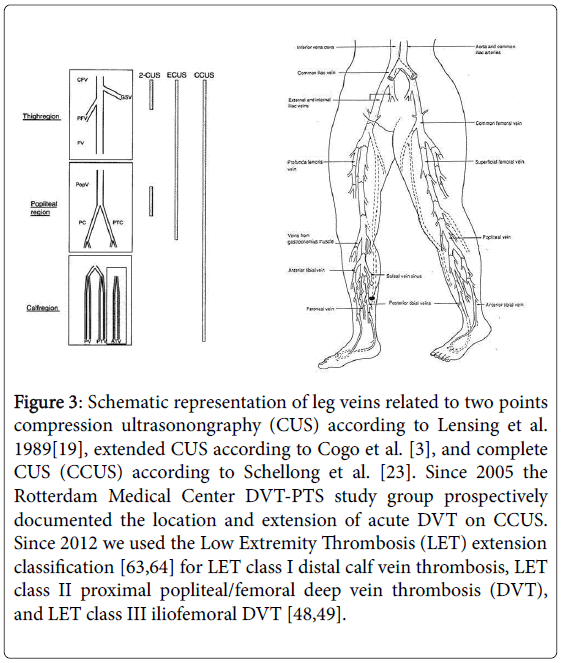
Figure 3: Schematic representation of leg veins related to two points compression ultrasonongraphy (CUS) according to Lensing et al. 1989[19], extended CUS according to Cogo et al. [3], and complete CUS (CCUS) according to Schellong et al. [23]. Since 2005 the Rotterdam Medical Center DVT-PTS study group prospectively documented the location and extension of acute DVT on CCUS. Since 2012 we used the Low Extremity Thrombosis (LET) extension classification [63,64] for LET class I distal calf vein thrombosis, LET class II proximal popliteal/femoral deep vein thrombosis (DVT), and LET class III iliofemoral DVT [48,49].
| All DVT | Prox DVT | Dist DVT | ||||
|---|---|---|---|---|---|---|
| Elias[22] | 204/623 | 32.80% | 112/623 | 18% | 92/623 | 14.8.1% |
| Schellong[23] | 275/1646 | 16.70% | 121/1646 | 7.40% | 154/1646 | 9.40% |
| Stevens [24] | 61/445 | 13.70% | 42/445 | 9.40% | 19/445 | 4.30% |
| Subramaniam[25] | 113/526 | 21.50% | 49/526 | 9.30% | 64/526 | 12% |
| Total | 653/3240 à 20.1% | 324/3240 à10% | 329/3240 à 10.2% | |||
DVT=deep vein thrombosis; Prox=proximal; Dist=distal.
Conclusion: A first complete CUS (CCUS) in 3249 patients with suspected deep vein thrombosis (DVT) in four prospective studies was positive for proximal DVT in 10%, distal DVT in 10,2% and for all DVT in 20.1%.
Table 4: Proportion of positive findings on complete compression ultrasonography (CCUS) in four large cohorts of symptomatic patients with suspected DVT undergoing CCUS of the proximal and distal veins.
As compared to proximal DVT, CVT patients were significantly younger and displayed the usual signs/symptoms (pain, edema, erythema) less often at presentation. Recent surgery or trauma more frequently elicited CVT and cancer was less frequent than in proximal DVT patients. Symptomatic pulmonary embolism (PE) was present in a higher proportion of CVT 26.5% vs. proximal DVT patients 19.9%, respectively (p<0.05).
We recently found a 26% incidence of CVT testing by CCUS in our large prospective 2005-2016 Rotterdam Erasmus Tower study of 3830 patients with suspected DVT. DVT including CVT on CCUS was found in 14.5% and alternative diagnosis in 17% of 3383 patients suspicious for leg vein thrombosis. The rapid ELISA Vidas of Figures 4 and 5, manuscript in preparation).
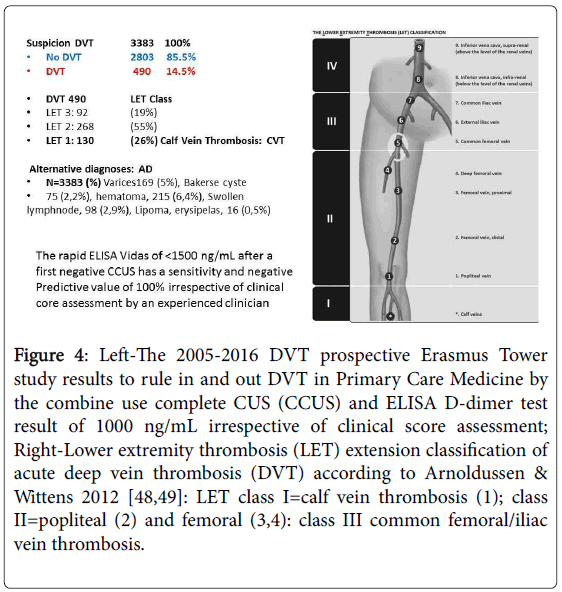
Figure 4: Left-The 2005-2016 DVT prospective Erasmus Tower study results to rule in and out DVT in Primary Care Medicine by the combine use complete CUS (CCUS) and ELISA D-dimer test result of 1000 ng/mL irrespective of clinical score assessment; Right-Lower extremity thrombosis (LET) extension classification of acute deep vein thrombosis (DVT) according to Arnoldussen & Wittens 2012 [48,49]: LET class I=calf vein thrombosis (1); class II=popliteal (2) and femoral (3,4): class III common femoral/iliac vein thrombosis.

Figure 5: The Rotterdam ERASMUS DVT Simplification of algorithm 2018.
Diagnosis and prevention of Post-Thrombotic syndrome (PTS)
The Clinical-Etiology-Anatomic-Pathophysiologic (CEAP) classification (Table 5) for PTS is widely applied by dermatologists, phlebologists, surgeons and epidemiologists [27]. In 1992, Prandoni developed in the 1990s a standardized scale for the assessment of PTS in post-DVT legs [28]. Each subjective sign and objective symptom of PTS was scored as 0, 1, 2 or 3 based on subjective judgement [28].
| Classification | Symptom |
|---|---|
| Clinical: C | |
| C0 asymptomatic | No visible varicose veins |
| C1 | Spider or reticular veins |
| C2 | Varicose veins |
| C3 | Oedema |
| C4a | Pigmentation or eczema |
| C4b | Lipodermatosclerosis or atrophie blanche |
| C5 | Skin changes with healed ulceration |
| C6 | Skin changes with active ulceration |
| Symptomatic | Symptomatic, including aches, pain, tightness, skin irritation, heaviness, muscle cramps, and other complaints attributable to venous dysfunction |
| A | Asymptomatic |
Abbreviations: CEAP: Clinical Etiology Anatomic Pathophysiological; E: Etiology; A: Anatomic; P: Pathophysiological; C: Clinical
Table 5: Clinical (C) part of the CEAP classification for severity of chronic venous insufficiency either primary or secondary see E, A and P parts: EAP)[27].
The 5 signs and 7 symptoms of the original Prandoni score are taken over unchanged by PTS investigators and trialists as the Villalta (Table 6) [29-32]. The evaluation of the Villalta scale for PTS severity grading in the Prandoni et al., COX and IDEAL studies started at 6 months post-DVT by lumping the subjective complaints and objective skin lesions for mild, moderate and severe postthrombotic syndrome (PTS, Table 6). Wik et al. introduced the principle of patient self-reported Villalta scale and demonstrated that the Villalta scale evaluation by a physician, nurse and patient self-reported Villalta scale are quite similar [33]. By adding a visual guide on objective PTS skin lesions in self-reported Villalta scale the results of the Villalta score at 1 to 2 years post-DVT correlated well with disease specific VEINES-QOL and VEINES-SYM scores [31,32]. As no differences in general mental health quality of life score between post-DVT patients with and without PTS was observed, this simple means that patients with severe PTS not complicated with leg ulcers (Villalta score <10) usually enjoy a normal mental and physical health status in contrast to severe PTS patients (Villalta score above 10) who experience leg failure problems like restricted walking distances and painful legs during standing. We conclude that the lumping subjective and objective signs and symptoms by the Villalta score do not reflect the underlying etiology and pathophysiology of PTS and underestimates the clear indications to treat objective signs of reflux, obstruction, progressive skin lesions and ulceration. The Villalta scales of no mild versus moderate PTS do not differentiate between primary venous insufficiency or varicosis versus post-DVT venous insufficiency and secondary varicosis. It is mandatory to validate the Villalta scoring system of subjective signs and objective symptoms scoring system of early PTS against the objective ‘C’ grading of the CEAP scoring system (Table 5) at 6 and 12 months post-DVT up to 2 to 5 year’s post-DVT in prospective management studies (Table 6). This statement is of particular interest, since literature data are convincingly showing that mild to moderate PTS is present in about 50% of post-DVT patients at time point one to two years post-DVT using the broad spectrum mild-moderate-severe Villalta score results between 5 and more than 15 [1,32]. The objective symptoms of the Villalta score all belong to the C of CEAP (Table 6). The clinical skin lesions, the C of CEAP, start to appear at 6 and 12 months post-DVT. The Rotterdam multidisciplinary DVT PTS working Group of primary care physicians, internists, radiologists and echographists decided to use the clinical (C) criteria of the CEAP classification for objective grading of PTS (Table 6). The C of CEAP for the objective grading of leg swelling and skin lesions can easily be assessed at 1, 3 and 6 months and 1 to 2 years post-DVT.
| Fives subjective symptoms | Seven objective sign: | All belong to C | |
|---|---|---|---|
| S of CEAP | C of CEAP[27] | ||
| Heaviness of the foot/leg | Pretibial oedema | C3 | |
| Pain in calf/thigh | Induration of the skin | C4 | |
| Cramps in calf/thigh | Hyperpigmentation | C4 | |
| Pruritus | New venous ectasia | C2 | |
| Paraesthesia | Redness | C1 | |
| Pain during calf compression (post DVT) | |||
| Ulceration of the skin | C5, C6 | ||
| Each sign or symptom is graded with a score as 1, 2, or 3. | |||
| (1=mild, 2=moderate, 3=severe). Ulceration of the skin 4 points | |||
| The presence leg ulcer is a late complication of PTS consistent with severe CVI, C 5, 6. | |||
| Grading of the clinical severity of post-thrombotic syndrome (PTS) according to Villalta score | |||
| Absent: | score < 5 | ||
| Mild-to-moderate: | score between 5 and 10 and 10 to 15 respectively at 2 consecutive visits | ||
| Severe: | score >15 at 2 consecutive occasions | ||
| The Rotterdam Antwerp modification of the Villalta scoring system is an ordered use of the C of CEAP clinical symptoms and signs by primary care physician, internists, radiologists, surgeons and dermatologists. | |||
| The Villalta scoring system is not suitable for use at time of acute deep vein thrombosis (DVT) and during serial CCUS at 1 to 3 months post-DVT. The combined use of the Villalta and the C of CEAP scoring systems are suitable for assessment of PTS at 6 to 12 months and subsequent follow-up for 2 to several years post-DVT for the assessment of the appearance, persistence, increase and decrease of mild, moderate and severe PTS manifestations | |||
Abbeviations: CEAP: Clinical Etiology Anatomic Pathophysiological; E: Etiology; A: Anatomic; P: Pathophysiological; C: Clinical
Table 6: Translation of the Villalta clinical scoring system into the Rotterdam Antwerp modification of the clinical (C) objective criteria of the CEAP classification [27] for the assessment of the postthrombotic syndrome (PTS). In all clinical studies PTS assessment started at 6 to 12 months post-DVT [28-30].
The need to prevent of DVT recurrence as the main cause of PTS
The risk of recurrent VTE in unprovoked DVT patients after shortterm (3 to 6 months) OAT treatment varies from 5% to 15% in the year following discontinuation of OAT with a long-term yearly risk of VTE recurrence of 2 to 4% and a cumulative estimated 8 year risk near 45% (blue line Figure 6) [34]. The risk of recurrent VTE in unprovked DVT patients after long-term OAT treatment is somewhat less but remains high (rate of recurrence after long-term OAT) [34] indicating the need for anticoagulant extension in about one third of post-DVT patients [34-36]. Labropoulos et al. (2003) defined venous reflux in lower ectremity veins as a main cause of PTS. The cutoff values for reflux in the superficial and deep calf veins must be greater than 500 milliseconds (ms) [37]. The reflux cutoff value for the femoropopliteal veins should be greater than 1000 ms. Outward flow in the perforating veins should be considered abnormal at greater than 350 ms [37]. In the clinical study of Labropoulos et al. [38] half of the patients with isolated acute DVT became asymptomatic, whereas all acute DVT patients with extended DVT remained symptomatic during follow-up in the post DVT period.
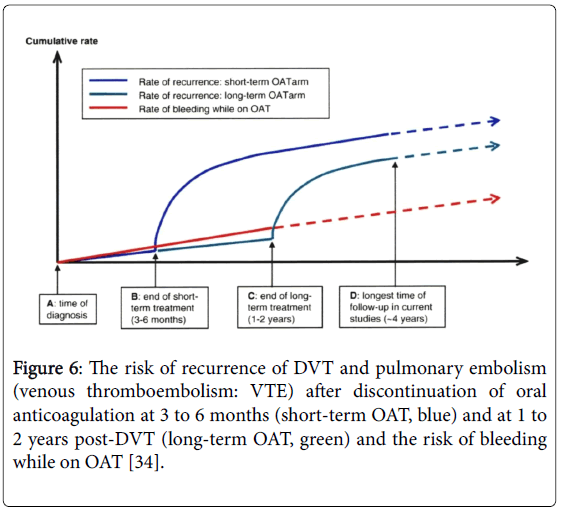
Figure 6: The risk of recurrence of DVT and pulmonary embolism (venous thromboembolism: VTE) after discontinuation of oral anticoagulation at 3 to 6 months (short-term OAT, blue) and at 1 to 2 years post-DVT (long-term OAT, green) and the risk of bleeding while on OAT [34].
Reflux, obstruction, or a combination was more common in extended proximal extended DVT than in isolated thrombosis in one segment of the leg vein [38]. Recurrent DVT and PTS skin damage are more likely to develop in extended DVT than in those with DVT in a single vein segment. Patients with reflux and obstruction presented more skin damage than those with reflux or obstruction alone. DVT extending from calf vein to proximal femoral veins produced the highest PTS prevalence [1,38,39]. Rodger et al. developed a clinical decision rule (CDR) for the risk of VTE recurrence derived from 646 patients with a first unprovoked VTE treated with OAT for about 6 months and followed for recurrent VTE after OAT discontinuation [34-36]. PTS signs as assessed by the presence of Hyperpigmentation (C4), Edema (C3) and Redness (HER) plus D (VIDAS D-dimer) appeared to make biological and clinical sense as important risk factors for DVT recurrence and embolic complication (Table 7) [36]. The REVERSE 2 study design in Figure 7 did not quantify HER by clinicians according to the objective clinical (C) criteria of the CEAP classification (Table 4) and the two O of Obesity BMI >30 and older age of HERDOO2 are not-VTE specific risk factors for DVT recurrence (Figure 7). The VIDAS D-dimer cut-off of 250ng/mL was measured during just before discontinuation of anticoagulation (Figure 7). The REVERSE 2 did not take the unique opportunity to compare VIDAS D-dimer measurements during anticoagulation versus one month after discontinuation anticoagulation according to the PROLONG and VIENNA DVT recurrence prediction studies (Table 7). Prospective studies on LET evaluation at time of acute DVT, and the combined use of objective clinical ‘C of CEAP’ (Table 6) and VSCC scoring systems related to reflux and RVP on serial CUS should be used on top of the ‘C’ of CEAP. According to our experiences anno 2018 it is mandarory to measure of quantitative D-dimer levels at time of acute DVT, before and one month after anticoagulant discontinuation between 6 to 12 months post-DVT.

Figure 7: The HERDOO2 study design, classification and outcome of anticoagulant treatment (bloodthinners) in 2779 patients with a first unprovoked deep vein thrombosis [36].
| HERDOO2 | Vienna Model Palateri Model | DASH Score | |
|---|---|---|---|
| Author | Rodger et al.[36] | Eichinger et al.[59] | Tosetto et al.[60] |
| Number of patients | 646 | 929 | 1818 |
| Patient cohort | Prospetive | Prospective | Meta-analysis |
| Predictive variables | Men: no | Gender | Abnormal D-dimer |
| Women: | Distal vs Prox DVT | after anticoagulation | |
| Age > 60 years | D-dimer after | Age | |
| PTS HER | anticoagulation | Male gender | |
| BMI >30 kg/m2 | PROLONG | Hormonal therapy | |
| D-dimer >250 ug/L | DULCIS | ||
| Age >65 yrs | Palareti | ||
| Recurrence risk | < 180 points (nomogram | ||
| Low risk | 1.60% | 4.40% | 3.10% |
| 95% CI | 0.3-4.6% | 2.7-6.2% | 2.3-3.9% |
Table 7: Prediction models to asses the recurrence risk of deep ven thrombosos (DVT and pulomonary embolism (PE) after discontinuation of antiocoagulation in patients with a first unprovked DVT.
Medical elastic stockings (MECS) for acute DVT and PTS
About one of every three to four post-DVT patients will develop PTS sequelae within one to two years, which are frequently moderate to severe and produce considerable socioeconomic consequences [40,41]. The incidence of asymptomatic post-DVT patients in the control arm of two randomized clinical trials (Prandoni et al., COX and IDEAL) comparing below knee MECS versus No MECS using the Villata score cut-off of 42,44]. The main disadvantage of these MECS studies was that they did not compare the Villata score with objective measurement PTS objectively by the C of CEAP score (Tables 5 and 6) and reflux on CUS. Wearing MECS versus no wearing MECS in the Prandoni study revealed an overall increased PTS Villalta score (cut-off >5) in 50% for those randomized for No MECS and 25% for those randomized for MECS at time points 6 months post-DVT and there was no further decrease of Villata score between 6 month and 2-year follow-up (Figure 3) [42]. MECS only reduced the subjective signs (Table 8, left), but did not reduce the objective clinical skin lesions of the C symptoms of CEAP) (Table 8, right) at time points 6 months, 1 year and 2 years post-DVT. This conclusion was overlooked and misinterpreted by Prandoni in his publication in 2004 [42]. Michiels recognized this novel insight in Table 8 in 2016 that wearing MECS does not alter the objective signs of PTS. The recommendation derived from the Prandoni MECS study (2004) to wear MECS for 2 years after acute DVT has lead to an enormous overtreatment with MECS in the past 20 years because half (about 50%) of post-DVT patients do not have any sign of PTS. The other half post-DVT patients, who develop PTS wearing MECS will only reduce subjective signs with persistence of objective PTS signs related to underlying venous pathology at 6 to 12 months post-DVT.
| Time | Patients N | Subjective symptoms | Objective signs | ||
|---|---|---|---|---|---|
| MECS/No | MECS/No | MECS | No MECS | MECS | No MECS |
| N/N | OR versus controls | OR versus controls | |||
| 3 months | 90 / 90 | 0.78 ± 1.05 | 2.16 ± 2.14 | 3.14 ± 2.25 | 3.37 ± 1.96 |
| 6 months | 90 / 90 | 0.96 ± 1.21 | 2.54 ± 2.12 | 2.81 ± 2.21 | 3.02 ± 2.22 |
| 1 yr | 89 / 89 | 0.79 ± 1.29 | 2.28 ± 2.08 | 2.45 ± 2.27 | 3.02 ± 2.22 |
| 2 yr | 85 / 81 | 1.00 ± 1.35 | 2.51 ± 2.28 | 2.29 ± 2.18 | 2.52 ± 2.11 |
| 3 yr | 82 / 76 | 0.63 ± 0.96 | 2.11 ± 2.00 | 1.84 ± 2.13 | 2.43 ± 2.29 |
| 4 yr | 68 / 58 | 0.63 ± 0.96 | 2.48 ± 1.96 | 1.78 ± 1.92 | 2.47 ± 1.96 |
| 5 yr | 35 / 29 | 0.54 ± 0.82 | 2.34 ± 1.84 | 1.83 ± 2.08 | 2.45 ± 1.53 |
Source Prandoni et al. AnnInt Med 2004;141:249-256[42]
Table 8: Significant reduction of subjective symptoms score but no change in objective signs for post-thrombotic syndrome in the randomized clinical trial of below-knee medical elastic compression stockings (MECS) versus no MECS when the Villalta scoring was separated into subjective symptoms and objective signs (Table 4) for the assessment of the effect of MECS on PTA in the original study of Prandoni et al.[42].
The randomized placebo controlled SOX trial compared the outcome of active versus placebo MECS used for 2 years to prevent PTS after a first event of proximal DVT [43]. From 2004 to 2010, 410 patients were randomly assigned to receive active MECS and 396 placebo stockings (PS). The primary objective outcome (Ginsberg’s criteria for severe PTS) and the secondary subjective outcome according to Villalta scale (Table 4) were assessed at 6 months, 1 and 2 years post-DVT. Ginsberg’s objective criteria included ipsilateral pain and swelling of at least 1 month’s duration that are typical in character for overt PTS: worse at the end of the day or with prolonged sitting or standing, and better after a night’s rest and leg elevation. Cumulative incidence of objective PTS (at 2 years) was 14.2% in active MECS versus 12.7% in placebo stockings (PS) (hazard ratio 1.13 95% CI 0.73-1.76; p=0.58). Cumulative incidence of overall mild moderate and severe PTS by Villalta’s criteria (Villalta clinical score ≥ 5 mild, >10 moderate or severe including ulcer (>15) between 6 months and subsequent visits for 2 years) was 52.6% in active MECS versus 52.3% in placebo stockings (hazard ratio 1.00, 95% CI 0.81-1.24; p=0.96 [43]. Symptomatic PTS patients in particular when complicated by edema are candidates for relief of symptoms by MECS. The overall DVT recurrences in three randomized clinical trials (Brandjes et al, Prandoni et al. and COX) were 59 (10%) 64 (11%) in 596 post-DVT patients wearing MECS versus 64 (11%) in 584 wearing no-MECS during 2 years follow-up demonstrating that wearing MECS did not reduced the VTE recurrence rate (Table 9) [41-43].
| Acute DVT | MECS | No MECS | |||||
|---|---|---|---|---|---|---|---|
| Study | N | N | N | DVT recurrence | N | N | DVT recurrence |
| Brandjes et al.[41] | 194 | 96 | 14 | 14.60% | 98 | 13 | 13.30% |
| Prandoni et al.[42] | 180 | 90 | 12 | 12.30% | 90 | 13 | 14.30% |
| Kahn et al.[43] | 806 | 410 | 33 | 8% | 396 | 38 | 11% |
| Total | 1180 | 596 | 59 | 10% | 584 | 64 | 11% |
Table 9: VTE (mainly DVT) recurrence rate in three randomized clinical trials comparing overtreatment with medical elastic stockings: MECS versus no MECS during 2 years after acute DVT.
Ten Cate-Hoek performed the IDEAL (individualised versus standard duration of elastic compression stocking) study, a multicenter randomized non-inferior clinical trial comparing MECS vs. No MECS post-DVT for 2 years at 12 hospitals (Figure 8) [44]. The IDEAL study enrolled 865 patients and randomly assigned 437 to individualized duration of MECS and 428 to standard duration of MECS for symptomatic PTS (Villata score >4). Out of 432 patients in the intervention group 283 (66%) were advised to stop MECS before 24 months of whom (236 [55%] of 432 patients had stopped MECS after 6 months, and 47 [11%] at 12 months (Figure 8). Post-thrombotic syndrome in the IDEAL study occurred in 125 (29%) of 432 patients receiving individualized duration of therapy and in 118 (28%) of 424 receiving standard duration of therapy for 2 years [44].
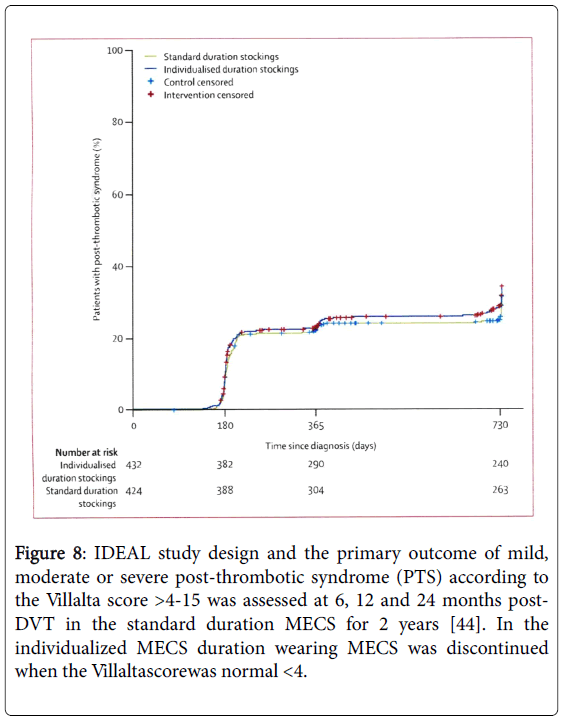
Figure 8: IDEAL study design and the primary outcome of mild, moderate or severe post-thrombotic syndrome (PTS) according to the Villalta score >4-15 was assessed at 6, 12 and 24 months post- DVT in the standard duration MECS for 2 years [44]. In the individualized MECS duration wearing MECS was discontinued when the Villaltascorewas normal <4.
No serious adverse events related to the MECS intervention occurred. The absolute difference in PTS frequency between standard duration MECS for 1 and 2 years versus individualized duration MECS was not different (hazard ratio 1.3 p=0.77). Distribution of severity of post-thrombotic syndrome was similar for both groups.
The IDEAL study confirmed the results of the COX study that individualized therapy with medical elastic compression stockings for the prevention of objective PTS symptoms was non-inferior to standard duration of therapy of 24 months. Shortening the length of stocking therapy as much as possible to those in whom relief of subjective PTS symptom can be reached will significantly enhance the wellbeing of post-DVT patients.
Bridging the gap between acute DVT, DVT recurrence and PTS
Three prospective clinical research studies on prevention of DVT recurrence and the risk of PTS clearly demonstrated that rapid and complete recanalization at time point 3 months post DVT complete recanalization and absence of PTS (normal CUS) did predict low risk on DVT recurrence, whereas delayed and incomplete recanalization at time point 3 months post-DVT is associated with high risk on reflux and the presence of mild to moderate PTS 12 months post-DVT [45-47]. Objective measurement of PTS according to the C of CEAP and the degree of recanalization and reflux on CUS at 1 and 3 months post-DVT are mandatory for the assessment of DVT recurrence and PTS in a prospective safety-outcome study [45-50]. A large prospective study of 313 consecutive DVT patients evaluated residual vein pathology (RVP) on repeated CUS of common femoral and popliteal veins at 3, 6, 12 24 and 36 months post DVT [47]. The cumulative incidence of normal CUS (complete recanalization, no residual venous pathology: RVT) was 39%, 58%, 69% and 74% at 6, 12, 24 and 36 months post DVT respectively. Of 58 DVT recurrent episodes, 41 had abnormal CUS (RVT+). The hazard ratio for recurrent DVT was 2.4 for persistent RVT+ as compared to complete vein renalization (RVT-) [47]. Consequently, serial CUS assessment at 1, 3 and 6 months post- DVT followed by objective PTS assessment (C of CEAP) at 6 months 1 year and 2 years post-DVT is mandatory to study the relation between Lower Extremity Thrombosis (LET) extension on CCUS and the development of PTS in prospective clinical safety outcome studies (Figure 9) [48-51]. LET extension on CCUS at time of acute DVT and subsequent assessment of PTS using physical examination and the C of CEAP by clinicians and the Villata scores by patient’s self-assessment on top of flow duplex ultrasound should be performed in routine clinical practice at 1 month, 3 and 6 months, one year and two years post-DVT. About half of the post-DVT patients who have normal CCUS 3 months post-DVT do not develop PTS after 3, 6 to 9 months post-DVT obviating wearing MECS and anticoagulation at 6 months post-DVT (Figure 9, study arm1). Asymptomatic post-DVT patient with complete recanalization, no reflux, and no PTS at 6 to 9 months post-DVT develop; both wearing MECS and anticoagulation can dediscontinued (Figure 9). In case reflux of the deep venous system is found at 3 or 6 months post-DVT, wearing MECS and oral anticoagulation (VKA or NOAC) should be continued for 1 to 2 years (Figure 9) [51].
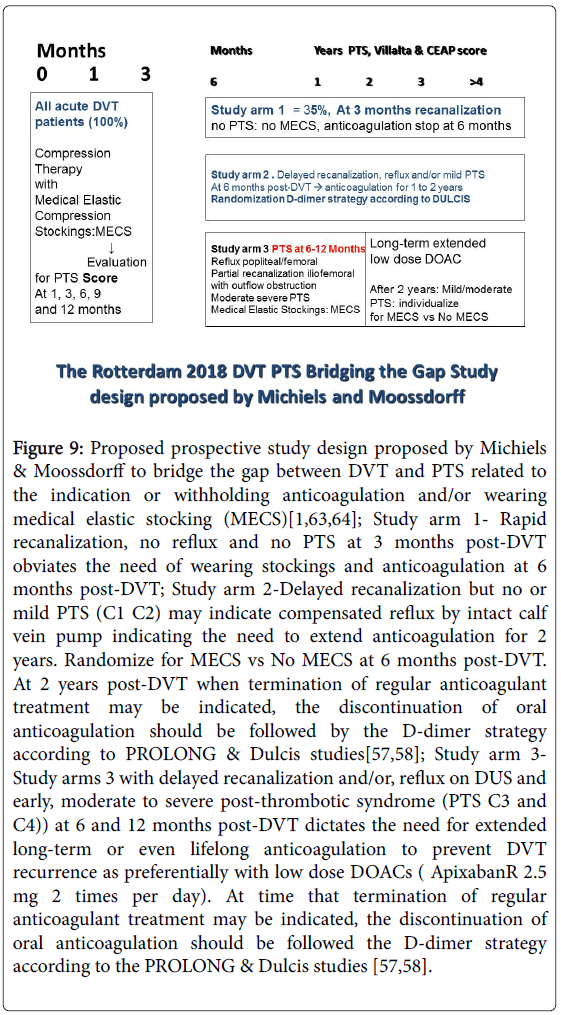
Figure 9: Proposed prospective study design proposed by Michiels & Moossdorff to bridge the gap between DVT and PTS related to the indication or withholding anticoagulation and/or wearing medical elastic stocking (MECS)[1,63,64]; Study arm 1- Rapid recanalization, no reflux and no PTS at 3 months post-DVT obviates the need of wearing stockings and anticoagulation at 6 months post-DVT; Study arm 2-Delayed recanalization but no or mild PTS (C1 C2) may indicate compensated reflux by intact calf vein pump indicating the need to extend anticoagulation for 2 years. Randomize for MECS vs No MECS at 6 months post-DVT. At 2 years post-DVT when termination of regular anticoagulant treatment may be indicated, the discontinuation of oral anticoagulation should be followed by the D-dimer strategy according to PROLONG & Dulcis studies[57,58]; Study arm 3- Study arms 3 with delayed recanalization and/or, reflux on DUS and early, moderate to severe post-thrombotic syndrome (PTS C3 and C4)) at 6 and 12 months post-DVT dictates the need for extended long-term or even lifelong anticoagulation to prevent DVT recurrence as preferentially with low dose DOACs ( ApixabanR 2.5 mg 2 times per day). At time that termination of regular anticoagulant treatment may be indicated, the discontinuation of oral anticoagulation should be followed the D-dimer strategy according to the PROLONG & Dulcis studies [57,58].
Lower Extremity Thrombosis (LET) extension of acute DVT: therapeutic implication
The 2012 guidelines of the Society for Vascular Surgery and the American Venous Forum recommended precise terminology for exact location of acute DVT: isolated calf vein, popliteal-femoral, calf vein with extension into popliteal-femoral or iliofemoral veins and isolated iliofemoral with or without extension into inferior vena cava (Figure 8) [52-55]. The LET classification has been designed based on the hemodynamic hypothesis that the severity of acute DVT and the risk on PTS or DVT recurrence is related the most cranial level of thrombus extension: the higher the LET class the higher PTS incidence and severity and the lower quality of life (Figure 8)[52-55].
De Maeseneer et al. [53] investigated LET class extension in 1338 adult patients with unilateral acute distal and proximal DVT on CCUS, aged above 18 years and collected between 1992 and 2014 at the University Hospital Hospital Antwerp Belgium (Table 10). Out of 1338 patients, a one segment DVT was seen on CCUS in 433 (33%) patients of whom 370 had CVT (27.6%). CVT localization included posterior and anterior tibial vein, peroneal vein, gastrocnemius vein and soleus vein. The distribution of thrombus extensions of proximal DVT present in 945 (according to 2012 guidelines [52] and LET classification [48,49]) is shown in Table 7. Two, three four and five segments of leg vein thrombosis extensions on CCUS were seen in 208 (16%), 345 (26%), 149 (11%) and 193 (14%) respectively. The single segment vein thrombosis in 63 acute proximal DVTs patients were located in the popliteal vein (PV) in 3), in the femoral vein (FV) in 37 FV), in the common femoral vein (CFV) in 25, and in the iliofemoral vein (IFV) in 8 patients. If thrombus is limited to one segment it must be initiated in that segment. Thrombus formed restricted to segment level 5 or 4+5 was detected in 126 (9%), to segment 3+4+5 in 67 5%) and to segment 2+3+4+5 in 20 (1.5%) acute proximal DVT patients without calf vein thrombosis (Table 10). The pathophysiology of isolated DVT and of restricted DVT in segments 2, 3 or 4 without CVT is probable related to local causes like extension from ascending superficial thrombosis or thrombo phebitis or perforating veins into the deep venous system.
| LET extension / DVT on CCUS | Number/% of total | ||
|---|---|---|---|
| LET I | |||
| Distal calf VT: segment 1 | 370 | 0.27 | |
| Proximal DVT | 968 | 0.68 | |
| 1 segment either PV, FV, CFV or IV (CVT) | 63 | 0.047 | |
| 2 segments | 208 | 0.16 | |
| 3 segments | 345 | 0.26 | |
| 4 segments | 149 | 0.11 | |
| 5 segments | 193 | 0.14 | |
| Proximal DVT starting at the level of CVT | 502 | 0.375 | |
| LET I/II | |||
| Segment 1+2 | CV PV | 111 | 0.083 |
| Segment 1+2+3 | CV PV FV | 267 | 0.2 |
| LET I/II/III | |||
| Segment 1+2+3+4 | CV PV FV CFV | 124 | 0.093 |
| LET II/III, no CVT | PV FV CFV and/or IFV | 241 | 0.18 |
| Proximal DVT | 945 evaluable cases | ||
| Femopopliteal DVT | 439 | 0.328 | |
| Iliofemoral DVT total | 506 | 0.38 | |
| Iliofemoral 1+2+3+4+5 | 157 (11.7%) | ||
| Iliofemoral no CVT | 189 (14%) | ||
| Iliofemoral no CVT no polpliteal | 160 (12%) | ||
Table 10: Lower Extremity Thrombosis (LET) extension in 1338 patients with unilateral first acute deep vein thrombosis (DVT) on complete compression ultrasonography (CCUS) [53].
Out of 1338 patients thrombus formation on CCUS started at the level of calf vein in 872 (65%) of whom 370 (32% LET) presented with CVT LET class I and 502 (37.5%) had extension into the proximal veins LET class I/II/III (Table 10). Only 160 (12%) with isolated iliofemoral acute DVT (LET class III) would have been considered as ‘ideal’ candidates for catheter directed thrombolysis (CDT) [55]. There was no involvement of proximal DVT of segment 2 in 67 (LET class III) and segment 1 (proximal DVT without CVT, LET class II/III) in 20 cases. Acute proximal DVT LET class II/III without involvement of calf or popliteal vein should also be considered as ‘ideal’ cases for CDT. A detailed description of thrombus extension on CCUS at time of presentation surely will allow a better risk prediction of DVT recurrence and PTS during follow-up for a few to several years. Strijkers retrospectively evaluated the clinical impact of the LET extension classification using a questionnaire follow-up in 1338 patients with unilateral acute DVT seen at the University Hospital Antwerp [53,55]. Out of 1338 eligible patients 668 patients were excluded because 277 had deceased, 391 reached the age of 80-plus years and 8 moved outside Belgium or The Netherlands. Only 660 patients were invited by mail to fill in the questionnaires and 315 responded (Table 11) [55]. The mean age in years at DVT diagnosis in 315 responders to the questionnaire was 50.6 +13.3 years. DVT was left sided in 56.2%. The risk factors for the first acute thrombotic event included malignancy (3.2%), pregnancy/postpartum (5.7%), immobilization/surgery (22.2%), trauma/fracture (11.7%), oral contraceptive use (4.8%), not specified (21.9%) and idiopathic (35.1%) in only one third of the 315 responding DVT patients (Table 11). In this retrospective study PTS was scored by means of an adapted version of a patient self-reported Villalta scale [33], Strijkers added a visual guide on PTS manifestations to the questionnaire of the clinical Villalta scale to ensure a correct assessment of the clinical situation by the patients themselves.
| LET claasification | Total | LET I | LET II | LET III | P-value |
|---|---|---|---|---|---|
| Extension DVT | (Figure 6) | CV | CV/FV | CV/FV/CF/IF | |
| FV or FV/CV | FV/CF/IF or CF/IF or IF | ||||
| Number of patients | 315 | 100 | 108 | 107 | ns |
| Age mean, years (yrs) | 50.1 | 51.4 | 49.9 | 49 | ns |
| BMI mean | 27.5 | 29.6 | 28.3 | 27.2 | 0.021 |
| Follow-up median yrs | 6.9 | 6 | 6.3 | 7.6 | |
| Villalta score median | 6 (3-11) | 4 (2-9) | 7 (3-12) | 6.5 (3-12.5) | 0.002 |
| DVT recurrence | 29.10% | 32% | 28.70% | 27.10% | ns |
| Ipsilateral | 18.70% | 19% | 28.70% | 27.10% | ns |
| Contralateral | 6% | 8% | 4.60% | 5.60% | ns |
| Bilateral | 4.40% | 5% | 3.70% | 4.70% | ns |
| Contra/bilat | 10.40% | 13% | 8.30% | 10.30% | |
| Still on anticoagulation | 51.70% | 38% | 54.70% | 61.70% | 0.002 |
| Still wearing MECS | 45.70% | 35% | 42.60% | 58.90% | 0.002 |
| Venous ulcers | 5.40% | 6% | 2.80% | 7.50% | ns |
| Family history: | |||||
| DVT | 27% | 33% | 23.10% | 57% | ns |
| Varicosis | 57.80% | 63% | 53.70% | 57% | ns |
| Comorbidity | 56.80% | 54% | 50.90% | 65.40% | |
Kruskal-Wallis test significance indicatedasP
Conclusion: DVT recurrence rate after longterm follow-up of is equally high and around 30% in LET class I, II and III acute DVT patients, but the Villata score, post-DVT patients still on anticoagulation and post-DVT patients still wearing MECS after long-term follow-up is significantly lower in LET class I(one-third) as compared to LET class II (around 50%) and LET class III (two-third) acute DVT patients. Source Strijkers et al.[54,55]
Table 11: Characteristics of 315 post-DVT patients after a median follow-up of 6.9 years at time of PTS Villalta score evaluation in Lower Extremity Thrombosis (LET) extension class I, versus class II and III DVT (P-value LET 1 vs II/III)[54,55].
As shown in Table 8, the median self-reported Villalta score and the number of patients still on anticoagulation and wearing MECS were significantly lower in LET class I versus class II/III DVT patients [55]. The distribution of LET classes was LET I in 97, LET I,II in 90, LET II in 17, LET III in 16, LET II,III in 26, and LET I,II,III in 63 acute DVT patients (Figure 10) [55]. Mild and moderate PTS do not differ between the six different LET classes. Significantly higher rates of severe PTS was present in LET class II and LET III vs. LET class I (P=0.012), and in LET class I,II,III versus LET class I (p=0.002). Overall, Strijkers found a two- to threefold higher risk for developing severe PTS for patients with LET class II or LET class III compared to patients with LET class I at time of DVT diagnosis. In this study, quality of life scored by VEINES-Qol declined with increasing LET class extension from class I to class II and III (Figure 11) [55]. CVT was complicated by PTS in 37% after long term follow-up. Relative Risk of Untreated CVT is 4.8 fold for DVT to recur. Early treatment of CVT LET class I is mandatory because it prevents extension of CVT into proximal DVT and will reduce DVT recurrence and PTS by 50%. Guarnera et al. reported a study of 111 patients with CVT LET class I in the gastrocnemius or tibial deins diagnosed by CUS, circumference of calf ’s and ankles and treated with nadroparin and MECS [56]. The calf circumference in the affected leg significantly decreased from 38.1 cm to 37.1 cm after one week and to 35.7 cm after one month. This was associated by significant decrease of VAS-pain score from 58 to 30 after one week and to 12.7 after one month.
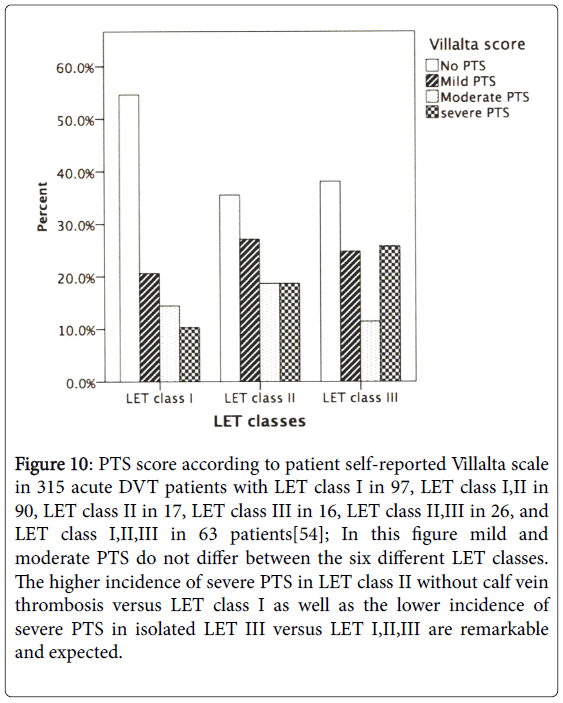
Figure 10: PTS score according to patient self-reported Villalta scale in 315 acute DVT patients with LET class I in 97, LET class I,II in 90, LET class II in 17, LET class III in 16, LET class II,III in 26, and LET class I,II,III in 63 patients[54]; In this figure mild and moderate PTS do not differ between the six different LET classes. The higher incidence of severe PTS in LET class II without calf vein thrombosis versus LET class I as well as the lower incidence of severe PTS in isolated LET III versus LET I,II,III are remarkable and expected.

Figure 11: Mean VEINES-QOL scores according to patient selfreported questionaires in 315 acute DVT patients with LET class I in 97, LET class I,II in 107, and LET class in 105 patients after a mean follow-up 6 years[55].
D-Dimer strategy to prevent DVT recurrence by extended anticoagulation
The 2006 PROLONG randomized multicenter management study used the qualitative SIMPLIFY D-Dimer assay, which was normal in 385 (63.3%) and abnormal in 223 (36.7%) of 608 post-DVT patients (36.7%) one month after anticoagulation discontinuation [57]. After 1.5 years follow-up a total of 18 events occurred among the 120 patients who stopped anticoagulation (15.0%), as compared with 3 events among the 103 patients who resumed anticoagulation (2.9%) (hazard ratio 5.36; P=0.007, Figure 12). After 1.5 years follow-up the incidence of VTE recurrence increased to 24 of 385 patients with a normal Simplify D-dimer level (6.2%) with a hazard ratio of 2.17; P=0.21, Figure 8) as compared to those with an abnormal Simplify Ddimer level while on anticoagulant treatment (Figure 8). After 4 years of follow-up the incidence of VTE recurrence increased to about 35% (NPV 65%) with hazard ratio (HR) of 6.0 for abnormal Simplify DD/no-VKA vs. continuation of VKA (Figure 12). After 4 years of follow-up the hazard ratio (HR) between normal Simplify DD with no VKA versus abnormal DD treated with VKA increased to 2.97 with an absolute incidence of DVT recurrence of about 20% (NPV 80%) (Figure 13) [58]. These results after 4 years follow-up in Figure 10 clearly indicate that separation of unprovoked DVT in two groups by a qualitative Simplify D-dimer test is not sensitive enough to separate a clear cut low risk group of DVT recurrence after anticoagulant discontinuation. These data strongly indicate the need to use a sensitive ELISA VIDAS D-dimer test in combination with PTS assessment the C of CEAP and/or Villata score to better separate low versus intermediate versus high risk VTE recurrence rate at time of anticoagulation discontinuation.

Figure 12: The qualitative Simplify D-Dimer assay used in the PROLONG multicenter management was normal in 385 (63.3%) and abnormal in 223 (36.7%) of 608 patients (36.7%). During a maximal follow-up of 600 days (1.6 years) a total of 18 events occurred among the 120 patients who stopped anticoagulation (15.0%), as compared with 3 events among the 103 patients who resumed anticoagulation (2.9%), for an adjusted hazard ratio of 4.26 (95% confidence interval [CI], 1.23 to 14.6; P=0.02)[57]. Thromboembolism recurred in 24 of 385 patients with a normal Ddimer level (6.2%). Among patients who stopped anticoagulation, the adjusted hazard ratio for recurrent thromboembolism among those with an abnormal D-dimer level, as compared with those with a normal D-dimer level, was 2.27 (95% CI, 1.15 to 4.46; P=0.02).
The DULCIS study (D-dimer and Ultrasound in Combination Italian Study) used as compared to the sensitive ELISA VIDAS Ddimer assay less sensitive quantitative D-dimer assays for the evaluation of VTE recurrence after anticoagulation discontinuation in 988 evaluable DVT patients with a first unprovoked DVT [58]. If after the period of at least 6 months post-DVT the quantitative D-dimer used (VIDAS, Innovance, Hemosil HS, Hemosil or STA Lia test) in this multicenter study remained below the cut-of point of normal, anticoagulation was definitely stopped and the patients were followedup for 2 years. In the cohort of 109 post-DVT patients who refused OAT treatment, and who had a quantitative D-dimer measurement above the cut-off value, the incidence of major VTE was 8.8% (2.3% patient/years). In 506 (51%) of the 988 post-DVT patients, the Ddimer levels were normal after stopping anticoagulation, the incidence of VTE was 2.8%, patient/years. Out of 988, 373 (38%) patients with increased quantitative D-dimer levels received extended anticoagulation for 2 years follow-up the incidence of VTE was 0.7% patient/years at the cost of 14 major bleedings (2.3% patients/years) [58]. These 2 years follow-up results in the DULCIS study indicate that separation of unprovoked DVT in two groups by a normal versus increased quantitative D-dimer tests result is appears to be feasible and sensitive when combined with HER or C of CEAP PTS evaluation to separate a low versus high risk group of DVT recurrence after anticoagulant discontinuation.
Prediction rules for DVT recurrence
As the expansion of the Palareti’s D-dimer strategy in the PROLONG and DULCIS studies after discontinuation of anticoagulant treatment three groups of VTE investigators developed simple scoring systems to asses VTE=DVT and pulmonary (PE) recurrence risk restricted to patients with a first un-provked DVT (Table 7). Eichinger et al. [59] developed the Vienna Prediction Model. Tosetto et al. [60] constructed the DASH score. Rodger et al. [36] designed the HERDOO2 study and treatment anticoagulant outcome (Figure 5). The HERDOO2 scoring system is suitable for women but not for men (Table 7). The three prediction models in unprovoked DVT patients have been developed to assess the risk of VTE by linking clinical characteristics with laboratory test and the use of D-dimer of different accuracy and cut-off levels (ELISA VIDAS in the HERDOO2 and ELISA D-dimer in the Vienna Prediction Models and unspecified in the DASH prediction model (Table 7). All three VTE prediction models are suboptimal similar as has been clearly demonstrated by Palareti in his PROLONG and DULCIS studies (Figures 6 and 7). Post- DVT patient with a first DVT recurrence after discontinuation of anticoagulation are candidate for long-term or even lifelong anticoagulant in particular when associated with a persistent risk factor or PTS.
Bridging the gaps between acute DVT treatment, DVT recurrence and PTS prevention
The proposed concept to bridge the gap between DVT and PTS in Figures 7 to 11, addresses six key questions to be solved by novel treatment options of provoked and unprovoked acute DVT to prevent DVT recurrence and to reduce the incidence of PTS [45-56]. The diagnostic work-up of post-DVT patients should follow the Rotterdam, Antwerp Maastricht approach to PTS according to current recommendations [1,15,50,61-64]. To validate the proposed concept a prospective safety-outcome study is mandatory with a minimal followup period of 2 years (Figure 13) [1,62-64]. All acute CVT and DVT patients will immediately receive anticoagulant and compression therapy (MECS). Serial CCUS at 1 and 3 months post-DVT will separate the group of patients with rapid and complete recanalization versus the group with delayed and incomplete recanalization. Objective documentation will consist of PTS score using the patient self-reported Villalta scale according to Wik et al. [33], the C of CEAP scoring assessment (Table 5) and serial CUS at 1 and 3 months post- DVT followed by taking a therapeutic decision at 6 to 12 month spost- DVT for extended anticoagulation (Figure 14). The strategy in study arm 1 is predicted to be cost-effective and safe. Patients with delayed recanalization and reflux but no significant PTS (C 0/1) at 3 to 6 months post-DVT have no indication for wearing MECS but are candidates for extended anticoagulation for at least one year post- DVT. Symptomatic patients with PTS (Villalta score and C of CEAP) at time point 6 months post-DVT are candidates for wearing MECS just for symptomic relief of PTS complaints at work and during walking at daytime. Patients with PTS (Villalta and C of CEAP) on top of abnormal flow US at 6 to 12 months post-DVT should be considered for extended or even life-long anticoagulation with apixaban 2.5 mg bid ombined with MECS (Figure 14). As demonstrated in the PROLONG and DULCIS studies [57,58], proper extension of anticoagulation with low dose apixaban 2.5 mg bid is currently one of the best option to prevent the DVT recurrence after discontinuation of anticoagulant treatment (Figure 14). The presence of hyperpigmentation (C4), edema (C3) and redness (HER) [36] of the skin in post-DVT patients as assessed by the objective C of CEAP criteria on of ultrasonic abnormalities at time points 3, 6 to 12 months post-DVT surely will become the strongest predictors of DVT recurrence and embolic complications. In view of the distribution of DVT in the proposed study design in Figures 5-10, the LET extension classification at time of a first acute DVT of the lower leg will have significant therapeutic implications. Symptomatic patients with acute ileofemoral and rapid extension of proximal DVT into the ileofemoral region are candidate for catheter directed thrombolysis as the risk of severe post-thrombotic syndrome by anticoagulation alone is high and irreversible. Recanalization of distal DVT in the calf and lower popliteal region is predicted to be rapid and complete with no reflux on ultrasonography and subsequent low risk of DVT recurrence and PTS obviating the need of wearing MECS and anticoagulation at 6 months post-DVT. Delayed and incomplete recanalization of proximal DVT and the presence of reflux due to valve destruction irrespective of the degree of recanalization on CUS at 3 to 6 months post-DVT will occur in one third of LET I/II and LET II class DVT and is associated with a high risk of DVT recurrence and symptomatic PTS indicating the need to wear MECS for relief of symptoms and to extend anticoagulation to prevent DVT recurrence as the main cause of PTS. If residual venous pathology (RVP) on CUS at 3 or 6 months post- DVT is present further invasive corrective strategy will mainly depend on the absence or presence of PTS related to reflux in the popliteal/ femoral region or partial obstruction outlet syndrome in the iliofemoral region (May-Turner syndrome). If this involves the femoral and/or popliteal veins, continuation of MECS is advocated. If symptoms of venous claudication and duplex raise suspicion of residual obstruction or at the ileofemoral level (absence of phasic flow at the level of the common femoral vein, visible obstruction of the external iliac vein or prominent collateral circulation) consultation of experts is mandatory to assess the clear indication for surgical correction or stenting. Moossdorff and Michiels performed in 2016 the DVT-PTS Bridging the Gap pilot study in the primary care setting to test the feasibility of the LET approach in the primary care setting and produced good evidence that complete recanalization of proximal DVT will occur in about one third of DVT in the popliteal/femoral region (LET class II) on serial CUS within 3 months post-DVT[65-67]. This is predicted to be associated with no or low risk on DVT recurrence with no reflux on DUS and no or very low risk on PTS obviating the need of wearing stockings and no need for extended anticoagulation. When the recanalization of the popliteal-femoral region is delayed and incomplete at 3 months post-DVT (RVT present) due to reflux and valve destruction in the polpiteal/femoral region, this will be associated with a high risk of DVT recurrence as the cause of PTS[65-67]. Post-DVT patients with a high risk for DVT recurrence are candidates for long-term extension of anticoagulation with DOACs (apixaban 2.5 mg bid) (Figure 13).

Figure 13: After 4 years (1500 days) follow-up of the PROLONG study, the hazard ratio (HR) between abnormal Simplify D-dimer and No VKA vs. VKA increased from5.3 to 6.1 with an absolute incidence of DVT recurrence of about 35%. After 4 years of followup the hazard ratio (HR) between Normal Simplify D-dimer and no VKA versus Abnormal Simplify D-dimer and VKA increased from 2.1 to 2.97 with absolute incidence of DVT recurrence of about 20% indicating that the qualitative Simplify D-Dimer test is not sensitive enough to separate low risk versus moderate to high risk DVT recurrence in patients with unprovoked DVT after discontinuation of anticoagulant treatment. Courtesy of Palareti 2007.

Figure 14: Algorithm of the Rotterdam Maastricht treatment options of acute deep vein thrombosis (Acute DVT), the duration of regular anticoagulation and discontinuation or expension of anticoagulation according to the D-dimer strategy of the PROLONG and DULCIS study[57,58]. For extended anticoagulant treatment in post-DVT-patients low dose Direct Oral Anticoagulants (DOACs) with apixaban 2.5 mg BID is srongly recommended, whereas rivaroxaban 20 mg QD is not safe enough foe prevention of VTE recurrence in terms of bleeding complications. Rivaroxaban should be evaluated in prospective quality driven academic management studies in primary care health medicine and hospital outpatients ward comparing 20 mg QD versus 10 mg BID during treatment prolongation and 10 mg versus 2x 5 mg BID in extension studies for prevention of DVT and PE recurrence and the post-thrombotic syndrome [1,63,64].
The results from the AdVent study (Table 12) [68,69], suggested that isolated acute ileofemoral DVT and extension of proximal popliteal/ femoral in LET class III DVT patients at time of acute DVT presentation (Figure 13) may profit from Catheter Directed Thrombolysis (CDT) as compared to regular anticoagulation. However the differences in PTS using the Villata score of >5 in the AdVent study were minor after 1 year follow-up and severe PTS was even higher in the CDA treated as compared to anticoagulation after 5 years follow-up (Table 12) [68,69]. The results of the ATTRACT randomized clinical trial comparing catheter directed thrombolysis followed by anticoagulation versus anticoagulation alone (control) included patients with idiopathic acute popliteal/femoral and iliofemoral DVT (Table 12) [70]. The results of the ATTRACT study were neither inferior nor superior for eacht of the two treatment options CDT vs. anticoagulation (Table 12) [70]. The ongoing randomized clinical study comparing Catheter Accelerated thrombolysis Versus Anticoagulation (CAVA) only included acute ileofemoral DVT LET class III with a short clinical history of less than one week or 10 days because the risk of severe PTS by anticoagulation alone in LET Class III/IV acute DVT patients is irreversible and high [49-56]. The CAVA study excluded proximal popliteal/femoral (LET class II). Fresh early stage of acute proximal DVT LET class II/III without involvement of calf or popliteal vein should are to be considered as ‘ideal’ candidates for CDT in the near future. The results of the CAVA study results are to be expected in the fall of 2018.
The first author is a founder of the Good heart Institute & Foundation in Nature Medicine & Health, Rotterdam, The Netherlands, Freedom of Science and Education, European Free University Network. JJ Michiels is co-founder of the Central European Vascular Forum (CEVF) and serves as consultant professor in the Blood coagulation, Hemostasis Research Laboratory (co-founder VWF-VWD research program) at the department of Hematology University Hospital, Antwerp; as consultant professor in Hematology and Blood coagulation, Comenius University, Bratislava, Slovakia; as consultant professor in hematology, Romania MPN Working Group, University Hospital Bucharest; consultant to the Dutch Society of Internal Medicine and Ministry of Public Health; consultant of quality driven Industrial and Pharmaceutical Medicine; as an editor of 3 Medical Journals and as a guest editor on request and by self-initiation. Writing assistance was utilized in the preparation of this manuscript, it was carried out at the Good heart Institute and Foundation in Nature Medicine and Health, Rotterdam, The Netherlands. The author has no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.