Biochemistry & Pharmacology: Open Access
Open Access
ISSN: 2167-0501
![]() +44-77-2385-9429
+44-77-2385-9429
ISSN: 2167-0501
![]() +44-77-2385-9429
+44-77-2385-9429
Research Article - (2015) Volume 4, Issue 1
Despite its decreasing incidence in western countries, the care of gastric cancer remains a concern. As gastric cancer is often diagnosed at an advanced stage, the prognosis of patients with advanced disease remains dismal. Recent trials in advanced gastric cancer have been focused on targeted therapies. Agents targeting EGFR1 and HER2 have been widely tested. The addition of trastuzumab to cisplatin/fluoropyrimidine-based combination chemotherapy significantly improved survival in patients with HER2 positive advanced gastric cancer, which is now the new standard of care by recent ToGA trial. Other agents targeting VEGF, the PI3K–Akt–mTOR pathway, and other biological pathways have also been investigated in clinical trials, but showed little impact on the survival of patients. This review will focus on the recent progress in targeted agents for the treatment of AGC and summarize the current clinical evidence and ongoing trials supporting the use of targeted agents in the treatment of patients with AGC.
<Keywords: Targeted therapy; Advanced gastric cancer; Novel; HER2; VEGF
Gastric cancer (GC) is the fifth most common cancer in the world and is the third-leading cause of cancer death. There were nearly one million new cases worldwide in 2012 (631,000 men, 320,000 women) with approximately 723,000 deaths (469,000 men, 254,000 women) [1]. Over 70% of new cases and deaths occurred in developing countries, with the highest incidence in Eastern Asia, especially in Japan and China [2]. According to the 2012 Chinese cancer registry annual report, gastric cancer had become the third most common cancer and the second leading cause of cancer related death in China [3].
The survival of patients with gastric cancer is substantially worse than that of patients with most other solid malignancies, and the only treatment that offers a potential cure is complete resection of the tumor. However, in most of countries, the majority of patients is diagnosed at advanced stages and has a poor prognosis. Despite the improvement of surgical techniques and the recent availability of new chemotherapy regimens, outcome of the patients with advanced disease is usually poor, the median overall survival (OS) is approximately 7 to 11 months, and the median progression-free survival (PFS) is 6 to 7 months [4-6]. These results suggested that even the most widely accepted regimens, such as fluoropyrimidine and/or platinum based chemotherapy regimens, have not been able to achieve satisfactory survival. Thus, there is an urgent need to develop more efficient therapies.
During the past few decades, remarkable progress in tumor biology has led to the development of new agents that target critical aspects of oncogenic pathways. Recent trials in advanced gastric cancer have been focused on targeted therapies, the agents including: targeting the membrane HER2 and EGFR membrane receptors, as well as antiangiogenic drugs targeting VEGF. A number of small trials have also appeared in the literature, exploring the inhibition of the Akt– mTOR pathway (Figure 1). However, only HER2-targeting drugs have been proven efficacy so far. This review will focus on the recent progress in targeted agents for the treatment of AGC and summarize the current clinical evidence and ongoing trials supporting the use of targeted agents in the treatment of patients with AGC.
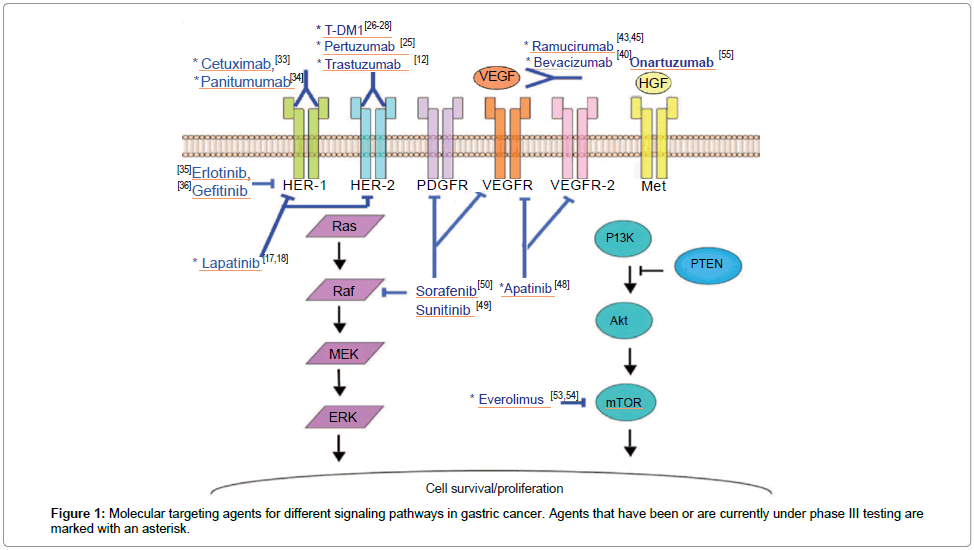
Figure 1: Molecular targeting agents for different signaling pathways in gastric cancer. Agents that have been or are currently under phase III testing are marked with an asterisk.
Among HER family members, such as human epidermal growth factor receptor (EGFR, also referred to as HER1), HER2, HER3 and HER4, HER2 has become the focus of investigations in GC. HER2 overexpression is observed in 10%–38% of gastric cancer tumor samples, and it is more frequent in intestinal type compared with that in diffuse type GC and in cancers of the gastroesophageal junction (GEJC) compared with that in cancers located elsewhere in the stomach [7-9].
Trastuzumab
Trastuzumab is a humanized recombinant monoclonal antibody that selectively binds to the extracellular domain of HER-2, thereby blocking its downstream signaling. Up to now, trastuzumab is the first and only targeted agent for gastric cancer approved by both the U.S [10] and European [11] authorities.
Trastuzumab has been evaluated in ToGA study. A major breakthrough was achieved in the care of advanced gastric cancer since the results of the ToGA trial were published [12]. This was a large multicenter, randomized, controlled phase III clinical study, exploring the benefit of trastuzumab in addition to chemotherapy, in HER2 overexpression advanced cancer of the stomach or gastroesophageal junction. In this trial, a total of 3665 patients were screened for HER2 overexpression, leading to the randomization of 298 and 296 HER2- positive (IHC 3+ or FISH-positive) patients in the chemotherapy (capecitabine or 5-fluorouracil plus cisplatin) plus trastuzumab or chemotherapy alone arms, respectively. Importantly, cross-over to the trastuzumab-containing arm was not allowed for patients progressing in the reference arm. The addition of trastuzumab to chemotherapy led to a significantly longer OS duration, 13.8 months versus 11.1 months (p =0.0046), significantly longer PFS interval, 6.7 months versus 5.5 months (p<0.0002), and significantly higher overall response rate (ORR), 47% versus 35% (p<0017). The greatest benefit was seen in patients with higher levels of HER-2 expression, with either an IHC score of 3 or 2 plus FISH positivity; the OS time of those patients reached 16 months. Adverse effects were comparable between the two treatment groups. Moreover, the addition of trastuzumab did not affect quality of life. Based on the findings of this trial, trastuzumab, in combination with cisplatin–fluoropyrimidine chemotherapy has been approved by US FDA and European Medicines Agency as first-line therapy in HER2 positive GC and GEJC.
However, the OS gain was shorter than expected by comparison with breast cancer studies, and the GC patients who achieved an initial therapeutic response to trastuzumab eventually exhibited disease progression within 7 months. Those findings suggested that a significant proportion of patients with HER2-positive GC either do not satisfactorily respond to trastuzumab or develop an acquired resistance to this antibody.
Lapatinib
Lapatinib is a dual inhibitor of the tyrosine kinase domains of HER- 1 and HER-2 based on its interference with adenosine triphosphate binding. Lapatinib has been proven efficacy and approved in HER2- positive breast cancer [13]. With regard to GC, several preclinical studies demonstrated the anti-proliferative effects of lapatinib [14], in addition to the synergic action of lapatinib with trastuzumab [15] or with other chemotherapeutic agents, such as 5-fluorouracil, cisplatin, oxaliplatin and paclitaxel, and irinotecan [14]. However, a phase II study of lapatinib in combination with chemotherapy as first-line treatment achieved only a 9% response rate, with a median OS of 4.8 months [16]. Subsequently, the TYTAN trials, investigated weekly paclitaxel plus or minus lapatinib in second-line therapy in HER2 positive GC. It failed to demonstrate any OS and PFS benefit in the ITT population, but statistically significant improvements in OS and PFS were observed in patients with HER2-positive IHC3 + tumors and in Chinese patients [17]. The LOGiC phase III trial investigated capecitabine and oxaliplatin plus or minus lapatinib in first-line therapy in advanced or metastatic HER2 + upper GI tract (UGIT) adenocarcinomas, the results were reported in 2013 ASCO meeting and demonstrated a non-significant prolongation (1.7 months) of OS with the addition of lapatinib [18].
The limited efficacy of trastuzumab in the ToGA trial [12] and the unsatisfactory results of the TYTAN [17] and LOGiC trials [18] mentioned above suggest that the presence of drug resistance mechanisms or alternative pathways of escape from HER2 targeted therapy. To improve the treatment results of targeting HER2 in HER2-positive GC patients, there is an urgent need to elucidate the mechanisms underlying the alterations in tumor cell sensitivity to anti-HER2 therapy and to establish rational strategies to overcome this phenomenon.
Pertuzumab
Pertuzumab is a recombinant, humanized immunoglobulin IgG 1k monoclonal antibody, which targets HER2, a transmembrane glycoprotiein with intrinsic tyrosine kinase activity. It is the first one in a new class of targeted cancer treatment called HER2 dimerization inhibitors. Pertuzumab prevents HER2 from dimerizing with other ligand-activated HER receptors, most notably HER3 [19,20]. Like trastuzumab, pertuzumab can also stimulate antibody-dependent, cell-mediated cytotoxicity (ADCC). Because pertuzumab and trastuzumab bind to different HER2 epitopes and have complementary mechanisms of action, these two agents, when given together, provide a more comprehensive blockade of HER2 signaling and result in greater antitumor activity than either agent alone in HER2-positive tumor models [21,22]. Its efficacy and safety in combination with trastuzumab in HER2-positive metastatic breast cancer patients has been demonstrated in some phase III clinical trials [23,24].
In gastric cancer, an ongoing randomized phase IIa study (Study BP27836, JOSHUA) is being conducted in patients with inoperable or metastatic HER2 positive adenocarcinoma of GC or GEJC. This study has shown activity and safety of pertuzumab combined with cisplatin and capecitabine in patients with HER2-positive metastatic gastric cancer. Now a double-blind, placebo- controlled, randomized phase III study ( Study BO25114, JACOB) is being conducted to compare overall survival (OS) in patients with HER2-positive AGC or GEJC treated with pertuzumab in addition to trastuzumab plus fluoropyrimidine and cisplatin (TFP) versus patients treated with placebo in addition to TFP. The primary objective is OS, the secondary objectives include PFS, ORR, quality of life and safety. The result of this study is worth expecting [25].
T-DM1
Trastuzumab-DM1 (T-DM1) is a novel anti-HER2 antibody-drug conjugate (ADC) in development for treatment of patients with HER2- positive cancer. T-DM1 combines the HER2-targeting properties of trastuzumab with intracellular delivery of DM1, a highly potent derivative of the antimicrotubule agent maytansine [26-28]. DM1 binds to tubulin and inhibits microtubule assembly with greater potency than vincristine or vinblastine. In T-DM1, trastuzumab and DM1 are covalently linked via the thioether linker (N-maleimidomethyl) cyclohexane-1-carboxylate (MCC).
T-DM1 has now demonstrated significant therapeutic effects in some phase III trials and may set a new standard for anticancer therapy as a drug with minimal toxicity and significant efficacy in previously treated HER2 overexpressing breast cancer patients. A trial (NCT01641939) is now ongoing to examine the efficacy and safety of T-DM1 compared with standard taxane therapy in patients with HER2- positive gastric cancer in second line setting. In this study, patients will be randomized to one of the three groups, 3.6 mg/kg T-DM1 every 3 weeks, 2.4 mg/kg T-DM1 every week, or standard taxane therapy for at least 12 weeks. The primary endpoint of the study was OS. If this study can achieve a positive result, it will provide a more effective strategy to improve the survival of patients on the current basis of trastuzumab treatment.
The EGFR is overexpressed in about 25% of gastric cancer and has been associated with more aggressive phenotype and poorer survival, which suggests that EGFR may be a rational therapeutic target [29]. Interestingly, and in contrast to colorectal cancer findings, where KRAS mutations occur in approximately 40% of patients and predict for lack of anti-EGFR efficacy, KRAS mutations are less common in gastric cancer, as these are only found in 3–13% of cases [30-32]. Similarly, no correlation was found between the KRAS genotype and response to treatment in gastric cancer, although further data may be needed to ascertain these findings [32]. Anti-EGFR mAbs and TKIs are currently undergoing clinical trials for GC patients.
Cetuximab
Cetuximab is a chimeric (mouse/human) mAb targeting to EGFR. Cetuximab is already approved for use in metastatic colorectal cancer and head and neck cancer. In several phase II trials of gastric cancer, cetuximab has shown some promising results when combined with various chemotherapeutic agents in first-line settings. The phase III trial (EXPAND) [33] assessed the efficacy of cetuximab in combination with cisplatin and capecitabine as a first-line treatment for patients with advanced GC or GEJC. 904 patients in 24 countries were randomized to receive capecitabine and cisplatin, or the same combination plus cetuximab. The primary study end point is PFS, and secondary objectives include OS, quality of life and safety. The results are disappointing. This study has failed to meet its primary end point, the addition of cetuximab did not extend PFS, compared with chemotherapy alone (4.4 months in cetuximab plus chemotherapy group vs. 5.6 months in chemotherapy alone group, p=0.3158).
Panitumumab
Panitumumab is a fully humanized IgG2 mAb targeting EGFR, and which has been approved in metastatic, wild-type KRAS genotype colorectal cancer patients, in combination with chemotherapy. In gastric cancer, a phase II–III trial (the REAL-3 trial) was designed to assess the combination of panitumumab with the standard epirubicin, oxaliplatin and cisplatin (EOC). However, the survival in the panitumumab arm was inferior to that in the chemotherapy-alone arm (PFS, 6.0 months vs. 7.4 months, p = 0.068; OS, 8.8 months vs. 11.3 months, p = 0.013) [34].
The EGFR tyrosine kinase inhibitors (TKIs) gefitinib and erlotinib were evaluated in phase II trials but produced disappointing results as monotherapy for AGC [35,36]. Accordingly, there is no plan to move forward with anti-EGFR mAbs in further clinical investigation of AGC.
The clinical results of anti-EGFR agents might suggest that the role of EGFR pathway and the value of anti-EGFR therapy in GC need more evaluation and the concrete strategy including appropriate target patients population, combination and sequence with chemotherapy agents also need further investigation.
Bevacizumab
VEGF is a key factor to the development of tumor angiogenesis and its blockade has been extensively studied in a variety of solid tumors. Hence bevacizumab, an anti-VEGF monoclonal antibody, has been approved in colororectal, kidney, lung and breast cancer. Several phase II trials combining bevacizumab with different chemotherapeutic agents were conducted on treatment-naive or pretreated patients with AGC or GEJC, demonstrating results which were initially promising [37-39]. A Phase II trial of bevacizumab 15 mg/kg at day 1 plus cisplatin 30 mg/m2 and irinotecan 65 mg/m2, both at day 1 and day 8, every 3 weeks, was administered in 47 advanced gastric or gastroeosophageal junction cancer patients, showing a promising 65% overall response rate and a median time to progression of 8.3 months. The tolerance was well [37]. In another report, bevacizumab 7.5 mg/kg was combined with docetaxel 70 mg/m2 and oxaliplatin 75 mg/m2 every 2 weeks, showing a 42% response rate in 38 advanced gastric cancer patients, with a median PFS of 6.6 months [38]. On the basis of results from these phase II studies, a large prospective phase III randomized, doubleblind, contrast study (AVAGAST) was conducted internationally [40]. In this study, 774 advanced gastric or gastroeosophageal junction cancer patients were randomized to receive cisplatin and capecitabine with or without bevacizumab. Although the study did not reach its primary endpoint of OS (12.1 vs 10.1 months; p = 0.1002), the ORR was significantly better in the bevacizumab arm (46% versus 37%; p =.0315) and the PFS interval was significantly longer (6.7 vs. 5.3 months; HR: 0.8; p = 0.003). Interestingly, there was a discrepancy between OS HRs according to the geographical regions. Survival was longer in patients in pan-America with the addition of bevacizumab, but not in Asians or Europeans despite the better prognosis of the latter. That might be related to a higher rate of further treatment as 66, 31 and 21% of patients received a second-line therapy in Asia, Europe and pan-America, respectively. Suffice it to say, it seems inappropriate to incorporate bevacizumab in the treatment algorithm of AGC patients now.
Ramucirumab
Vascular endothelial growth-factor receptor (VEGFR)-2 and the VEGF A, C, and D ligands are known mediators of angiogenesis. VEGFR-2 is an important mediator in the VEGF pathway [41,42].
Ramucirumab is a fully human monoclonal antibody (IgG1) that binds the extracellular domain of VEGFR-2 and blocks VEGF ligands binding, shutting down VEGF signaling and inhibiting the growth of new blood vessels that feed the tumor. Ramucirumab is being tested in several phase III clinical trials for the treatment of metastatic gastric adenocarcinoma [43], non-small cell lung cancer [44] , among other types of cancer.
REGARD [43] is a global, randomized, double-blinded, placebocontrolled phase III study of ramucirumab and best supportive care (BSC) compared to placebo and BSC as treatment in patients with locally advanced or metastatic gastric cancer including gastroesophageal junction adenocarcinoma following progression after initial fluoropyrimidine or platinum-containing chemotherapy. In total, 355 patients were randomized in 29 countries. The primary endpoint was overall survival and the secondary endpoint was progression-free survival. Results demonstrated that ramucirumab (8 mg/kg by infusion every two weeks) plus best supportive care (BSC), as compared to placebo plus BSC, increased the median overall survival of patients with advanced gastric cancer by 37 percent (median overall survival of 5.2 months [95% CI 4.4, 5.7] vs. 3.8 months [95% CI 2.8, 4.7] for placebo, P=0.047, hazard ratio 0.78 [95% CI 0.60, 0.998]). Additionally, ramucirumab significantly improved progression-free survival, demonstrating a 62 percent increase in median progressionfree survival (2.1 months [95% CI 1.5, 2.7] vs. 1.3 months [95% CI 1.3, 1.4] for placebo, P < 0.001, hazard ratio 0.48 [95% CI 0.38, 0.62]).
It is the first phase III trial to show improved overall survival and progression-free survival with a biologic agent in advanced gastric cancer after prior chemotherapy. Based on results of REGARD, on April 21, 2014, the U.S. Food and Drug Administration (FDA) has approved ramucirumab as a single-agent treatment for patients with advanced or metastatic gastric cancer or gastroesophageal junction (GEJ) adenocarcinoma with disease progression on or after prior fluoropyrimidine- or platinum-containing chemotherapy. This approval represents a meaningful advance for patients and gives them an important new second-line treatment option.
Similar to REGARD study, in RAINBOW study, ramucirumab adds to an efficacy of chemotherapy also improved overall survival in second-line gastric cancer.
RAINBOW [45] study is a global, phase III, randomized, doubleblind study of ramucirumab plus paclitaxel versus placebo plus paclitaxel in the treatment of metastatic gastric adenocarcinoma following disease progression on first-line platinum- and fluoropyrimidine-containing combination therapy. Patients with gastric or gastroesophageal junction cancer who experienced disease progression during or within 4 months of first-line therapy with a platinum agent and a fluoropyrimidine were randomly assigned to 1 of 2 treatment regimens. All 665 patients received paclitaxel 80 mg/m2 on days 1, 8, and 15 of every 4-week cycle until disease progression, unacceptable toxicities, or death. They were also randomly assigned to receive intravenous ramucirumab 8 mg/kg every 2 weeks or placebo. The ramucirumab and paclitaxel combination was associated with better OS (9.6 vs. 7.4 months, HR, 0.87, 95% CI, 0.678 - 0.962; P = .0169) and PFS (4.4 vs. 2.8 months; HR, 0.635; 95% CI, 0.536 - 0.752; P <.0001) than monotherapy. Patients treated with the combination also had a significantly better median TTP (5.5 vs. 3.0 months; P <.0001) and a better objective response rate (28% vs. 16%; P =.0001). This largest gastric cancer second-line trial clearly demonstrated that an effective second-line therapy can improve survival of patients with metastatic advanced gastric cancer. This is the only study to date to demonstrate a 2-month improvement in survival in this setting, and with a relatively high 28% response rate for the combination therapy.
The results of the RAINBOW trial, combined with findings from REGARD trial of ramucirumab monotherapy, support the routine use of second-line therapy in patients with advanced gastric cancers who can tolerate the regimens. It also seemed that the targeting VEGFR agents might be more rational in the second-line therapy of AGC rather than in the first-line therapy.
Apatinib
Apatinib (YN968D1) is a small-molecular TKI agent that highly and selectively inhibits the VEGFR-2 [46]. In a randomized, threearm, double-blind, phase II trial of apatinib as a third-line treatment in patients with metastatic gastric cancer, 141 patients were randomized to receive apatinib (850 mg, qd), apatinib (425 mg bid) or placebo [47]. The study was reported during the 2011 ASCO Annual Meeting, and the results were as follows: median PFS, 3.4 months vs. 3.4 months vs. 1.4 months; median OS, 4.8 months vs. 4.3 months vs. 2.5 months. Common AEs included hypertension and hand-foot syndrome. Based on this result, a randomized, double blinded, placebo controlled, multicenter phase III study in a third-line setting in AGC is currently being conducted in China, the preliminary results were reported during the 2014 ASCO Annual Meeting [48]. Totally 273 patients were randomized to apatinib 850 mg qd p.o. or placebo and were treated until disease progression, intolerable toxicity or withdrawal of consent. The primary endpoint is OS. Median OS was 6.5 months with apatinib vs. 4.7 months with placebo (HR, 0.709; 95% CI, 0.537- 0.937; P = .0149). Median PFS was 2.6 vs. 1.8months (HR, 0.444; 95% CI, 0.331-0.78; p < .0001). The AE including hypertension, proteinuria, hand-foot syndrome, bleeding, cardiac and liver toxicities, but all were manageable and reversible. Apatinib is the first small molecule targeting VEGFR to show a survival benefit in AGC, which made it as a new treatment option for AGC patients who failed to second line of chemotherapy.
Sunitinib & Sorafenib
Sunitinib is an orally available tyrosine kinase inhibitor that is approved in kidney cancer and gastrointestinal stromal tumors, which targets VEGFR1–3, PDGFR, RET and KIT. In gastric cancer, sunitinib was investigated in patients as second line treatment in a Phase II study that enrolled 78 patients with advanced gastric cancer. At a dose of 50 mg/day for 4 weeks every 6 weeks, disease control was obtained in 34.7% of patients (partial response: 2.6%; stable disease: 32.1%). The median PFS was 2.3 months and median OS was 6.8 months respectively. Adverse events were unremarkable at 50mg dosing (fatigue, neutropenia, nausea, diarrhea and stomatitis) [49]. These data suggested that single-agent sunitinib has little clinical interest as salvage therapy for chemotherapy-refractory AGC patients. At this time, there is no plan to move forward with sunitinib in further clinical investigations of GC.
Other tyrosine kinase inhibitors, such as the multikinase inhibitor sorafenib, similar to sunitinib in activity, are studied in Phase I and Phase II trials for gastric cancer. A phase II study of sorafenib combined with docetaxel and cisplatin as a treatment for chemo-naive metastatic or local advanced unresectable GC or GEJC patients was recently reported [50]. The study enrolled 44 patients who received sorafenib 400 mg bid, in combination with docetaxel 75 mg/m2 day 1 and cisplatin 75 mg/m2 on day 1 in a 3 weeks cycle. The ORR was 41 %, the median PFS was 5.8 months, and the median OS was 13.6 months. The authors concluded that sorafenib, combined with docetaxel and cisplatin, was effective and tolerable as a treatment for GC or GEJC. However, the results of this study did not show superiority over historical data from the cisplatin and docetaxel combination chemotherapy, thereby unlikely to be further clinical development of sorafenib in GC.
Everolimus
mTOR is a key regulator of cell growth and proliferation, cellular metabolism, and angiogenesis, belonging to the PI3K–Akt–mTOR signaling pathway. The mTOR pathway has been shown to be frequently activated in a variety of human cancers, including gastric cancer [51]. Inhibitors of the PI3K–Akt–mTOR pathway have been developed at multiple levels, such as PI3K–Akt inhibitors and mTOR inhibitors. Among these drugs, everolimus (RAD001) has been investigated in advanced gastric cancer, as preclinical data suggested that the drug reduced peritoneal dissemination of a gastric cancer cell line in a mouse model [52]. In a multicenter phase II trial using everolimus as salvage therapy for pretreated AGC patients, the disease control rate was 55%, and the median PFS were 2.7 months. At a median followup duration of 9.6 months, the median OS was 10.1 months and good tolerability was observed [53]. Based on this provocative result, a phase III randomized trial, GRANITE-1 study was conducted to compare everolimus with placebo plus best supportive care in patients with progressive disease after one or two prior lines of chemotherapy [54]. A total of 656 patients from 23 countries were enrolled; 439 were randomized to everolimus, 217 to placebo. Median OS was 5.39 months with everolimus vs. 4.34 months with placebo (HR, 0.90; 95% CI, 0.75- 1.08; P = 0.1244). Median PFS was 1.68 vs. 1.41 months (HR, 0.66; 95% CI, 0.56-0.78; p < 0.0001). Compared with BSC, everolimus did not significantly improve overall survival for advanced gastric cancer that progressed after one or two lines of previous systemic chemotherapy.
Onartuzumab
c-Met is a proto-oncogene encoding a membrane tyrosine kinase receptor – hepatocyte growth factor receptor (HGFR). HGFR plays an important role in tumor development through activation of key oncogenic pathways, angiogenesis, and tumor metastasis [55]. In gastric cancer patients, over-expression and amplification of c-Met often indicates poor prognosis [56-58]. c-Met inhibitors include monoclonal antibodies and small molecules that inhibit the enzymatic activity of the c-Met TK. Onartuzumab is a humanized monoclonal antibody directed against HGFR. A randomized, multicenter, doubleblind, placebo-controlled, phase III study evaluating the efficacy and safety of onartuzumab combined with mFOLFOX6 in patients with metastatic Her2-negative, c-Met positive gastroesophageal cancer is now ongoing (ClinicalTrials.gov Identifier: NCT01662869).
Pembrolizumab
Pembrolizumab is a highly selective, humanized IgG4/kappa isotype monoclonal antibody designed to block the interaction between PD-1 and its ligands, PD-L1 and PD-L2, thus reactivating the immune system to eradicate the host tumor. PD-1 is a negative co-stimulatory receptor expressed primarily on activated T cells. Binding of PD-1 to its ligands inhibits effector T-cell function. Expression of PD-L1 on tumor cells and macrophages can suppress immune surveillance and permit neoplastic growth. Pembrolizumab is able to achieve a dual blockade (PD-L1 and PD-L2) and shows no cytotoxic (ADCC/CDC) activity. The drug demonstrated a clinical activity in multiple tumor types, and recently became the first PD-1 inhibitor approved by the FDA when it was granted marketing approval for advanced melanoma.
The phase Ib study (Clinicaltrials.gov:NCT01848834) presented at ESMO 2014 assessed the safety, tolerability, and antitumor activity of pembrolizumab in gastric cancer patients [59]. Using a prototype IHC assay, PD-L1 expression was assessed in archival tumor samples from patients with recurrent/metastatic adenocarcinoma of the stomach or gastroesophageal junction. Eligible patients with PD-L1 staining in stroma or ≥ 1% of tumor cells were enrolled and treated with pembrolizumab 10 mg/kg every 2 weeks for up to 24 months or until complete response, disease progression, or unacceptable toxicity. Enrollment was designed to include an equal number of patients from Asia Pacific (AP) and the rest of the world (ROW). Of the 39 patients enrolled, 19 were from AP and 20 from ROW. AP patients were more likely to have received two or more therapies than ROW (79% vs. 55%). At a median follow-up of approximately 6 months, the ORR was 31% (31.6% in AP and 30% in ROW). Responses were ongoing for 6/6 Asia Pacific patients and 5/6 patients from the rest of world (median response duration not reached; range 8 + to 20 + weeks). Evidence of an association between PD-L1 expression and PFS (p = 0.032) and ORR (p = 0.071) was observed. The most common treatment-related adverse effects were hypothyroidism and fatigue. The author concluded that pembrolizumab was generally well tolerated and provided antitumor activity in patients with advanced gastric cancer that expressed PD-L1. These findings supported the potential of the PD-L1 pathway in gastric cancer and further development of pembrolizumab as a treatment option for patients with advanced gastric cancer. On the basis of the antitumor activity observed in this trial, a phase II study in advanced gastric cancer (KEYNOTE-059) is expected to begin enrollment in early of 2015.
Targeted therapies have showed promise for improving the current grim prognosis of advanced gastric cancer. Contemporary targeted cancer therapy has progressed rapidly over the past decade. The ToGA trial has marked the beginning of a new era in AGC treatment. The addition of trastuzumab to combination chemotherapy is now considered a standard first-line treatment for HER2 positive advanced GC patients. However, this benefit is limited to only approximately 20% of AGC patients (HER2-positive), and sooner or later it will be development of resistance.
Unfortunately, up to now, no similar encouraging results was obtained in other targeting agents except ToGA trial, we still have a long way to go. EGFR-targeted therapy has not been successful in gastric cancer to date. Antiangiogenic treatment in gastric cancer is now focused on ramucirumab, which was recently approved by the US FDA for the treatment of advanced gastric cancer or gastroesophageal junction adenocarcinoma with disease progression after prior platinum and fluoropyrimidine chemotherapy. Anti-HGF therapy is potentially effective in gastric cancer, but we have to wait for the results of Phase III trials. Another potentially interesting target is the modulation of immune checkpoints, such as PD-1 and PD-L1. The PD-1 inhibitor pembrolizumab has demonstrated promise in patients with gastric cancer. The development of drugs against stem cell characteristics will probably become another important new approach. A randomized phase III study (BRIGHTER) has now been started in which BBI608, is being investigated as second-line therapy in gastric/gastroesophageal junction cancer [60].
Targeted therapies are beginning to change the course of gastric cancer. However, at present, little is known about the outcome of gastric cancer patients after targeted therapies. Molecular heterogeneity, a defining feature of gastric tumors, is driven by mutations and other genetic alterations. As other malignacies, the signal pathways involving in the carcinogenesis and development of gastric cancer are interactive and complex. The further researches of the signal pathways network will help us understand better about the molecular mechanism of gastric cancer and figure out potential therapy targets.
The key goals of future studies in the research field of GC treatment should include the development of better combination for validated targets, more new effective agents for novel targets, and the detection of novel predictive molecular markers to identify better and optimal treatment modalities for metastatic gastric cancer. A number of phase III clinical trials are ongoing (Table 1). These novel agents, once verified and validated, may become the next ‘gold standard’ and, if combined with reliable biomarkers for resistance and response prediction, may ultimately introduce a new era of personalized medicine.
| Target | Agent | Trail | Regiment | N | Results |
|---|---|---|---|---|---|
| First-line | |||||
| VEGF | Bevacizumab | AVAGAST | XP+ Bevacizumab | 774 | Negative |
| EGFR | Panitumumab | REAL-3 | EOC+ Panitumumab | 553 | Negative |
| EGFR | Cetuximab | EXPAND | CP+ Cetuximab | 904 | Negative |
| HER2 | Trastuzumb | ToGA | XP+Trastuzumb | 584 | Positive |
| HER2 | Lapatinib | LOGiC | Capox+ Lapatinib | 545 | Negative |
| HER2 | Pertuzumab | JACOB | XP+Trastuzumb+ Pertuzumab | 780 | Ongoing |
| HGF/c-MET | Rilotumumab | RILOMET-1 | ECX+ Rilotumumab | 450 | Ongoing |
| HGF/c-MET | Onartuzumab | MetGastric | FOLFOX+ Onartuzumab | 800 | Ongoing |
| Second-line | |||||
| VEGFR2 | Ramucirumab | REGARD | BSC+ Ramucirumab | 355 | Positive |
| VEGFR2 | Ramucirumab | RAINBOW | Paclitaxol+ Ramucirumab | 665 | Positive |
| HER2 | Lapatinib | TyTAN | Paclitaxol+ Lapatinib | 261 | Negative |
| mTOR | Everolimus | GRANITE-1 | BSC+ Everolimus | 656 | Negative |
| mTOR | Everolimus | AIO-STO-0111 | Paclitaxol+ Everolimus | 480 | Ongoing |
| HER2 | T-DM1 | GATSBY | Paclitaxol vs T-DM1 | 412 | Ongoing |
| PARP | Olaparib | GOLD | Paclitaxol + Olaparib | 500 | Ongoing |
Table 1: Phase III studies of targeted agents in AGC