Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
![]() +44 1478 350008
+44 1478 350008
ISSN: 2165-7092
![]() +44 1478 350008
+44 1478 350008
Research Article - (2014) Volume 4, Issue 2
Aim: Although most Pancreas Transplants (PTs) are currently performed with exocrine enteric drainage, <20% also incorporate portal venous delivery of insulin (portal-enteric drainage). The purpose of this study was to analyze outcomes according to surgical technique.
Methods: We retrospectively reviewed outcomes in 202 consecutive PTs in 192 patients at our center. All patients received either r-ATG or alemtuzumab induction with tacrolimus/mycophenolate ± steroids.
Results: From 11/01 to 3/13, we performed 162 simultaneous kidney-PTs (SKPT), 35 sequential PTs after kidney, and 5 PTs alone (40 solitary PTs). A total of 179 (89%) were performed with portal-enteric and 23 with systemic-enteric drainage; all PTs were initially approached as intent-to-treat with portal-enteric drainage. Indications for systemic-enteric drainage were pancreas retransplantation following primary PT with portal-enteric drainage (N=9), central obesity (N=7), and unfavorable vascular anatomy (n=7). The systemic-enteric drainage group was characterized by more pancreas retransplants (39% versus 4%, p<0.0001), more solitary PTs (35% versus 18%, p=0.09), more African-Americans (39% versus 17%, p=0.02) and more patients with C-peptide positive diabetes (30% versus 13%, p=0.054) compared to the portal-enteric drainage group. Although the proportions of male recipients (70% versus 56%), recipients = 80 kg (30% versus 24%), and early relaparotomy rates (48% versus 36%) were all numerically higher in systemic-enteric versus portal-enteric PTs, respectively, none of these differences were significant. The incidence of early PT thrombosis was 4% in systemic-enteric compared to 8% in portal-enteric PTs (p=NS). With a mean follow-up of 5 years in systemic-enteric compared to 6 years in portal-enteric PT recipients, respective patient survival (70% versus 84%) and pancreas graft survival (61% versus 60%) rates were comparable; respective death-censored kidney graft survival (81% versus 82%) rates were similar.
Conclusion: In patients with disqualifying technical features for PT with portal-enteric drainage, comparable overall results can be achieved with systemic-enteric PT as a secondary technique.
<Keywords: Pancreas Transplantation; Systemic-bladder; Hyperinsulinemia
The history of pancreas transplantation (PT) has been closely intertwined with the evolution in surgical techniques.Advances in surgical techniques and clinical immunosuppression have led to improving results in vascularized PT that are attributed to reductions in technical failures and immunologic graft losses over time, respectively [1].According to Registry data, most PTs are performed with systemic venous delivery of insulin and either bladder (systemic-bladder) or enteric (systemic-enteric) drainage of the exocrine secretions [1]. Prior to 1995, more than 90% of PTs were performed by the standard technique of systemic-bladder drainage, usually using a duodenal segment conduit for exocrine drainage. Since 1995, the number of PTs performed with primary enteric exocrine drainage has increased dramatically and currently accounts for 91% of simultaneous kidney-PT (SKPT), 89% of sequential PT after kidney (PAK), and 85% of PT alone (PTA) cases[1].The latter 2 (PAK and PTA) categories are usually combined and analyzed together as solitary PTs because of similar albeit inferior outcomes compared to SKPT. At present, over 80% of enteric drained PTs are performed with systemic (iliac or vena cava) venous delivery of insulin, resulting in peripheral hyperinsulinemia [1]. In the non-transplant setting, systemic hyperinsulinemia has been associated with insulin resistance, dyslipidemia, accelerated atherosclerosis, and macroangiopathy.
To improve the physiology of PT, an innovative surgical technique of intraperitoneal portal venous drainage using an anterior approach to the superior mesenteric vein (SMV) was developed by Gaber et al. [2] and subsequently refined to a “retroperitoneal” or lateral approach by Boggi et al. [3] combining portal venous delivery of insulin with enteric drainage of the exocrine secretions (portal-enteric technique). However, the potential of portal-enteric drainage has never been fully realized as it currently accounts for only 18% of SKPT and PAK and 10% of PTA transplants [1]. A number of studies have demonstrated no major or consistent differences in outcomes for bladder-drained or enteric-drained PTs with either portal or systemic venous drainage [4-8]. Although nearly all PTs are currently performed with one of the three above techniques, current philosophy dictates that the most appropriate technique to be performed is the one with which the surgical team has the most experience. At our center, we have extensive experience with each technique but currently perform portal-enteric drainage preferentially using the anterior approach to the SMV. The purpose of this study was to analyze our experience in PT with systemic-enteric drainage when portal-enteric drainage was not considered possible or safe.
Recipient selection
Indications for PT were insulin-requiring diabetes with complications and the predicted ability to tolerate the operative procedure and manage the requisite immunosuppression and close follow-up irrespective of C-peptide production [9,10]. Selection criteria for SKPT in “type 2” diabetes included patients <55 years of age with a body mass index (BMI) <30 kg/m2, insulin-requiring for a minimum of 3 years with a total daily insulin requirement <1 u/kg/day, a fasting C-peptide level <10 ng/ml, absence of severe vascular disease or tobacco abuse, adequate cardiac function, and presence of "complicated" or hyperlabile diabetes [9,10]. Selection criteria for solitary PT were similar to SKPT except for renal function, in which the calculated glomerular filtration rate was >70 ml/min/1.73m2 in PTA (native renal function) and >40 ml/min/1.73m2 in PAK (renal allograft function) recipients who were already receiving a calcineurin inhibitor. Donor selection was more stringent for solitary PT, including younger donors and a minimum of a 2-3 human leukocyte antigen (HLA) match [9,11].
Technical aspects
All patients were T- and B-cell negative by flow cytometry crossmatch. All PTs were initially approached as intent-to-treat with portal-enteric drainageusing an anterior approach to the SMV and enteric exocrine drainage to the proximal ileum in the recipient (side to side duodeno-enterostomy, usually without a diverting Roux limb) [9,12]. Diverting Roux limbs were used rarely and only if the donor duodenum did not reperfuse well. Arterial inflow was usually based on the recipient's right common iliac artery after the pancreas dual artery blood supply was reconstructed with a donor common iliac bifurcation "Y" graft [13]. Relative “contraindications” to portal venous drainage were a small SMV (<6mm in diameter); a deep, buried, or inaccessible SMV (usually associated with central obesity, particularly in recipients with a Body Mass Index [BMI]>30 kg/m2); a sclerotic or partially thrombosed SMV or history of venous thrombosis from a previous PT with portal venous outflow; portal hypertension; or an arterial “Y” graft that would not reach a soft target either on the iliac artery or aorta (Table 1) [9,12]. In patients (particularly male) with a high BMI, the SMV can be quite deep in the mesentery and the donor common iliac artery bifurcation "Y" graft might not be long enough to reach the recipient's iliac artery through a window in the distal ileal mesentery, even with the liberal use of a donor artery "extension" graft. In these cases, systemic venous and enteric drainage were performed to simplify the procedure.Of the first 121 SKPTs, all but two were performed by transplanting the kidney to the left iliac vessels and the pancreas to the right common or external iliac artery through a midline intraperitoneal approach. However, since 7/30/10, nearly all SKPTs were performed with ipsilateral placement of the kidney and pancreas to the right iliac vessels in order to reduce operating time and to preserve the left iliac vessels for future transplantation.
| Venous: | Small SMV (<6mm in diameter) |
| Deep, buried, or inaccessible SMV (usually | |
| associated with central, omental, or mesenteric | |
| obesity or BMI >30 kg/m2) | |
| Sclerotic or partially thrombosed SMV | |
| History of venous thrombosis from a previous PT with portal venous outflow | |
| Portal hypertension | |
| Arterial: | Severe proximal iliac artery or aortic atherosclerosis (absence of soft target) |
| Short or absent “Y” graft available for arterial reconstruction of the pancreas graft | |
| Bowel: | Severe mid-abdominal adhesions (i.e.-sclerosing encapsulating peritonitis, multiple prior laparotomies) |
Table 1: Potential Contraindications to PT with Portal-Enteric Drainage Using the Anterior Approach
Anti-coagulation
In solitary PTand selected SKPT recipients, 2000-3000 units of intravenous heparin (30-50 units/kg) were administered as a single dose during surgery prior to implantation of the pancreas and a heparin infusion was continued post-transplant (continuous infusion of 300 units/hour for 24 hours, then 400 units/hour for 24 hours, and then 500 units/hour until post-operative day 5) in the absence of bleeding [14]. Indications for intravenous heparin included solitary PT, preemptive SKPT, history of thrombophilia or clotting disorder in the recipient, small or diseased donor or recipient vessels, prolonged pancreas cold ischemia (>15 hours), extended donor criteria, or history of prior pancreas graft thrombosis [9,14].
Immunosuppression
Patients received depleting antibody induction with either alemtuzumabor alternate day rabbit anti-thymocyte globulin(1.5 mg/kg/dose, total 3-5 doses) in combination with tacrolimus, mycophenolatemofetil (MMF), and tapered steroids or early steroid withdrawal [9,15,16]. Steroids were completely stopped on post-operative day #5 unless the patient was identified as “high immunological risk” defined by the presence of delayed (kidney) graft function, retransplantation, African American (AA) patient <40 years of age, allosensitization (pre-transplant panel reactive antibody [PRA] level >20%), or PTA. Since 2009, all PT recipients at our center (n=74) have received alemtuzumab induction with tacrolimus, MMF, and either early steroid elimination or rapid prednisone taper (dose reduction to 5 mg/day by 2 months following PT if determined to be high immunological risk) [15,16]. All patients received anti-infective prophylaxis with cefazolin for surgical site prophylaxis, fluconazole, valganciclovir, and trimethoprim-sulfamethoxazole. Anti-platelet therapy, consisting of oral aspirin (81 mg/day) was administered to all patients. Treatment of hypertension, hyperlipidemia, anemia, and other medical conditions was initiated as indicated, aiming to maintain the blood pressure <140/90 mm Hg, fasting serum cholesterol <200 mg/dl, and hematocrit>27%.
Statistical analysis
Data were compiled from both prospective and retrospective databases, with confirmation by medical record review in accordance with local Institutional Review Board guidelines and approval. For categorical variables, the chi-square test was applied, and Fisher's exact test was used when data were sparse. Categorical data were summarized as proportions and percentages and continuous data were summarized as means and standard deviations.Cumulative survival curves were estimated by Kaplan-Meier analysis.A two-tailed p-value of <0.05 was considered to be significant. Based on limitations in study design (retrospective study with a marked difference in sample size between the two groups) and the lack of significance for outcome variables in univariate analysis, we refrained from performing a multivariate analysis and present our findings mainly in a descriptive fashion.
From 11/1/01 through 3/1/13, 202consecutive PTs were performed in 192 patients, including 162 SKPT, 35 sequential PAK, and 5 PTA (40 SPTs).A total of 186 PTs (92%) were primary and 16 pancreas retransplants (10 of which had their primary PT performed at our center). All but 4 patients received kidney and PTs either simultaneously or sequentially (one patient received a kidney following a PTA).PT with portal-enteric drainage was performed preferentially in 179 cases; however, systemic-enteric drainage was performed in 23 cases (11%) in which portal-enteric drainage was not deemed possible or safe.Indications for systemic-enteric drainage were pancreasretransplantation (n=9, in which the primary PT was performed with portal-enteric drainage), central obesity (n=7), and difficult vascular anatomy (n=7). The decision to abort portal venous drainage and switch to systemic venous drainage was made intra-operatively in all cases.Demographic and clinical features of the two groups according to surgical technique of PT are listed in Table 2. The systemic-enteric technique was employed in 56% of pancreas retransplants versus 7.5% of primary PTs (p<0.0001). The systemic-enteric drainage group was characterized by more solitary PTs (35% versus 18%, p=0.09), more AA patients (39% versus 17%, p=0.02) and more patients with C-peptide positive diabetes (30% versus 13%, p=0.05) compared to the portal-enteric drainage group. In addition, the systemic-enteric group had proportionately more SKPT patients on hemodialysis with a longer pretransplant duration of dialysis compared to the portal-enteric group. Although the proportions of male recipients (70% versus 56%), recipients = 80 kg body weight (30% versus 24%), and early relaparotomy rates (48% versus 36%) were all numerically higher in systemic-enteric versus portal-enteric PTs, respectively, none of these differences were significant (Table 2).
| Mean ± SD | Systemic-enteric N = 23 |
Portal-enteric N = 179 |
p-value |
|---|---|---|---|
| Donor age (years) | 24.2 ± 9.0 | 26.5 ± 11.0 | NS |
| Donor weight (kg) | 70.9 ± 14.2 | 72.0 ± 15.8 | NS |
| Donor BMI (kg/m2) | 22.8 ± 4.7 | 24.0 ± 3.9 | NS |
| Cold ischemia time (hours) | 16.4 ± 4.8 | 15.9 ± 3.8 | NS |
| HLA-mismatch | 3.7 ± 1.4 | 4.4 ± 1.2 | NS |
| PRA >10% | 5 (21.7%) | 30 (16.8%) | NS |
| CMV D+/R- | 2 (8.7%) | 52 (29.1%) | 0.04 |
| Retransplant | 9 (39.1%) | 7 (3.9%) | <0.001 |
| Solitary PT | 8 (34.8%) | 32 (17.9%) | 0.09 |
| Recipient age | 44.8 ± 12.1 | 42.9 ± 9.4 | NS |
| Recipient gender: Male | 16 (69.6%) | 100 (55.9%) | NS |
| Recipient:African American | 9 (39.1%) | 30 (16.8%) | 0.02 |
| Recipient weight (kg) | 74.3 ± 14.0 | 70.7 ± 12.6 | NS |
| Recipient weight≥ 80 kg | 7 (30.4%) | 43 (24.0%) | NS |
| Dialysis history:SKPT Hemodialysis Peritoneal Dialysis None (preemptive) |
12/15 (80%) 1/15 (6.7%) 2/15 (13.3%) |
71/147 (48.3%) 41/147 (27.9%) 35/147 (23.8%) |
0.028 |
| Duration of dialysis: SKPT (months) | 39.3 ± 34.6 | 17.8 ± 15.6 | 0.03 |
| Duration of diabetes (years) | 27.0 ± 9.5 | 25.3 ± 8.4 | NS |
| PT waiting time (months) | 9.8 ± 6.9 | 9.2 ± 6.0 | NS |
| C-peptide positive pretransplant | 7 (30.4%) | 23 (12.8%) | 0.054 |
| Patient survival | 16 (69.6%) | 151 (84.4%) | 0.086 |
| Death with functioning grafts | 5 (21.7%) | 15 (8.4%) | 0.059 |
| Kidney graft survival | 13 (56.5%) | 126/175 (72%) | NS |
| Death-censored kidney graft survival | 23/16 (81.3%) | 126/154 (81.8%) | NS |
| Pancreas graft survival | 14 (60.9%) | 107 (59.8%) | NS |
| Death-censored pancreas graft survival | 14/18 (77.8%) | 107/161 (66.5%) | NS |
| Follow-up (months) | 60 ± 37 | 74 ± 29 | NS |
| Relaparotomy | 11 (47.8%) | 64 (35.8%) | NS |
| Early thrombosis | 1 (4.3%) | 14 (7.8%) | NS |
| Days of initial hospital stay | 12.5 ± 7.2 | 10.9 ± 8.2 | NS |
| Readmissions | 15 (65.2%) | 104 (58.1%) | NS |
| Acute rejection | 6 (26.1%) | 52 (29.1%) | NS |
| Major infections | 15 (65.2%) | 100 (55.9%) | NS |
Table 2: Donor and Recipient Characteristics and Outcomes According to Surgical Technique
The incidence of early PT thrombosis was 4% in systemic-enteric compared to 8% in portal-enteric PTs (p=NS). With a mean follow-up of 60 months in systemic-enteric versus 74 months in portal-enteric PT recipients (range 1-12.5 years, 140 patients had a minimum follow-up of 5+ years), respective actual patient (70% versus 84%, p=0.086), kidney (56.5% versus 72%), and pancreas graft (61% versus 60%) survival rates were comparable (Table 2). Actuarial patient and pancreas graft survival rates are depicted in Figures 1 and 2 (p=NS). The incidence of death with functioning grafts was slightly higher in systemic-enteric compared to portal-enteric PT recipients (22% versus 8%, p=0.06). Death-censored kidney (81.3% versus 81.8%) and pancreas (77.8% versus 66.5%) graft survival rates were likewise comparable in the systemic-enteric and portal-enteric groups, respectively (Table 2). There were no differences in length of initial hospital stay or rates of readmissions, acute rejection, or major infection between the two groups (Table 2).
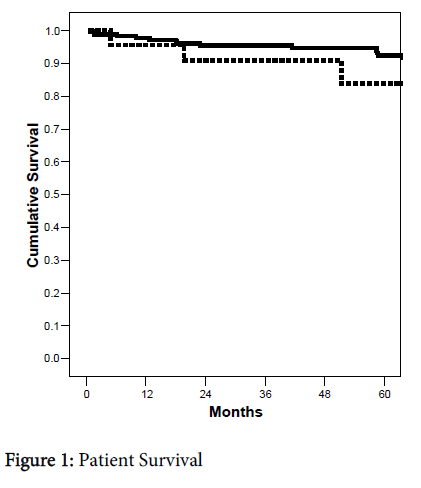
Figure 1: Patient Survival
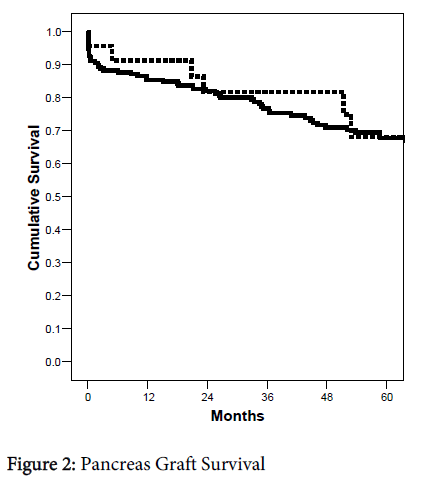
Figure 2: Pancreas Graft Survival
With improvements in organ retrieval and preservation technology, refinements in diagnostic and therapeutic technologies, advances in clinical immunosuppression and antimicrobial prophylaxis, and increased experience in donor and recipient selection, success rates for PT have steadily improved [1,17]. For recipients of primary deceased donor pancreas transplants, one-year patient survival is more than 95% in all 3 categories; unadjusted five-year patient survival rates are 87% in SPK, 83% in PAK, and 89% in PTA recipients; and more than 70% of patients are alive at ten years post-transplant [1,17]. One-year pancreas graft survival (insulin-free) rates are 85.5% in SPK (93% kidney graft survival), 80% in PAK, and 78% in PTA recipients, which translates to pancreas graft half-lives approaching 14 years in SPK and 10 years in solitary pancreas transplant recipients [1,17]. According to Registry data, PT outcomes are comparable regardless of surgical technique. In contrast to other treatments for diabetes, pancreas graft survival is largely defined as complete insulin independence concomitant with the absence of abnormal glycemic excursions.
The optimal surgical technique in PT remains controversial. All surgical techniques of PT share common ground with respect to organ donor selection and management, organ assessment and procurement, organ preservation, and back bench preparation of the pancreas [11,13].
Being familiar with multiple surgical techniques of PT is helpful because the optimal technique may need to be individualized based on anatomic issues.Purported benefits of PT with portal venous outflow include technical, metabolic, and immunologic “advantages” [2-9,12]. However, these benefits have not been confirmed by either prospective cohort studies, randomized controlled trials, or large analyses based on registry databases [1,4-8,12]. Alternatively, there are likewise no well controlled studies to suggest any major disadvantages or unique risks associated with portal venous outflow other than technical considerations. In this study, we chose to focus on technical “contraindications” and analyzed our experience with systemic-enteric drainage as a “rescue” or secondary technique of PT when portal-enteric drainage was not deemed safe.
An advantage of portal venous outflow is that the PT is primarily a mid-abdominal rather than a pelvic procedure, which is beneficial in patients who have had previous pelvic transplants or otherlower abdominal procedures.In patients with primary pancreas graft thrombosis following portal-enteric drainage, however, we preferentially chose to perform pancreas retransplantation with systemic-enteric (n=8) rather than repeat portal-enteric (N=1) drainage even though the latter technique is possible [18]. Our rationale for this decision was based on the fact that the recipient’s common iliac vein or distal inferior vena cava provided a larger conduit for venous outflow than the SMV. Whether this actually translates into a lower risk of PT thrombosis is unknown, particularly since the etiology of PT thrombosis is multifactorial [14]. Consequently, it is not surprising that the systemic-enteric group was characterized by more retransplants and solitary PTs because the majority of retransplants are performed as solitary PTs.
A potential disadvantage of the mid-abdominal or anterior approach to the SMV is that the arterial anastomosis may be difficult and require a long interposition “Y” graft (especially in patients with central, omental, or mesenteric obesity or in patients with severe proximal iliac vascular disease). In addition, the SMV may be small, deep or difficult to access in patients with this type of body habitus. Consequently, it is also not surprising that our systemic-enteric group was characterized by more patients with either a larger body habitus or type 2 diabetes phenotype (AA, C-peptide positive, male, higher body weight). In our experience, other potential contraindications to portal-enteric drainage using the anterior approach are listed in Table 1. In addition to the lateral or retroperitoneal approach introduced by Boggi [3], a number of other variations of portal-enteric drainage have evolved over the years to minimize technical challenges including the use of diverting Roux-en-y limbs for the enteric anastomosis (either with or without a venting jejunostomy), duodeno-gastric drainage, and, more recently, duodeno-duodenal drainage [12,19-30].
Based on this experience, we conclude that in patients with disqualifying technical features for PT with portal-enteric drainage, comparable overall results can be achieved with systemic-enteric PT as a secondary technique. We believe that the trends towards diminished patient survival and higher incidence of death with functioning grafts in the systemic-enteric group are probably not directly related to surgical technique but rather a consequence of differences in the composition of the patient population (more retransplants, longer duration of pretransplant dialysis, fewer preemptive transplants, more AA and C-peptide positive patients). Although numerous variations exist in the basic surgical techniques of PT and nuances continue to be described, we believe that the most appropriate technique to be performed should be determined by donor and recipient anatomy as well as the comfort level and experience of the surgical team with each technique.