Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2014) Volume 4, Issue 1
Purpose: To study the MRI findings and clinical features of pancreatic carcinoma with the first symptom of acute pancreatitis.
Materials and Methods: Twelve patients with pancreatic carcinoma and the first symptom of acute pancreatitis were included in this study. Pancreatic carcinoma with acute pancreatitis was confirmed by pathology. The MRI findings and clinical features of pancreatic carcinoma combined with acute pancreatitis were noted.
Results: In the 12 patients with acute pancreatitis, the pancreas appeared edematous and non-necrotic on MRI. The pancreatic carcinomas were mainly located in the head of the pancreas (83.33%, 10/12). Most patients showed a mass on T1-weighted and T2-weighted images. A dilated pancreatic duct and/or Common Bile Duct (CBD) was observed on MRI of 75% (9/12) of the patients. The results of laboratory tests demonstrated increased CA19-9 in 8 of the patients (66.67%), elevation of both ALP and AST in 11 of the patients (91.67%), and normal ALP and AST levels in 1 patient.
Conclusions: Acute pancreatitis may be an indicator of pancreatic carcinoma. A pancreatic mass and a dilated pancreatic duct and/or CBD observed by MRI can provide evidence of the associated pancreatic carcinoma. Increased levels of ALT, AST or ALP and CA19-9 may aid the diagnosis of pancreatic carcinoma in cases of acute pancreatitis.
Keywords: Pancreas, Pancreatitis, Carcinoma, Magnetic resonance imaging
The incidence of pancreatic carcinoma, one of the most aggressive malignant tumors, is increasing in the United States [1]. The insidious nature of pancreatic carcinoma stems largely from the inability to clinically detect its earliest forms [2].
The association of pancreatitis with carcinoma of the pancreas has been recognized and reported sporadically in the literature [1,3]. Acute pancreatitis may be the initial presentation of pancreatic carcinoma, although the frequency of this phenomenon is as low as 3% [4].
As early as in 1953, Israels [5] reported that patients with carcinoma in the head of the pancreas had relapsing pancreatitis. Balthazar et al [6] described the role of Computed Tomography (CT) in the preoperative diagnosis of pancreatitis associated with pancreatic carcinoma. There are also some case reports of patients with AP who had pancreatic carcinoma; most of the patients had a characteristic history, symptoms and clinical signs [3-6]. Tummala et al [3] reported that Endoscopic Ultrasound (EUS) can be used for diagnosing Nonalcoholic Non-Gallstone-related (NANG)acute pancreatitis associated with pancreatic carcinoma, but the use of this instrument is an invasive method for detecting space-occupying lesions of the pancreas. Therefore, the prompt and accurate diagnosis of pancreatic carcinoma with the first symptom of acute pancreatitis is imperative.
The role of Multislice Spiral Computed Tomography (MSCT) imaging in screening patients with acute and chronic pancreatitis is significant. Magnetic Resonance Imaging (MRI) of the pancreas has undergone a major change because it can provide noninvasive images of the pancreatic ducts and the parenchyma [7]. MRI of the pancreas employs several pulse sequences, such as T1-weighted, T2-weighted and fat saturation imaging, MR Cholangiopancreatography (MRCP) and dynamic gadolinium-enhanced imaging. MRI can replace CT examination or may be useful as a secondary noninvasive modality to characterize and better evaluate equivocal CT findings. MRI is a valuable tool in the assessment of the full spectrum of pancreatic diseases [8] and has the potential to detect small or early pancreatic carcinoma.
Our purpose is to present the MRI findings, discuss their utility in the evaluation of pancreatic carcinoma with the first symptom of acute pancreatitis and correlate the MRI findings with the clinical features.
Study Population
This investigation was conducted with the Institutional Review Board approval for retrospective studies in our institute. Patient informed consent was waived. We performed a retrospective analysis of the patients in our patient database who presented from January 2005 to December 2012 with the inclusion requirements. These patients were subsequently enrolled into our study. The inclusion criteria included the following: (1) the first typical clinical manifestations of acute pancreatitis. (2) Laboratory test values of serum amylase or urinary amylase that were more than three times greater than normal or a surgical pathological diagnosis of pancreatic carcinoma with acute pancreatitis. (3) Having had abdominal MRI examination within 48 hours of the onset of symptoms. (4) Pancreatic carcinoma confirmed by surgery. The exclusion criteria included the following: (1) Pancreatic carcinoma as the first symptom, secondary to acute pancreatitis. (2) Having a history of chronic pancreatitis. (3) Having symptom of acute pancreatitis but had been diagnosed with pancreatic carcinoma pre-admission. (4) Having gall stones or alcohol consumption. The results of the clinical and laboratory tests of all of the patients whose initial diagnosis was acute pancreatitis were examined, but all of the patients were diagnosed with pancreatic carcinoma by pathology.
Finally, 12 patients were enrolled into this study, including 9 males and 3 females with an average age of 57 ± 10 years (ranging from 46 to 72 years).
Clinical Manifestations
Nine of the 12 patients had abdominal pain without any obvious incentives during the month before admission. The abdominal pain lies in the paroxysmal upper or lower abdominal and increased after eating. Nine of the patients experienced abdominal pain accompanied by waist pain, which 4 of the 9 patients could alleviate by stooping; 2 of the patients had acute abdominal pain after eating a fatty meal or a surfeit of food. Three patients who were diagnosed with acute pancreatitis were admitted to the hospital for treatment and had acute abdominal pain after being discharged from the hospital, which caused them to be readmitted. Seven of the patients had nausea and vomiting.
MR Imaging Techniques
MR imaging was performed using a 1.5-T MR scanner with 38 mT/M gradients and a 120 mT/M per second slope (Signa Excite; GE Medical Systems, Milwaukee, WI) with a phased array torso-pelvis coil. The sequences included the following: axial fast spoiled gradient echo (FSPGR) T1-weighted imaging with fat suppression (repetition time [TR] ms/echo time [TE] ms = 150170/1.6; flip angle = 80; matrix = 512160192; field of view (FOV) = 2632 cm; section thickness = 5 mm; number of excitation (NEX) = 1), gradient-echo (GRE) T1-weighted in-phase and out-of-phase MR imaging (TR ms/TE ms = 150/4.4, 2.2; flip angle = 90; matrix = 256192224; FOV= 2632 cm; section thickness = 5 mm; NEX= 1), respiratory-triggered (R-T) axial fast recovery fast spin-echo (FRFSE) T2-weighted MR imaging with fat suppression (TR ms/TE ms = 10,00012,000/90100, with TR determined by the frequency of respiration; section thickness = 5 mm; intersection gap = 0.5 mm; matrix = 256192; NEX = 3; and FOV = 34 cm 34 cm), coronal and axial Single Shot Fast Spin-Echo (SSFSE) T2-weighted MR imaging (TE = 90100 ms; 2 s between slice acquisitions; section thickness = 5 mm; intersection gap = 0.5 mm; matrix = 384 224; one-half signal acquired; and FOV = 33 cm 33 cm), SSFSE radial series slabs MR Cholangiopancreatography (MRCP) (TE = 1300 ms; 6 s between image acquisitions; section thickness = 40 mm; matrix = 384 224; one-half signal acquired; FOV = 30 cm 30 cm), and three-dimensional (3D) FSPGR dynamic contrast-enhanced MR imaging. Dynamic contrast-enhanced imaging was performed using an axial fat saturated 3D FSPGR sequence. Gadolinium chelate (Magnevist, Schering Guangzhou Co., China) was administered (0.2 mmol per kilogram of body weight) intravenously at approximately 3.5 ml/s by projector (Spectris MR Injection System, Medrad Inc., USA) injection, followed by a 20-mL saline solution flush. Three enhanced phases were acquired, including the arterial dominant, portal venous, and delayed phases of contrast enhancement.
Indicators of Liver Function and a Tumor Marker
After admission to the hospital, 3-4 ml of fasting venous blood was collected from the patients within 24 hours. The levels of serum CA19-9 and the liver function indicators were determined using a Laison 2229 automated luminescence analyzer and reagents and an automatic biochemical analyzer (Beckmann, CX800, Italian Diasioni Company). We selected the key liver indicators that reflect liver damage [9]. These indicators included aspartate aminotransferase (AST, reference range: 5.0-40 U/L)alanine aminotransferase (ALT, reference range: 5.0-40 U/L) and alkaline phosphatase (ALPreference range: 15.0-110 U/L). CA19-9 (reference range: 0-37 U/m L) is a specific marker for the diagnosis of pancreatic carcinoma.
MR Image Observations
Two observers (with 4 and 6 years of experience in interpreting abdominal MRI images) who were blinded to the laboratory data and clinical outcomes reviewed the MR images to discern the patterns in and beyond the pancreas.
The MRI observations included signal intensity of pancreatic tumors, and enhanced modes after administration of the contrast agent in pancreatic tumors, thickening of the anterior renal fascia, stranding or fluid collection in the peripancreatic fatty space, dilation of the Common Bile Duct (CBD) and the Main Pancreatic Duct (MPD), and interruption of the MPD. An MPD with a diameter of >3 mm was defined as dilated, as was a CBD with a diameter >8 mm [10]. The diameter of the second lumbar vertebra (L2) was the reference used to determine the size of the pancreas [11]. The severity of the acute pancreatitis was graded using the MR severity index (MRSI) [12]. According to the MRSI [13], acute pancreatitis is graded as mild (0-3 points), moderate (4-6 points) or severe (7-10 points).
Statistical Analyses
The data derived from MRI were expressed as the average of the two observers findings. Any discrepancies in the non-continuous data were negotiated by the two observers until a consensus was reached. The inter-rater agreement for the final MR diagnoses of the two observers was expressed as the mean kappa (k) value.
Patient Samples
Twelve patients underwent tumor resection. Surgery revealed a pancreatic mass in each (12/12) of the patients. The average size of the 12 tumors was 3.2 ± 1.5 cm (ranging from 1.8 to 5.4 cm). Two of the patients (16.67%, 2/12) had poorly differentiated tumors, six of the patients (50.0%, 6/12) had moderately differentiated tumors and four of the patients (33.33%, 4/12) had well-differentiated tumors.
MR Finding of Acute Pancreatitis and Pancreatic Carcinoma
The agreement between the observers regarding the pancreatic mass and its signal intensity and dilated CBDs and MPDs was satisfactory (κ= 0.63-0.67, P<0.05).
In the twelve patients, 33.3 % (4/12) of the tumors were hypointense on T1 weighted images and hyperintense on T2 weighted images (Fig. 1A and 1B), 50% (6/12) of the pancreatic tumors appeared isointense on both T1 weighted images and T2 weighted images (Fig. 2A and 2B) and 16.67% (2/12) of the tumors appeared isointense on T1 weighted images and hyperintense on T2 weighted images (Tab. 1). Five of the twelve patients who had three-dimensional (3D) FSPGR dynamic contrast-enhanced MR imaging exhibited no enhancement in the arterial phase but gradually progressive enhancement in the delayed phase (Fig. 1D and 1E).
| Patients | T1WI | T2WI | Arterial Phase | Venous and delayed Phases |
|---|---|---|---|---|
| Group 1 (n=4) | hypointense | hyperintense | hypointense | slight enhancement |
| Group 2 (n=6) | isointense | Isointense | isointense | no enhancement |
| Group 3 (n=2) | isointense | hyperintense | isointense | slight enhancement |
Table 1: Signal intensity of pancreatic cancer on MRI
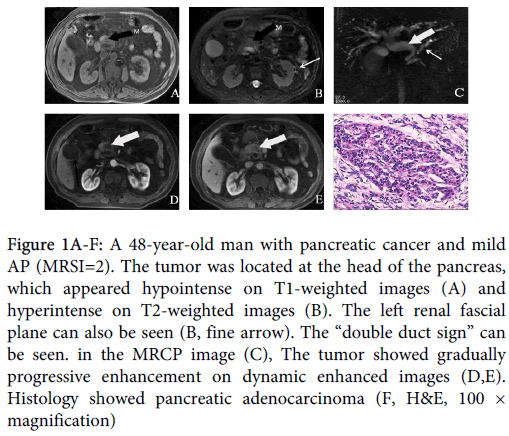
Figure 1A-F: A 48-year-old man with pancreatic cancer and mild AP (MRSI=2). The tumor was located at the head of the pancreas, which appeared hypointense on T1-weighted images (A) and hyperintense on T2-weighted images (B). The left renal fascial plane can also be seen (B, fine arrow). The “double duct sign” can be seen. in the MRCP image (C), The tumor showed gradually progressive enhancement on dynamic enhanced images (D,E). Histology showed pancreatic adenocarcinoma (F, H&E, 100 × magnification)
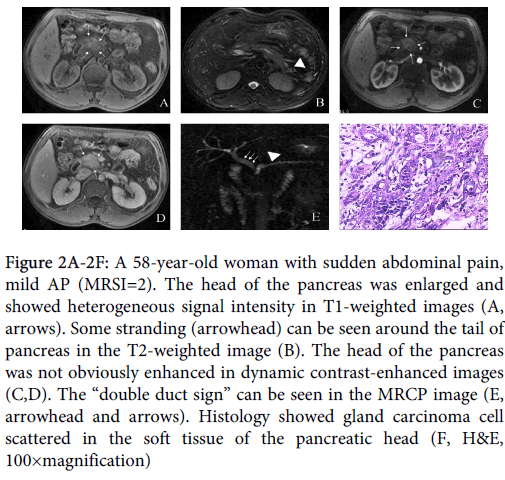
Figure 2A-2F: A 58-year-old woman with sudden abdominal pain, mild AP (MRSI=2). The head of the pancreas was enlarged and showed heterogeneous signal intensity in T1-weighted images (A, arrows). Some stranding (arrowhead) can be seen around the tail of pancreas in the T2-weighted image (B). The head of the pancreas was not obviously enhanced in dynamic contrast-enhanced images (C,D). The “double duct sign” can be seen in the MRCP image (E, arrowhead and arrows). Histology showed gland carcinoma cell scattered in the soft tissue of the pancreatic head (F, H&E, 100×magnification)
The main pancreatic duct was dilated in 75% (9/12) of the patients, and the CBD was dilated in 33.33% (4/12) of the patients. In three of the patients (25%, 3/12), both the main pancreatic duct and CBD were dilated (Tab. 2) (Fig.1C and 1E). Peripancreatic fatty space stranding was observed in 66.67% (8/12) of the patients. The eft renal fascial plane was thickened in 58.33% (7/12) of the patients, and 16.67% (2/12) of the patients had right renal fascial plane whose mass was located in the head of the pancreas. The acute pancreatitis appeared edematous and without necrosis on MRI.
| Patient no. | Sex | Age | Tumor location | Common bile duct | MPD | MPD disruption | Renal fascial plane |
|---|---|---|---|---|---|---|---|
| 1 | M | 46 | Head | Dilatation | Yes | right | |
| 2 | M | 50 | body | Dilatation | No | left | |
| 3 | M | 64 | Head | Dilatation | Dilatation | Yes | left |
| 4 | F | 58 | Head | Dilatation | Dilatation | No | No |
| 5 | M | 52 | body | Yes | left | ||
| 6 | M | 66 | Tail | Dilatation | No | No | |
| 7 | M | 68 | Head | Dilatation | No | left | |
| 8 | M | 47 | Head | No | left | ||
| 9 | M | 70 | body | Dilatation | No | left | |
| 10 | F | 72 | body | Dilatation | Yes | No | |
| 11 | F | 69 | Head | Dilatation | No | right | |
| 12 | M | 48 | Head | Dilatation | Dilatation | Yes | left |
| MPD: Main pancreatic duct | |||||||
Table 2: MRI findings in patients with acute pancreatitis and pancreatic cancer (n=12)
The agreement between the observers regarding the MRSI scores was satisfactory (κ= 0.76, P<0.05). The average MRSI score of the 12 patients was 2.75±0.87 points (ranging from 0 to 4 points). Approximately 83.33%, 16.67% and 0% of the patients had mild, moderate or severe acute pancreatitis, respectively, according to the MRSI scores.
Analysis of the Indicators of Liver Function and a Tumor Marker
Each of the 12 patients had been classified as having edematous pancreatitis and no necrotizing pancreatitis by MR imaging. The levels of ALT, AST or ALP were significantly increased in these patients. The levels of ALT or ALP and AST were increased in 91.67% (11/12) and 58.33% (7/12) of the patients, respectively (Tab. 3). The level of CA19-9 was increased in 58.33% (7/12) of the patients (Tab. 3). Four patients with a mass located in the head of the pancreas had elevated AST or ALT and a dilated CBD. Moreover, during the follow- up, we found that the AST levels of these 4 patients who were diagnosed with pancreatic carcinoma and acute pancreatitis were significantly lower 1-2 weeks following surgery.
| Patient no. | Sex | Age | Tumor location | ALT | AST | ALP | CA19-9 |
|---|---|---|---|---|---|---|---|
| 1 | M | 46 | Head | elevated | elevated | elevated | normal |
| 2 | M | 50 | body | elevated | elevated | elevated | normal |
| 3 | M | 64 | Head | elevated | normal | elevated | elevated |
| 4 | F | 58 | Head | elevated | normal | elevated | elevated |
| 5 | M | 52 | body | normal | elevated | elevated | normal |
| 6 | M | 66 | Tail | elevated | elevated | elevated | elevated |
| 7 | M | 68 | Head | elevated | normal | elevated | elevated |
| 8 | M | 47 | Head | elevated | elevated | elevated | elevated |
| 9 | M | 70 | body | elevated | elevated | elevated | normal |
| 10 | F | 72 | body | elevated | normal | elevated | elevated |
| 11 | F | 69 | Head | elevated | elevated | elevated | normal |
| 12 | M | 48 | Head | elevated | normal | normal | elevated |
Table 3: Levels of indicators of liver function and a tumor marker
In this study, we found that whether acute pancreatitis was associated with pancreatic cancer could be diagnosed early by a combination of clinical history, laboratory tests and MR imaging. Our results indicate that acute pancreatitis may be an indicator of pancreatic carcinoma and that MRI is useful for detecting tumors in patients with pancreatic carcinoma whose first symptom is acute pancreatitis. MRI screening may improve the management of patients with pancreatitis and pancreatic carcinoma, particularly those with pancreatic carcinoma in the early stage.
Previous studies reported that most pancreatic carcinomas appear slightly hypointense on T1 weighted images and slightly hyper intense on T2 weighted images and are clearly distinct from normal pancreatic tissue, which displays higher signal intensity. Following the administration of a contrast agent, these tumors usually exhibit lower signal intensity than the adjacent normal pancreatic tissue [14-17,19]. In this study, we found that more than half of the pancreatic tumors appeared isointense on T1WI and T2WI. The reason may be that pancreatitis decreased the signal intensity of the pancreatic parenchyma and therefore, the pancreatic tumors appeared isointense in the background of lower signal intensity. In addition, the characteristics of the pathological tissue in patients with pancreatic carcinoma and acute pancreatitis may be different. We also found that pancreatic tumors were not enhanced in the arterial phase but were gradually enhanced in the delayed phase. This progression may result from contrast agent entering the pancreatic tissue and slowly draining into the vein [20].
Acute pancreatitis can be grouped into mild and severe pancreatitis. In 80% of patients, acute pancreatitis is mild and resolves without serious morbidity, but in up to 20% of patients, acute pancreatitis is complicated by substantial morbidity and mortality [29]. In this study, we found that acute pancreatitis mostly appeared edematous and without necrosis on MRI and that the MRSI score of AP combined with PC is low. Our results were similar to those of Tummala et al. [3], who found that few patients with pancreatic necrosis occurring in the presence of pancreatic carcinoma presented with acute pancreatitis as the first symptom [3].
The indirect MRI indices for the diagnosis of acute pancreatitis without pancreatic carcinoma include peripancreatic and retroperitoneal fluid collection, peripancreatic and retroperitoneal fat changes and peritoneal and fascial abnormalities such as an incrassated anterior renal fascia [21-23]. In addition to the above-mentioned indices, in this study, we also found that patients with acute pancreatitis combined with pancreatic carcinoma had dilatation of the pancreatic duct, limited interruption of the MPD, and a dilated CBD. Larena and Patel et al reported that the main pancreatic duct is rarely dilated in acute pancreatitis [24,25]. Our results suggest that when the pancreatic duct and/or CBD are dilated in cases of acute pancreatitis, an associated pancreatic carcinoma could exist.
There is a very close and complex relationship between liver and pancreas. The liver function of the most of patients with pancreatic carcinoma and acute pancreatitis was abnormal. In acute pancreatitis, apoptosis of the pancreatic acinar cells releases trypsin, further promoting the release of a large number of inflammatory cytokines that cause liver injury [26]. The prevalence and degree of liver injury is related to the severity of acute pancreatitis [27]. However, in our study, most of the patients had mild acute pancreatitis, but their ALT, AST or ALP levels indicated serious liver damage. The reason for this finding could be the dual effects of a pancreatic mass blocking the biliary tract and pancreatitis factors. Our results indicated that pancreatic carcinoma could be detected when patients with acute pancreatitis had severely damaged livers.
The CA19-9 serum level in patients with pancreatic cancer is generally considered a clinical diagnostic marker of the tumor. Hámori [28] reported that the sensitivity of CA19-9-based detection of pancreatic carcinoma is between 69% and 93%. In this study, we found that the sensitivity of CA19-9 assay for detecting pancreatic carcinoma combined with acute pancreatitis is 58.33%. We speculate that CA19-9 may also be a marker of pancreatic carcinoma when acute pancreatitis is the first symptom of pancreatic carcinoma.
The limitation in this study is our relatively small sample size. Therefore, further studies involving a larger number of patients are needed to confirm whether the patients with acute pancreatitis had pancreatic carcinoma when dilation of the pancreatic duct and/or CBD occurred and/or ALT, AST or ALP and CA19-9 levels are increased.
In conclusion, acute pancreatitis in patients with pancreatic carcinoma is relatively rare. Acute pancreatitis may indicate the existence of pancreatic carcinoma. MRI is a reliable noninvasive screening examination that is able to detect pancreatic carcinoma associated with pancreatitis in the majority of patients. Pancreatic carcinoma could be diagnosed when a pancreatic mass and a dilated pancreatic duct and/or CBD are observed by MRI. Increased levels of ALT, AST or ALP and CA19-9 may aid the diagnosis of pancreatic carcinoma in cases of acute pancreatitis.