Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Case Report - (2012) Volume 2, Issue 4
Abstract Background: Pancreatic trauma in children is relatively uncommon, but carries high morbidity and mortality rates when diagnosis is delayed. Preoperative diagnosis of pancreatic lesion might be difficult, especially in the case of isolated injury. Methodology: We analyze two cases of pancreatic trauma in childhood in our institute. Both cases were managed conservatively and discharged from the hospital without any complications. Results: In one case child had development of pseudocyst after about two weeks of trauma which was managed conservatively with percutaneous drainage. In another case, child was managed conservatively without any intervention. Conclusion: We emphasize the importance of CT (Computerized tomography) scan and judiciously use non operative management in the treatment of pancreatic trauma.
<Keywords: Blunt trauma abdomen, Pancreatic injury, Non operative management
Blunt trauma to the abdomen accounts for the majority of abdominal injuries in children. Pancreatic injury is the fourth most common solid organ injury, following injuries to the spleen, liver and kidneys [1]. Pancreatic injury is a rare but severe complication occurring in 2-5% of blunt abdominal traumas. It is most often caused by compression of the gland against the lumbar part of the vertebral column. Due to contusion, the pancreas often ruptures completely [2,3]. Non-surgical management of minor pancreatic injury is well accepted, but the management of serious pancreatic injury in children remains controversial [4]. Pancreatic injuries often induce severe complications. Some centers recommend an aggressive surgical approach to reduce the incidence of pseudocyst formation and to prevent greater morbidity and prolonged hospitalization. Others advocate that non-surgical management of pancreatic injury in children leads to a good clinical outcome. Early diagnosis and adequate therapy of pancreatic trauma are essential for the prevention of complications. Correct diagnosis can be difficult in blunt abdominal trauma, especially in the case of isolated pancreatic injury, because retroperitoneal lesions do not have any specific symptoms [4,5]. We evaluated the data of 2 cases of pancreatic injury in childhood presented at our department.
Case 1
A 4 year old male child presented to our hospital with history of tractor door fall on his abdomen on 10/8/2012, later he complained of pain in abdomen and distension of abdomen for which he was shown at local hospital later he was referred to our institute. On admission, child had no history of hematemesis, malena and hematuria.
On examination, child was conscious cooperative with vitals pulse-90/min, BP-90/60 mmhg, no evidence of pallor. As per abdomen examination, it was revealed that there exists tenderness in epigastrium and left hypochondrium and distension in the upper abdomen. No evidence of any external injuries to chest.
His investigations were as follows
Hemoglobin-8.7 gm%,
Hematocrit-26%
Liver function test–SGOT-51 IU/L, SGPT-340 IU/L,
Serum lipase -285 IU/l, serum amylase-321 IU/l on admission
Serum amylase-402 IU/l, Serum Lipase-458 IU/l after two days of admission
Serum Ca-9.4 mg%, RBS-95 mg%, serum urea-34 mg%, serum creatinine-0.8 mg%
He had undergone Ultrasonography of abdomen; report stated minimal intraperitoneal free fluid, with no evidence of solid organ injury on the day of injury. In view of further evaluation, child was subjected to CECT (Contrast Enhanced Computerized Tomography) of abdomen, which revealed an irregular hypodense non enhancing area measuring 5.3 cm×9.0 cm in the left lobe of liver adjacent to falciform ligament with sub capsular collection. Irregular hypodense, non enhancing linear area measuring 2.0 cm was seen in the body of pancreas along its transverse axis and all other solid organs were normal. Minimal intraperitoneal fluid in the pelvis and general peritoneal cavity was also observed. The fluid aspirated from the peritoneal cavity revealed amylase - 1347 IU/l, protein- 4.2 gm%, LDH- 220 IU/L, cell count- 6800 cells/mm3, with predominant lymphocytes. On the 11th day of admission, the child had abdominal distension and fever; hence review USG (Ultrasonography) was planned which showed a large ill defined fluid collection with few septae, and echogenic debris within lesser sac measuring 13.4×10.5×6.4 cm was seen. The child had persistent fever hence blood culture was sent and it was negative; antibiotics were given for 5 days.
In view of persistent symptoms of abdominal distension and pain in abdomen, plan for percutaneous drainage was decided on 18th day of admission; pigtail catheter insertion under USG guidance was done; about 30 ml clear fluid was drained; catheter was kept for 12 days; for first few days 300 to 350 ml drain output was observed which gradually reduced in amount and was nil on the day 12 of insertion. A review USG revealed no collection; hence catheter was removed on 14th day. The child was asymptomatic after catheter removal, hence was discharged on 12/9/2012 (30 days after admission) (Figures 1 and 2).
Figure 1: Child with percutaneous drainage.
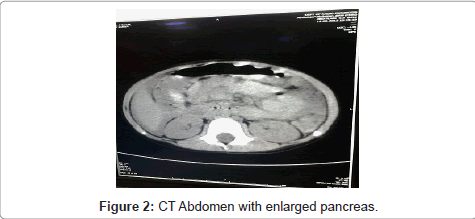
Figure 2: CT Abdomen with enlarged pancreas.
Case 2
A 11 year old male child history of self fall while coming from school on 30/8/2012 at 3 pm and sustained blunt trauma over abdomen was presented. There was no history of vomiting, abdominal distension or hematuria, but he complained of pain in abdomen since then; on examination there were no obvious external injuries, and his vitals are Pulse-90/min, BP-90/60 mmHg, with pain score of 6/10. As per abdomen examination, tenderness was revealed in the epigastrium with no guarding or rigidity. USG revealed Bulky pancreas with peripancreatic fluid collection 2.3×2 cm, with minimal free fluid in intraperitoneal cavity (Figures 3 and 4). Blood investigations were as follows: and electrolytes were normal (Table 2).
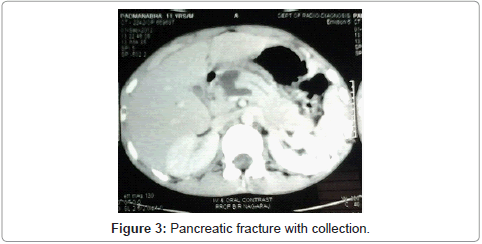
Figure 3: Pancreatic fracture with collection.
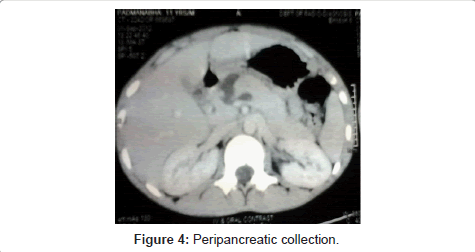
Figure 4: Peripancreatic collection.
| Investigation | 31/08/2012 | After 6 hours of admission |
1/9/2012 | 2/09/2012 |
| Haemoglobin (gm/ dl) | 10.7 | 12.1 | 11.2 | 10.8 |
| Hematocrit (%) | 31.8 | 36.4 | 33.6 | 32.6 |
| Serum Amylase | 1503 IU/L | 1656 | ||
| Serum Lipase | 965 IU/L | 1059 | ||
| SGOT | 17.9 IU/L | |||
| SGPT | 10.6 IU/L | |||
| Serum ALP | 151 IU/L |
Table 2: Results of the blood investigation-normal electrolytes.
Child was kept Nil per Oral for 3 days; pain was reduced on the day of admission with analgesics; in view of assessment of pancreatic injury, severity CECT abdomen was planned which showed pancreatic neck transection with fluid at transection site measuring 2.5×2.3 cm, and minimal fluid in the hepatorenal pouch. Child was asymptomatic for 1 week; again he complained of pain in abdomen with no h/o vomiting, fever or abdominal distension. Review USG revealed minimal fluid collection in the peripancreatic region with seepage of fluid into retro pancreatic tissue. Hence, the child was kept nil oral for 2 days after which pain reduced and no further increase in collection was observed; discharge was planned after 10 days of admission (Figures 3 and 4).
Pancreatic injuries are uncommon injuries constituting less than 10% of all abdominal injuries. Isolated pancreatic injuries are rare, most of the injuries associated with other solid organ injury.
Pancreatic injuries in blunt abdominal trauma are caused due to crushing of pancreas between vertebral column and another surface. It happens in thin individual due to lesser space between vertebral column and skin [6]. These represent major diagnostic challenge, retroperitoneal location of pancreas combined with reduced secretion and inactivity of pancreatic enzymes following injury may account for paucity of early physical signs [7,8]. Early deaths are from bleeding and late deaths due to infection. Diagnosis requires high level of suspicion, usually initial symptoms are non specific and vague, presents with mid epigastric pain or back pain following trauma. Physical signs include mild epigastric tenderness in the early period to frank peritonitis features in the late presentation. Elevation of serum amylase is not a specific sign of pancreatic injury. Enzyme levels increase only in 60-70% of patients in blunt abdominal c, and in even smaller proportion in penetrating injuries. In contrary elevated amylase values are present in one third of blunt abdominal trauma cases without pancreatic injury [3,4]. Continuous monitoring of enzyme values proved most effective. If constant elevation or continuous high values are present pancreas injury is probable.
CT scan is the most useful imaging technique for detecting parenchymal lesions in an early phase [5]. Suspicious signs can be thickening of the gland, surrounding edema or thickening of Gerota’s fascia. CT images did not directly detect disruption of the main pancreatic duct, but in our cases parenchymal lesions were correctly confirmed. Negative non-invasive examination does not exclude the possibility of pancreas lesion. If results of the CT scan are dubious or do not correlate with the clinical condition the procedure should be repeated. It is however important that repeated examination should be valued by the same radiologist. Pancreatic trauma was classified by the AAST (American Association for the Surgery of Trauma), (Table 1) which differentiates between five grades, the first case was grade II and second case was grade III injury, both managed conservatively [8-10].
| I. | Haematoma | Minor contusion without ductal injury |
| Laceration | Superficial laceration without ductal injury | |
| II | Haematoma | Major contusion without ductal or parenchymal injury |
| Laceration | Major laceration without ductal or parenchymal injury | |
| III | Laceration | Distal transection or parenchymal injury with ductal injury |
| IV | Laceration | Proximal transection or parenchymal injury affecting the ampulla |
| V | Laceration | Massive disruption of the pancreatic head |
Table 1: Classification of pancreatic injuries by the American Association for the Surgery of Trauma.
In the case of minor contusion or superficial laceration without duct injury conservative, non surgical treatment is justified [8]. Peripancreatic fluid collections, pseudocysts with no symptoms after minor blunt abdominal trauma follow up. In our case we had drained the pseudocyst under ultrasound guidance and child recovered well without ant complications.
Blunt pancreatic trauma continues to pose significant diagnostic and therapeutic challenges. In view of the numerous associated injuries, priority must be given to stabilizing the patient before any definitive management of the pancreatic injury. Non operative management plays major role in the management of pancreatic injuries. We emphasize on the usage of CT scan and Ultrasound scan in the management of pancreatic trauma.