Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Case Report - (2012) Volume 2, Issue 2
Conventional renal cell carcinoma (Grawitz tumour) represents the most frequent malignant tumour of the kidneys in adulthood. Metastasis occurs in more than 25% of cases, most frequently involving the bones (osteolytic metastases), lungs, brain, liver, adrenal glands and contralateral kidney. A single solitary metastasis is rare. Metastasis of the primary tumour occurs even many years after its removal. Pancreatic metastases are very rare and only anecdotal reports exist in literature. The authors describe here 2 case reports involving the diagnosis and successful removal of this rare metastasis. Both patients currently show no signs of tumour generalisation. Pancreatic metastases from renal cell carcinoma are a very rare entity. Patients with such metastases have a good prognosis if these are radically removed.
<Keywords: Pancreatic Metastases, Conventional Renal Cell Carcinoma, Surgical Treatment
CT - Computed Tomography
Renal cell carcinoma (Grawitz tumour, conventional renal cell carcinoma) represents the most frequent malignant tumour of the kidneys in adulthood. Metastasis occurs in more than 25% of cases, most frequently involving the bones (osteolytic metastases), lungs, brain, liver, adrenal glands and contralateral kidney. A single solitary metastasis occurs only rarely. Metastasis of the primary tumour occurs even many years after its removal. Pancreatic metastases are very rare and only anecdotal reports exist in literature.
The authors describe here 2 case reports involving the diagnosis and successful removal of this rare metastasis.
A 67-year old female patient underwent a radical nephrectomy on the right in 1994 for Grawitz tumour. She was followed regularly as part of the surveillance program. The follow-up CT abdominal scan in 2004 accidentally demonstrated a tumour of the pancreas (Figure 1). The patient had no subjective complaints, no weight loss, and no jaundice. Her biochemistry results, including liver enzymes, blood count and tumour markers did not demonstrate any pathological values. The abdominal CT scan described a tumour 3 cm in size at the border between the pancreatic head and body. There were no signs of generalisation to the lymph nodes or liver. In view of her overall condition, age and absence of metastasis, the patient was indicated to undergo elective surgery.
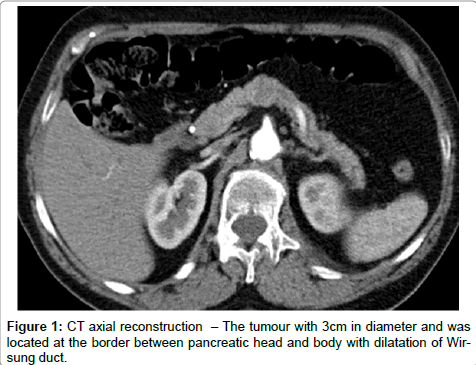
Figure 1: CT axial reconstruction – The tumour with 3cm in diameter and was located at the border between pancreatic head and body with dilatation of Wirsung duct.
During the procedure itself, we first performed a subserous cholecystectomy in view of the presence of cholecystolithiasis. On exploration of the omental bursa, we uncovered the pancreatic tumour described on the CT scan and we verified its relationship with the surrounding structures with using per-operative ultrasound. The tumour was located at the border between the pancreatic head and body, was 3 cm in diameter, well-demarcated, with no signs of extension into the surrounding structures. In view of the tumour´s localisation, we opted for a radical resection procedure involving a duodenum sparing pancreatectomy and splenectomy. The resected section was 13 cm long and its proximal end contained an egg-shaped tumour 3 cm in diameter with a sufficient resection border of healthy tissue. The specimen was fixed and sent for histological examination. The post-operative course was uncomplicated with the patient resuming oral intake. She was discharged on the 11th post-operative day.
The histological examination of the gallbladder demonstrated mild chronic cholecystitis. The spleen showed no pathological changes. The proximal end of the resected 13.4 cm long section of the pancreas contained a tumour 3 x 2.4 x 2.9 cm in size surrounded by a pseudo-capsule. The specimen also contained a further 3 satellite tumour foci 0.6 cm, 1 cm in diameter and 1.2 x 1.2 x 2.5 cm in size. Histologically, all three involved metastases of conventional renal cell carcinoma, grade 2 according to Fuhrman (Figures 2,3,4).
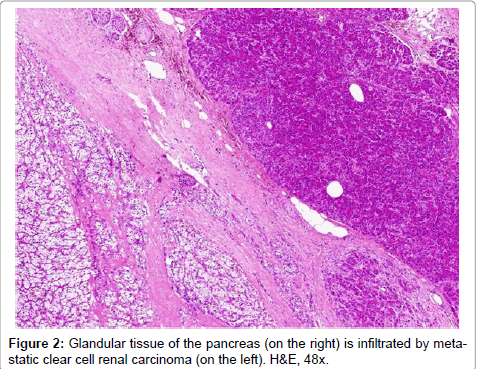
Figure 2: Glandular tissue of the pancreas (on the right) is infiltrated by metastatic clear cell renal carcinoma (on the left). H&E, 48x.
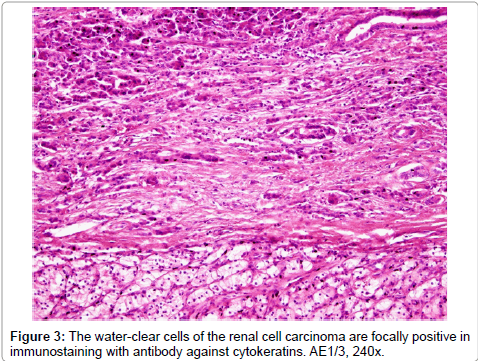
Figure 3: The water-clear cells of the renal cell carcinoma are focally positive in immunostaining with antibody against cytokeratins. AE1/3, 240x.
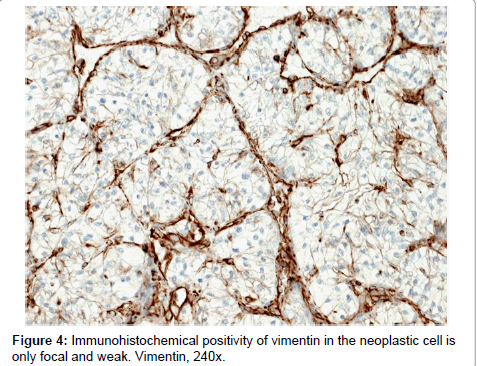
Figure 4: Immunohistochemical positivity of vimentin in the neoplastic cell is only focal and weak. Vimentin, 240x.
The patient is currently 7 years after surgery with no signs of local or distant tumour metastases. Her glycemic profile is physiological and the she shows no signs of diabetes. She is followed regularly by a surgeon and urologist.
A 65-year old female patient underwent a radical nephrectomy on the left in 1994 for Grawitz tumour. She was regularly followed as part of the surveillance program. In 2002, she developed foci in the liver and subsequently underwent segmentectomy of the 6th liver segment. The histology demonstrated the presence of carcinoid. She then underwent ileo-cecal resection for carcinoid. A year later, the followup abdominal CT scan demonstrated a tumour of the pancreas. The patient had no subjective complaints, no weight loss, and no jaundice. Her biochemistry results, including liver enzymes, blood count and tumour markers did not demonstrate any pathological values. The abdominal CT scan described a tumour 6 x 2 x 2 cm in size in the pancreatic tail. There were no signs of generalisation to the lymph nodes or liver. In view of her overall condition, age and absence of metastasis, the patient was indicated to undergo elective surgery.
Infiltration of the pancreatic tail by a tumour mass was uncovered during the procedure. There was no extension into the surrounding tissue and no signs of generalisation. A distal pancreatectomy (Figure 5) with splenectomy was performed.
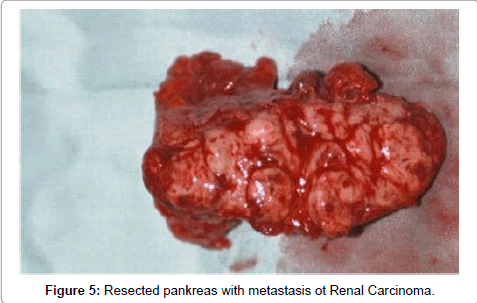
Figure 5: Resected pankreas with metastasis ot Renal Carcinoma.
The post-operative course was complicated by increased drain volume and drain amylase levels, namely 200 ml/24 hours with subsequent spontaneous decrease in this secretion. Oral intake was gradually reinstated and the patient was discharged on the 18th postoperative day. She was re-admitted a week later though with fever. The CT scan demonstrated the presence of a collection of fluid at the site of the distal pancreatectomy, which required subsequent surgical drainage. The patient was discharged after 3 weeks of treatment with an external pancreatic fistula (secreting 50 ml/24 hours). This secretion gradually decreased, ceasing spontaneously after 6 months.
The histological examination demonstrated 2 foci in the 7 cm long resected section of the pancreas. One was spherical, 0.7 cm in diameter, sharply demarcated, greyish-white on cross-section, tough. This was directly connected to the more distal focus of similar appearance, 1.8 x 1.8 x 6.5 cm in size. Both foci involved metastatic infiltration by conventional renal cell carcinoma (Grawitz tumour) grade I according to Fuhrman (Figure 6).
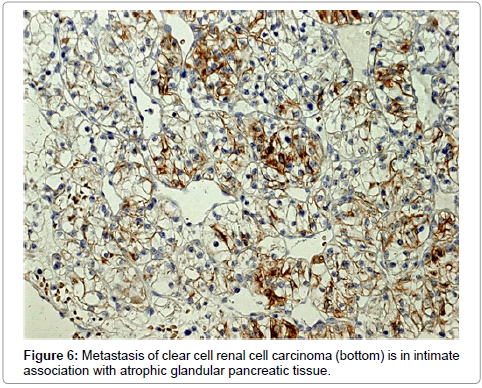
Figure 6: Metastasis of clear cell renal cell carcinoma (bottom) is in intimate association with atrophic glandular pancreatic tissue.
Immunohistochemically, the tumour cells were positive for cytokeratin, vimentin, epithelial membrane antigen and neuron specific enolase. The immunohistochemical testing for the presence of melanocytic markers (S-100, HMB45, melan A), neuroendocrine markers (CD57, chromogranin, synaptofyzin) and pancreatic hormones and enzymes in the tumour cells was negative. The spleen was 14 x 9 x 4 cm in size, of normal macroscopic appearance and did not demonstrate tumour infiltration histologically or any other pathological changes.
The patient is currently 7 years after surgery with no signs of local or distant tumour metastases and no signs of the pancreatic fistula. Her glycemic profile is physiological and she shows no signs of diabetes. She is followed regularly by a surgeon, endocrinologist and urologist.
Pancreatic metastases from renal cell carcinoma represent a relatively rare tumour of the pancreas, namely around 2% of all malignant tumours of the pancreas [1].
In up to 50% of cases, the course is asymptomatic and the tumour is often diagnosed as part of follow-up examinations in patients with prior radical nephrectomy [2]. According to data in literature, there is no difference in incidence between males and females. The primary tumour may be localised either in the right or left kidney and in some cases in both kidneys [2,3].
Pancreatic metastases from renal cell carcinoma have been recorded over the course of 6 months to 27 years following nephrectomy [4], and 11% of these metastases have been described in literature as occurring more than 10 years after the initial radical surgical procedure [5]. These data show that very careful but also very long follow-up and surveillance are necessary. During this period, it is important to pay careful and repeated attention even to minor complaints by patients, especially those involving digestive and respiratory problems- in view of the more frequent lung metastases. Repeated examinations are ä matter of course, especially X-ray examinations of the lungs and abdominal ultrasound. Today, repeated CT scans and tumour marker level monitoring (pyruvate kinase and antibodies against the MUC1 protein) should also be a matter of course [6,7].
Similarly to the diagnosis of primary pancreatic tumours, the diagnosis of pancreatic metastases from renal cell carcinoma is mainly based on non-invasive radiodiagnostic methods– ultrasound, CAT and eventually magnetic resonance imaging in cases of allergy to contrast dyes. Endoscopic ultrasound of the pancreas with fine needle biopsy of foci and subsequent cytological examination is essential for specifying the anatomical conditions and often for determining the precise diagnosis [8].
Surgical intervention aiming for R0 resection is then unequivocally the method of choice [9]. The type of surgical procedure differs according to the localisation of the metastasis. If this is located in the pancreatic tail, then a left-side (distal) hemipancreatectomy with splenectomy is indicated. Spleen-sparing left-side hemipancreatectomy is in these cases considered as unsuitable from the aspect of surgical oncology, in view of the close relationship especially between the splenic vein and pancreatic tissue as well as in view of the lymphatic drainage of this region [6,10,11].
Some authors describe the possibility of implementation of the spleen-saving procedures in the case of pancreatic metastasis of renal cell carcinoma in the pancreas body and tail. Due to the often several years apart from nephrectomy for renal cell carcinoma, it is necessary to always think about the possibility of duplication of tumor and thus the presence of any types of pancreatic cancer. Therefore, in our department we prefer even a suspicion of metastatic disease in the pancreas resection of the pancreas with splenectomy [12].
If the metastasis is located in the pancreatic head, the method of choice involves hemipancreatoduodenectomy, with the findings sometimes requiring a total pancreatectomy. This often depends on the presence of positive resection borders as determined peri-operatively. While some surgeons in the case of positive results opt for re-resection of the pancreas, others opt directly for total pancreatectomy. From the aspect of surgical oncology, both options are possible. From a purely surgical aspect, total pancreatectomy appears to be more suitable in view of the absence of the highly complication prone pancreaticojejunal or pancreatic gastric anastomosis [6,10,11,13].
If the metastasis is located in the pancreatic body, it is possible to perform an extended left-side hemipancreatectomy or a near total duodenum sparing pancreatectomy. Some authors though cite the possibility of resecting the pancreatic body with a pancreaticojejunal anastomosis at the site of the pancreatic tail [6,10,11,14].
In cases of multiple involvement of the pancreas, any of the aforementioned procedures is possible depending on the site of the individual metastases. The most frequent procedures though involve total or near total duodenum sparing pancreatectomy [6,10,11].
Our cases both involved multiple pancreatic metastases diagnosed 10 years following unilateral nephrectomy.
In the first case, we opted for a near total (duodenum sparing) pancreatectomy with splenectomy while in the second we opted for distal pancreatectomy with splenectomy.
According to literature, resectability of such metastases is around 74%. Disease prognosis in this case is significantly more favourable than in the case of patients with primary pancreatic carcinoma [7,10].
Malignant tumours of the pancreas are known to have a very poor prognosis. One exception involves metastases of renal cell carcinoma. Although these tumours are very rare, the possibility should always be kept in mind. The diagnosis is usually not difficult and radical surgery is indicated in all such cases.
The correct diagnosis and radical surgery lead to a favourable prognosis, with five-years survival cited as ranging from 25% to 35% [11]. This is why it is very important for patients who have undergone radical nephrectomy to be followed and surveilled very carefully and for a long time.
This work was supported by the IGA NS9998-4/2008.