Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
ISSN: 2327-4972
Research Article - (2014) Volume 3, Issue 3
Background: Parent-child sexual health communication is a well-documented protective factor against early sexual debut and other sexual risk behaviors. Yet, little is known about communication between single, African American mother-early adolescent son dyads. To address this, a mixed method, qualitative dominant, study design was used to explore the dynamics of sexual health communication between single African-American mothers and their early adolescent sons aged 11-14 years old.
Methods: Mothers and sons, recruited from community health fairs and after-school programs, participated in separate in-depth semi-structured interviews to explore mother-son sexual health communication and sons completed a brief survey about sexual activity.
Results: Mothers and sons expressed both comforts and discomforts with communication. Most mothers and sons reported high connectedness and felt comfortable talking with their sons about sex. Most sons agreed with the content of the sexual health message reported by their mothers, identified their mothers as approachable, and some sons reported that they would talk with their mothers before they started having sex. Mothers report providing a twoprong message to delay sexual debut and use condoms when sexually active and a strong desire to have their son disclose his intentions to sexually debut in order to facilitate sexual health decision-making and provide access to condoms. Findings from this study provide preliminary descriptive data that can be used by providers to facilitate parent-child sexual health communication during early adolescence and prior to a child's sexual debut.
<Keywords: Sexual health communication; Mother-son dyads; Early adolescents
Adolescent males of all race/ethnicities have higher rates of sexual risk behaviors than females. According to a nationally representative sample of high school-aged youth, adolescent males are more likely than females to have had sex before the age of 13 (M=9%, F=3%), had sex with four or more people (M=18%, F=13%), and to have used alcohol or drugs before last sexual intercourse (M=27%, F=18%) (Centers for Disease Control and Prevention [CDC] Youth Risk Behavior Survey, 2011). Additionally, African American (AA) high schoolers are more likely than Hispanics (H) or whites (W) to have ever had sex (AA=60%, H=49%, W=44%), had sex for the first time before the age of 13 (AA=14%, H=7%, W=4%), and had sexual intercourse with more than four people in their lifetime (AA=25%, H=15%, W=13%) (CDC, 2011). An early age of sexual debut is associated with inconsistent or nonuse of contraceptives in later life and is a risk factor for Sexually Transmitted Infections (STIs) and unintended pregnancy [1].
There are several decades of research supporting the protective role of parents in preventing adolescent sexual risk behaviors [2-4]. For example, a positive maternal-son relationship has been shown to predict sexual abstinence in African American adolescents [5] and greater condom use self-efficacy, fewer sexual partners, and less unprotected sex in African American male adolescents [6]. Greater amounts of parent-child sexual communication were associated with fewer sexual risk behaviors, more consistent condom use, and greater intentions to use condoms in the future [6]. Similarly, adolescent males ages 14-16 report that families are their primary source of information about pregnancy, STIs, and condoms [7]. However, parents often underestimate their child’s level of sexual experience; with parents of sexually active teens having more inaccurate reports of a teens’ sexual experience [8].
Though parents play a protective role, not all youth benefit equally. Huebner and Howell (2003) [9], found that minority youth reporting low parent-child communication were more likely to engage in risk behaviors than Caucasians. Studies found that African American adolescents report less parent-child communication about sexual health than whites and African American males are more likely than females to have risk behaviors even when reporting low parent-child communication barriers [10]. Studies suggest that male adolescents are more comfortable talking about sex with their fathers than their mothers and mothers feel more discomfort talking with male versus female children about sex [11,12]. Parents often fail to initiate sexual health communication prior to sexual debut. Beckett et al. found that >40% of youth engage in sexual activity prior to parent-child sexual health communication [13]. Parents report avoiding sexual health communication for fear of not knowing what to say [14], fear the conversation will go badly, not having knowledge, skill or efficacy, situational constraints, and fear communication will encourage sexual activity [15]. Additionally, youth in single-parent households are more likely to engage in risky behaviors [16]. Exploring the comfort, content, frequency, and timing of mother-son sexual health communication is particularly important in African American families since approximately 67% of African American youth live in single-parent households at some point during adolescence [17]. While research about parent-child sexual health communication is quite advanced, exploratory research among African American single mother-son sexual health communication is less developed.
Despite African American adolescent males being a high sexual risk group and more likely to live in single-parent households, few studies were found specifically exploring parent-child sexual health communication between single African American mothers and their early adolescent sons [13,18]. In order to provide contextual information for adolescent sexual health initiatives targeting young adolescent males, we examined sexual health communication between single, African American mothers and their early adolescent sons through in-depth interviews.
We used Hutchinson's et al. theoretical framework that posits how parents influence the sexual health behaviors of adolescents and that highlights determinants of parent-child sexual health communication to develop the research questions and interview guide used in this study [19]. Hutchinson’s framework suggests the importance of beliefs, intention, and knowledge to parent-child sexual health communication, and provides a structure for the interviews conducted separately from mothers and their sons. We devised two overarching research questions from the framework; 1) How do African American mothers and sons describe their conversations about sexual health topics? and 2) What is the level of concordance between reports of sexual health communication between African American mother and sons?
Design
Following the model described by Creswell et al. (2011) [20], we used a mixed methods exploratory study, a dominant qualitative with an embedded quantitative component to address our research questions. Qualitative date was collected on both the mothers and sons and the quantitative survey with conducted with the sons only. We conducted separate analysis of the qualitative and quantitative data and mixed them at the level of inference.
Data collection
One-on-one interviews (averaging 20 minutes) were conducted with sons and mothers, separately, in private areas in community centers and afterschool program locations. Following Seidman (2012) [21], we used a loosely structured, comfortable, and conversational style to conduct our interviews. Questions and probes were used to elicit information about and description of their experience of sexual health communication. Questions proposed during the interview were modified using an iterative process by which participant responses informed interview questions. Prior to interviews, mothers provided demographic data. Sons took a brief survey about sexual behaviors and parent-child communication because of the sensitive nature of asking young adolescents sexual questions in a face-to-face interview format. The 17 question survey took about 10 minutes to complete (Table 1) and was developed after exploring several instruments used in parent-based sexual health interventions [22-24]. The survey was meant to serve as a simplified way of gathering sensitive information from adolescent boys and was not meant for rigorous quantitative analysis.
| Topics | Adolescents | N a |
|---|---|---|
| General sexual health | How many times has your parent ever talked to you about dating or going out with a boy or a girl? | 0=4 1= 12 2=9 |
| How many times has your parent ever talked to you about how your body will change when you grow up or get older? | 0=6 1=8 2=11 |
|
| Waiting until older to have sex | How many times has your parent ever talked to you about waiting to have sex until you are older? | 0=4 1=11 2=10 |
| Waiting until marriage to have sex | How many times has your parent ever talked to you about waiting to have sex until you are married? | 0=8 1=7 2=10 |
| Using protection | How many times has your parent ever talked to you about condoms? | 0=14 1=8 2=3 |
| STI/HIV | How many times has your parent ever talked to you about HIV, AIDS, or other sexually transmitted diseases? | 0=9 1=8 2=8 |
Table 1: Adolescent Survey Results: Perceptions of Parent-Child Communication (Note. 0=We've never talked about it; 1= We've talked about it once or twice; 2= We've talked about it lots of times)
The theory informed interview guide, including questions and probes, was developed and used to conduct 44 individual interviews and two group interviews with brothers (N=48) representing 23 families. Participants received a $25 gift card. Data collection included audio recordings, field notes, and author developed paper/pencil surveys. Two experienced qualitative researchers conducted interviews and coded transcripts. Questions were asked about relationship quality, general communication, and sexual health communication (Table 2). Little new information arose from mothers or sons after 40 interviews were conducted, and data collection was stopped shortly thereafter. University of Texas Institutional Review Board approval was obtained for this study.
| Mother | Son | |
|---|---|---|
| 1. | I am interested in what moms think about adolescent sexual health. Tell me your thoughts. | I am interested in what young guys think about talking with their parents, especially about sex. Tell me your thoughts. |
| 2. | I am interested in what moms think about parent-child communication, particularly about sexual health. Tell me your thoughts. | I am interested in what young guys think about sexual health. Tell me your thoughts. |
| 3. | Describe one conversation you’ve had with your son about sexual health | Describe one talk you’ve had with your mom about sex. Your dad. |
| 4. | What message do you want your son to get from you about sexual health? | What message do you want to get from your mom about sex? How does that compare to what she tells you? |
Table 2: Sample of Questions from Interview Guide
Data analysis
We analyzed the data using a four step process. First, we used methods outlined in Bernard et al. (2010) [25] to conduct a cross case thematic content analysis of mothers and sons together as one data set to look for common themes present in the entire sample. Second, we conducted a concordance analysis between mother and son qualitative data. Third, we used mixed methods to analyze the results of the subgroup survey given to sons and results of the qualitative data at the level of inference. Finally, we developed a conceptual framework to describe the findings of the study (Figure 1).
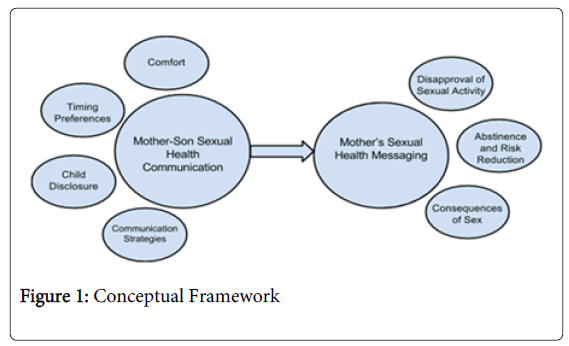
Figure 1: Conceptual Framework
Audio files were transcribed, cross-validated with transcriptions, and cleaned. Mother-son qualitative data were linked to allow a dyadic analysis of themes between mothers and their sons. We used ATLAS.ti (2013, ATLAS.ti Scientific Software Development GmbH) to manage the data and to facilitate the concordance analysis of qualitative themes to examine agreement of reports between mother-son dyads. Data were coded and analyzed by the first author and a second coder trained in qualitative analysis to determine thematic consensus and to mitigate bias. We used consensus building to merge differing interpretations of text. Confirmability of data was verified among the authors using peer debriefing of coding, thematic analysis, exemplars, and supportive quotes to assess the cohesiveness of descriptive interpretations.
Description of the sample
We recruited a community-based voluntary sample of single African American mothers and sons from after-school programs, health fairs, and community organizations in low income areas of a large urban city in south-central Texas. Eligible participants were African American adolescent males ages 11-14 who were English-speaking and resided primarily with their single mother. Sons who lived full-time with their father were excluded. The mother consented and then the adolescent assented for interviews.
The sample included 23 African American mothers and 25 sons ages 11-14 years. Almost all mothers completed high school, had fewer than 3 children, and an income less than $50,000. Only two adolescents reported sexual behaviors and all sons indicated talking with their parent about most sexual health topics once or twice. Sons reported higher communication about waiting to have sex than about condoms in the survey.
Findings
In step one, two main themes emerged from the cross case analysis of mother and son data; mother-son sexual health communication and mothers’ sexual health messages (Figure 1). Sexual health communication encapsulated several subthemes; comfort/discomfort, communication timing preferences, son to mother disclosure, and communication strategies. There are three subthemes related to sexual health messaging; disapproval of adolescent sexual activity, use of a two-prong abstinence and risk reduction message, and discussion of consequences of sex. To protect the identity of participants we have assigned unmatched codes to the dyads such as M1 for “mother 1” and S4 for “son 4” so that M1 and S1 are not necessarily a dyad.
Mother-son sexual health communication
We asked both mothers and sons about what they think about think about adolescent sexual health and parent-child sexual health communication. Participants described both comforts and discomforts, how they timed conversations, the desire for child disclosure, and the strategies used.
Comfort
While many mothers and sons felt comfortable discussing sexual health topics together related to their sense of connectedness, others described apprehensions. Most mothers described themselves as comfortable with communication about their beliefs regarding adolescent sexual activity. They attributed this comfort to a close relationship, “We attached to the hip [sic]. We have a very close relationship” (M23). Sons also said, “I have a very good relationship with my mom and dad. We always talk. She hugs and she loves me” (S12). Other mothers attributed comfort to open communication with their mothers. “My mom taught me that you should be able to talk about any and everything and that’s how I raised my children” (M1).
Discomfort
Some mothers described discomfort with communication related to not knowing what to say and negative communication outcome expectations. “I really didn’t want to talk about it but I have to say something” (M14). “You really don’t know what to say to them about it and I don’t want to say the wrong thing” (M21). While most mothers expressed positive outcome expectations for communicating with their sons, three mothers expressed concern for negative outcomes. “If I tell them, they’re going to want to go and experience it; feeling like the knowledge would be more harmful than helpful” (M2). Some mothers felt adolescents would do what they want regardless of parental communication, “You can let them know that’s not the right thing to do…but if there’s something they want to do, they’ll do it” (M22). Others expressed doubt over their influence on adolescent behaviors “I’m just hoping he listens to my guidance. Kids going to do what they going to do despite what your parents said. I did—I mean, that’s just human nature” (M5).While sons (n=9) indicated that they prefer to receive sexual health education from their mothers, a few sons (n=3) expressed discomfort talking with their mothers about sex. “We don’t talk about it [sex]. It feels kind of awkward” (S5).
Communication timing preferences
Mothers described how they determine when to communicate with their sons when they; 1) exhibit signs of readiness by asking questions, 2) have sexual health-based homework, or 3) show interest in dating.“It’s probably if we see something on TV. I’ll take that moment.” (M23). Sons described when mothers communicate, “While I was driving in the car, she was … telling me about that… like to wait.” (S25). Mothers expressed that they felt compelled to communication during early adolescence, “I know my time is coming to get deep with him.” (M14).
Son to mother disclosure
Mothers unanimously expressed a desire to have sons talk to them before having sex in order to provide a just-in-time message about risk reduction strategies. Mothers wanted to help with decision making, talk about consequences of sex, and take sons to get condoms. They stated, “If you want to have sex, then come to me first. Then we can talk about what steps you’re supposed to take first” (M28). Mothers encouraged sons to tell an adult before having sex. “If you want to have sex, say something. If you don’t say nothing to me, say something to your uncle…your dad…to somebody. Somebody can give you something. I just don’t want nothing to happen to you” (M11). Sons discussed their openness to disclosing information to their mothers. “Because that’s my mom. She gave birth to me, so I can tell her anything” (S1). They described their comfort in talking with their mothers about anything including their sexual activity. “There’s nothing I really can’t like—I don’t feel uncomfortable telling her anything” (S6). Nine mothers discussed how they encourage disclosure and communication. “I want them to know - You can come to me and talk to me. Don’t be afraid that there’s no subject you can’t talk about” (M13).
Strategies
Mothers and sons described the ways they communicate. “Once you get them into the zone, then they’ll start opening up a little bit (M12). Mothers described how they find teachable moments such as TV shows and school work to start the conversation. “If we see something on TV, I’ll take that moment” (M23). Mothers also responded to adolescent behaviors in order to engage in sexual health conversations. “I see him playing with girls sometimes, so I can sit down and talk to him about real life” (M16).
Mothers’ sexual health messages
We asked mothers what message they want their son to get from you about sexual health. We also asked sons what message they want to get from your mom about sex and how that compared to what she told them. Mothers and sons talked about messages of disapproval, used a two-prong message, and discussed consequences of sex.
Disapproval
Twelve of the 23 mothers volunteered responses of overall disapproval of adolescent sexual activity. “They may choose to have sex before marriage. It’s not something that I would advocate for them, but I just have to deal with it” (M4). However, seven mothers described beliefs that adolescent sexual activity is normal and expected. “My belief is sex when you’re married. But I know it don’t happen that way” (M1). Mothers expressed conflicting feelings, a desire for sons to wait until marriage for sex and the belief that their sons would have sex prior to marriage. “I want them to wait until they’re married but that’s not a reality right now” (M13).
Two-prong message
Mothers discussed the importance of getting a good education and establishing healthy relationships. Mothers (n=16) responded to the belief that their sons would have sex despite their desire for them to wait by having a two-prong message that; 1) promoted delaying sexual debut until the child was “older” or married and 2) provided a strong risk reduction message encouraging the use of condoms. “You need to start when you turn 19 years old and he need to use protection at all times” (M3).
Consequences
Mothers most often promoted delayed sexual debut and condom use by discussing the consequences of sexual activity. “I show him pictures of what can happen” (M24). Additionally, sons discussed how becoming a teen parent can negatively impact future plans. “If you have a baby… that might make it [college] hard” (S22). Mothers also stressed the impact of sexual activity on the formation of healthy relationships. They noted that youth should focus on their education rather than sex. Finally, mothers described how they clearly expressed their expectation for sons to delay sexual debut.
Concordance
In step two, we conducted a concordance analysis between mother and son qualitative data. While most mother-son dyads felt comfortable communicating, two sons who expressed discomfort communicating had mothers who also reported feeling uncomfortable. Six mothers believed their sons would tell them when they were going to have sex. “He will tell me because he tells me everything” (M1) while only nine sons reported that they would tell their mothers, with only three sons of the six mothersThere were high levels of agreement between mothers and sons regarding the sexual health message with three fourths of the dyads reporting the same messages being given (mother) and received (son). “She told me wait until I get older, and always use a condom so you won’t catch anything” (S28). “We talk about it a lot, about how you should wait to find a good woman who is right with God….and should wait till after you get married. And if you do it before you get married, wear a condom” (S15).
Survey results
In step three, we used mixed methods to analyze the results of the subgroup survey (Table 1) given to sons and results of the qualitative data at the level of inference. We found discrepancies in sons’ reports of communication. Five mother and son dyads indicated during the interview that they had not started talking about sexual health. However, in the survey, all 25 sons indicated some level of conversation with their parents regarding sexual health topics. While all sons reported during interviews that their mothers had talked to them about waiting, 10 sons reported on their survey that they had never talked with their parent about waiting to have sex until they were older or married. Seven mothers reported not discussing a risk reduction message. While 18 sons indicated during the interview that they had received a message to use condoms, 12 sons indicated on the survey that they had never talked about condoms. Only five sons reported on both the survey and in the interview that they had never talked about condoms with their parents. Finally, sons of mothers who expressed communication discomfort had lower communication scores across all items (Mean = 3.67 vs. Median= 5.17, range = 0-10).
Findings from this study provide insight into sexual health communication in African American mother-early adolescent son dyads. In general, single mothers provided a high level of sexual health communication that included messages about waiting to have sex and using condoms. Most mothers express comfort related to communicating with their son about sexual health and express positive attitudes toward communication. Similarly, Guilamo-Ramos et al. (2008) [15] found that maternal self-efficacy and positive emotions related to communication predicted the frequency of mother-reported communication in minority mother-child dyads. Those dyads that expressed discomfort reported more difficulty in maintaining open communication, a perception of maternal approachability, and struggled with the content, context, and receipt of sexual health messages.
In a survey conducted with 394 parent/child dyads, Evans et al. (2012) [26] found that only 33% of sons ages 10-14 years agreed with their mother’s reports of mother-son sexual communication. In contrast, this study found surprisingly high mother-son concordance in reports of sexual health messages with most sons (n=18) agreeing with their mothers’ reports on the sexual health message. This may be due to the high level of connectedness reported by the mothers related to being a single parent and is an important protective factor with agreement positively associated with sexual abstinence and condom use [27].
Though agreement between themes from mothers and sons was high, there were discrepancies in reports from the sons between the survey and interview. It is possible that mothers and sons narrowly conceptualized sex communication. They may not have considered conversations about dating or waiting to be “sexual health communication”. It is also possible that the interview process facilitated recall of conversations. This highlights the advantage of incorporating both interview and survey methods.
Many sons reported perceived maternal disapproval of sex, similar to findings in a nationally representative sample using Add Health data; 90% of youth reported perceived maternal disapproval of sex [28]. However, we found that most sons reported perceived maternal approval and endorsment of condom use. Khurana and Cooksey (2012) [28] found only 50% of sons reported perceived maternal approval of contraceptive use.
While mothers of early adolescent boys express disapproval of early sexual activity, they also provide supportive risk reduction messages about condom use in anticipation of sexual debut. We found that approximately 88% of sons reported receiving a risk reduction message. Teens who discuss condoms with their parent are more likely to report condom use at last sex in both community and high-risk youth samples [29].
An interesting finding of this study is that mothers who expressed high communication comfort and positive outcome expectations often cited maternal and female family members who role modeled open communication. This highlights the potential for exponential intergenerational change in social norms supporting parent-child sexual health communication in interventions targeting parental behavior change. Those who expressed discomfort or negative outcome expectations for sexual health communication had sons who reported less frequent and less extensive communication.
Another interesting finding was the strong desire for disclosure of sexual intentions prior to sexual initiation. Limited research has been conducted to examine the influence of disclosure on sexual behaviors and condom/contraceptive use. This could be a critical just-in-time moment in the trajectory of adolescent sexual health behaviors and outcomes and warrants further research. Additionally, it is important to explore the influence of family dynamics, parent-child relationships, and communication patterns on child disclosure of intentions to become sexually active. This study points to child disclosure of intentions to sexually debut and parental response as potentially influential on decision making, access to condoms and contraceptives, and ultimately on sexual behaviors.
There are several limitations to this study. Our study population, limited to a volunteer sample from afterschool programs to minimize heterogeneity, may represent highly engaged, less at-risk dyads. While this study provides insightful information for this subgroup, these qualitative findings cannot be generalized; however, the findings can be applied to other groups or settings. The survey, author developed and not psychometrically tested, and interview questions may have led participants to express their thoughts and feelings in a socially desirable way. While the interviews were fairly short, this is not unexpected as we were working with adolescent boys and asking about sensitive topics. Despite the compact nature of the interviews, we gleaned a plethora of information to move the science forward. Finally, there was racial discordance between interviewer and participant in some of the interviews and gender discordance between the sons and female interviewers that may have influenced participant comfort and disclosure though initial non-threatening questions were used to increase participant comfort. Expansion of this study to other racial and ethnic groups, family structures, and age groups, and recruitment locations is needed. Further quantitative studies are needed to determine associations between communication, relationship quality, child disclosure, and adolescent sexual activity.
We explored sexual health communication in single African American mother-son dyads. Many mothers felt comfortable communicating with sons and provided a two-prong message to delay sexual debut and use condoms when sexually active. Sons described feeling close to their mothers and expressed confidence in discussing sexual health questions. Mothers and sons had high sexual health message concordance. The unique implications of mother-son sexual health communication warrant greater research particularly in relation to sexual activity disclosure and cultural communication and their influence on sexual health communication. Additionally, further research is needed to explore how sexual health messaging differs across race/ethnicity and by gender of the parent and child. Finally, research between fathers and sons is limited.
Findings from this study should be considered and may be applicable in the clinical and public health setting by healthcare providers working with adolescents and families. Health care providers play an essential role in counseling parents on becoming sexual health educators and developing parent-based adolescent sexual health interventions to expand support for mother-son sexual health communication. Our findings indicate that sons prefer to receive sexual health education from their mothers, similar to other studies [30] and those mothers felt comfortable assuming the role of sexual health educator, even between mothers and sons. This underscores the need to provide mothers with the knowledge and skills to be primary sexual health educators. Studies have shown that with counseling, parents can be as effective as professional sexual health educators in improving adolescent sexual health outcomes [3]. Parents, particularly mothers, are often the first to provide sex education. Parents can tailor the message to their personal values and beliefs [31]. About one third of adolescents in this study reported intentions to go to their mother prior to becoming sexually active. Encouraging parents and children to establish and maintain protective communication and monitoring practices throughout adolescence is a crucial way nurses can positively impact adolescent sexual health outcomes.