Medical & Surgical Urology
Open Access
ISSN: 2168-9857
ISSN: 2168-9857
Research Article - (2018) Volume 7, Issue 4
Objective: To demonstrate and quantify the immune response changes over time in patients with Non-muscleinvasive Bladder Cancer (NMIBC) treated with bacillus Calmette-Guerin (BCG).
Methods: The study enrolled 52 patients. Group A included 32 patients with high risk and intermediate risk NMIBC treated with TURBT and intravesical BCG. Group B included 20 patients underwent cystoscopy for other indications. Monitoring immune changes was done by quantifying the percentage of T lymphocytes in urine samples taken before BCG therapy, immediately after BCG therapy and 3 months later. Patients in Group A were followed for 1 year and the clinical outcome was correlated to the level of the immune response.
Results: In the initial urine samples taken before BCG therapy the mean flowcytometeric percentages of the T lymphocytes were comparable in both groups. Six weeks after BCG therapy, Group A revealed a significantly elevated mean flowcytometeric measurement 53.3% which dropped after 3 months to 22.4% but still significantly more than that of Group B (which did not show a significant rise after 6 weeks and after 3 months). Out of the 32 patients in Group A, 25 patients (78%) revealed significantly elevated flowcytometeric measurements after BCG therapy in comparison to the mean percentage of the control group (strong responders), while 7 patients (22%) revealed minimally elevated measurements (weak responders). Three cases from the strong responders group (12%) had tumor recurrence during follow up period compared to 3 cases (43%) from the weak responders.
Conclusion: Flowcytometery is a feasible method for monitoring the BCG immune response by measuring the percentage of T lymphocytes in urine.
Keywords: Bladder cancer; Intravesical BCG; Flowcytometry
Till now the exact tumoricidal mechanism of BCG is not fully understood. Several efforts have been made to understand the immunological mechanisms involved. It is generally accepted that BCG induces an acute inflammatory response, during which there is various cytokines released, with lymphocytic and natural killer cell aggregation in the bladder wall. Urine analysis revealed elevated levels of interleukins and lymphocyturia, after BCG instillation.
Currently there is no well demonstrated predictive factor to evaluate the response to BCG therapy. Many studies reported different parameters of prognostic value for BCG immune response. Saint et al. [1] analyzed more than fifty studies published in the literature which assessed various parameters as prognostic markers for BCG immune response. They concluded that the cellular response criteria are the critical determinant of post-BCG outcome. The role of T lymphocytes notably the CD4+ cells was demonstrated in many studies as the most effective cells induced in response to intravesical BCG instillation having a central role in the antitumor mechanism of BCG [2-5].
Several authors tried various techniques to detect T lymphocytes as a marker for BCG immune response. Saint et al. [6] detected leukocytes in the urine after BCG instillation by conventional cytology. Other investigators used special stains or immunohistochemical studies to detect T cells in the bladder wall after BCG therapy [7-9]. Boer et al. demonstrated T lymphocytes in the urine of patients treated with BCG using flowcytometeric analysis. Flowcytometry is a technique for counting, examining and sorting microscopic particles suspended in a stream of fluid [10]. Flowcytometer measures the properties of light emission properties from fluorescently labeled monoclonal antibodies bound to the surface of the cells as they pass through a laser beam [11]. The light scattering properties of cells are related to their size and intracellular contents. This technique is more accurate than other techniques and allows computerized quantization of the amount of T lymphocytes in the urine before and after intravesical BCG instillation and hence we can demonstrate the magnitude of the immune response.
The aim of the current study is to measure the magnitude of the immune response and to demonstrate the immune response changes over time in patients treated with intravesical BCG instillations. This will allow early identification of those who will benefit from this therapy and those who will not benefit so that they can be offered another treatment option. T lymphocytes were used as markers for the immune response and flowcytometery was the technique used for counting these cells in the urine.
This study was conducted upon 52 patients, divided into 2 groups. Group A (the study group) included 32 patients (27 men and 5 women, age range 30-75 years, mean age 57 years) with high risk and intermediate risk NMIBC who were candidate for BCG therapy following bladder tumor resection presenting for the first time, excluding patients who had received previous intravesical therapy, patients with residual unresectable bladder tumors, patients with massive heamaturia after BCG instillation, patients with persistent fever more than 48 hours after BCG instillation, patients with recurrent urinary tract infection and patients on immunosuppressive drugs [5,6]. Group B (control group) included 20 patients who had underwent cystoscopic manipulations other than bladder tumor resection including seven patients who underwent transurethral resection of the prostate, five patients who underwent bladder stone extraction, and eight patients who underwent endovisual urethrotomy. Institutional review board approval was obtained before undertaking the study, and informed consent was signed by all enrolled patients [1].
In Group A, three weeks after tumor resection, all patients received six weekly doses of BCG. Voided urine samples were collected for flowcytometeric analysis to quantify the percentage of T lymphocytes. Samples were taken before BCG therapy, after the sixth dose of BCG and 3 months later. All patients in Group B were subjected to urine sampling for flowcytometery. Samples were collected at the same timing as Group A. Urine culture was done regularly before urine sampling to exclude infection. Group A underwent follow up cystoscopies every 3 months for the first year and maintenance BCG therapy as indicated.
Flowcytometery technique
A morning urine sample was collected from each patient in a test tube. Mononuclear cells were isolated by centrifugation at 2000 rpm for 5 minutes, and then washed by phosphate-buffered saline (PBS) at pH 7.2. Heamolysis of red blood cells was done by adding FACS lysing solution. 100 μl of the suspended cells were mixed with 10 μl fluorescein-labeled T cell antibody using commercial kit (FITCconjugated monoclonal mouse anti-human T cell by DAKO) and then incubated in the dark at 4°C for 30 minutes [2,10]. The mixture was then washed twice with PBS and 2% bovine serum albumin. The sample was then passed through a flowcytometer (Becton-Dickinson FacsCalibur). Data was analyzed by a computer and presented it in the form of histogram. The percentage of T-lymphocytes present in the urine samples was measured and recorded as a marker for the magnitude of the immune response.
The percentage of the T lymphocytes in the urine in Group A (32 patients) was measured by flowcytometery before and after BCG therapy and the mean results were compared to those in Group B (20 patients). In the initial samples taken 3 weeks following the TURT in Group A (before BCG therapy) and 3 weeks following the cystoscopic procedures in Group B, the mean flowcytometeric percentages of the T lymphocytes were comparable, 8.8% and 8.6% respectively (Table 1).
| Before BCG | At 6 weeks | At 3 months | ||
|---|---|---|---|---|
| Group A | Mean(%) ± SD | 8.8 ± 3.32 | 53.3 ± 27.95 | 22.4 ± 18.18 |
| Group B (control) | Mean(%) ± SD | 8.60 ± 3.13 | 9 ± 3.02 | 6.35 ± 2.25 |
Table 1: Comparison between Group A (study group) and Group B (control group) according to the mean flowcytometric percentage of Tlymphocytes measured before intravesical BCG, at 6 weeks and at 3 months following intravesical BCG.
After six weeks of BCG therapy Group A revealed a significantly elevated mean flowcytometeric measurement 53.3% which dropped evidently after 3 months to 22.4% but still significantly more than that of Group B (which did not show a significant rise after 6 weeks and after 3 months, 9% and 6.3% respectively). After 6 months both groups revealed comparable measurements 13.5% and 8.9% respectively (Figure 1).
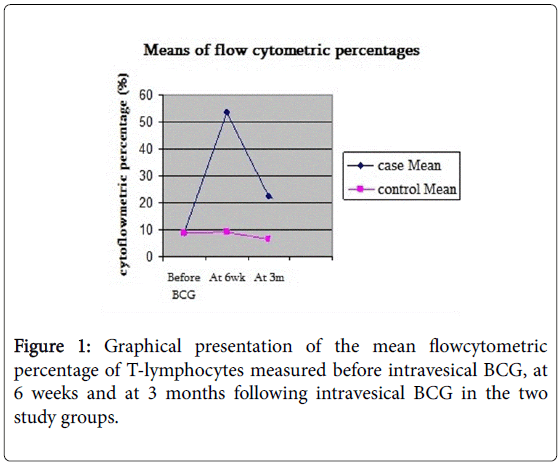
Figure 1: Graphical presentation of the mean flowcytometric percentage of T-lymphocytes measured before intravesical BCG, at 6 weeks and at 3 months following intravesical BCG in the two study groups.
Not all the patients in Group A did show a significant rise in the percentage of T lymphocytes after BCG therapy. Out of the 32 patients in Group A, 25 patients (78%) revealed significantly elevated flowcytometeric measurements after BCG therapy in comparison to the mean percentage of the control group (strong responders), while 7 patients in Group A (22%) revealed minimally elevated measurements after BCG therapy, which were comparable to the mean percentage of the control group (weak responders) (Table 2).
| After BCG therapy | After 3 months | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Max | Min | Mean | SD | Max | Min | |
| Strong responders (No:25) | 65.16 | 18.7 | 88 | 25 | 25.52 | 19.4 | 75 | 4 |
| Weak responders (No:7) | 11.28 | 3.63 | 15 | 4 | 11.14 | 2.2 | 15 | 9 |
| Control (No:20) | 9 | 3.02 | 15 | 4 | 6.35 | 2.25 | 12 | 3 |
No: Number; Min: Minimum; Max: Maximum; SD: Standard Deviation
Table 2: Comparison between the strong and weak responders of group A and the control group B according to the mean flowcytometric
All patients in Group A were followed up every 3 months for 1 year to detect tumor recurrence and all were given maintenance BCG as indicated. Out of the 32 patients in Group A, 26 patients (81%) were free during the follow up period, while 6 patients (19%) presented with tumor recurrence. The incidence of tumor recurrence was correlated with the immune response changes and it was found that out of the 25 strong responders 3 cases (12%) presented with tumor recurrence in the follow up period, while among the 7 weak responders, 3 cases (43%) presented with tumor recurrence (Figure 2). All recurrent cases received second course BCG therapy.
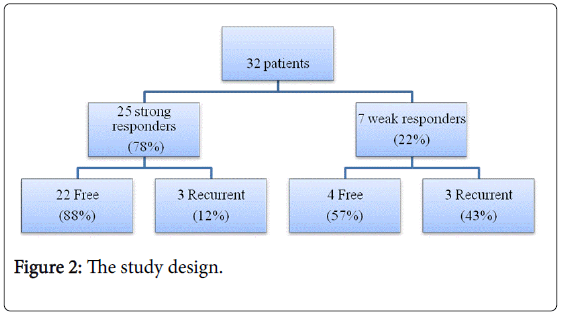
Figure 2: The study design.
Two cases from the strong responders group remained free for 9 months follow up after the second course, while the third case lost to follow up. Two cases from the weak responders group presented with tumor recurrence after 3 and 6 months from the second course and were managed by cystectomy, and the other case was free for 6 months follow up.
BCG has become an established adjuvant therapy for high and intermediate risk patients with NMIBC. However many patients may suffer from variable degrees of BCG toxicity and others may fail to respond to BCG therapy and are at risk of disease progression. So it is important to establish a protocol for BCG administration that provides maximal anti-tumor effect with least toxicity. At the same time it would be of great value to have tools that early predict those who fail to respond to BCG therapy so that they may have a better chance with another intravesical therapy or even cystectomy.
Several clinical trials were carried out trying to modify the protocol of administration of BCG. These trials involved many aspects of BCG therapy including the dose of BCG, the schedule of BCG therapy, BCG maintenance, detecting BCG failures…etc. The results of these trials usually came out with recommendations that did not differentiate between the relative response of each patient to BCG, assuming that all patients respond to BCG in the same manner, and the design of the BCG therapy was usually entailing the “wait and see” concept. We believe that all these aspects of BCG therapy should be individualized according to the patient's response to BCG. Monitoring the immune response after BCG instillation will help tailoring the therapy according to each individual patient. To monitor the immune response we have to select an immune parameter that represents the status and magnitude of the immune response. T lymphocytes proved to be a suitable immune parameter for monitoring the BCG immune response and it was measured by flowcytometeric analysis of urine samples from patients and control.
By analyzing the mean flowcytometeric measurements before and after BCG therapy among Group A and Group B, there was no statistically significant difference between both groups in the measurements before BCG therapy having a mean measurement of 8.8% and 8.6% among both groups respectively. After BCG therapy there was a significant increase in the mean percentage of the T lymphocytes among Group A rising up to 53.3% while the control Group B remained 9% and the difference was statistically significant. This denotes a pronounced immune response under the effect of BCG, supporting the vital role of T lymphocytes in the antitumor effect of BCG and highlighting its value as a predictive marker for post-BCG immune response. Three months following BCG therapy there was a drop in the mean flowcytometeric measurement to 22.4% among Group A reflecting the waning process of the immune response. This finding supports in an objective way the need for maintenance BCG dosage at 3 months follow up, and is in accordance with many clinical trials which recommend maintenance BCG dosage at 3 months follow up.
By analyzing the flowcytometeric measurements among Group A who received BCG therapy we can divide the 32 patients into two subgroups. Strong responders group including 25 patients (78%) who showed elevated flowcytometeric measurements in comparison with the mean measurement of the control group reflecting favorable immune response, and weak responders group including 7 patients (22%) with minimally elevated measurements which were comparable with the mean measurement of the control group reflecting poor immune response. There was a positive correlation between the level of the immune response and the clinical outcome where only 3 recurrent cases were from the strong responders group with favorable immune response (12%) and 3 recurrent cases were from the weak responders group with poor immune response (43%).
All recurrent cases received second course BCG therapy. Two of the recurrent cases from the strong responders subgroup remained free for 9 months follow up after the second course. On the contrary, two cases from the weak responders subgroup presented with tumor recurrence at 3 and 6 months from the second course and were managed by cystectomy. The results of the present study highlight an important issue regarding the correlation between the immune response and the clinical response. Patients with initial strong immune response to BCG therapy who present with tumor recurrence may benefit from another course of BCG. Those with poor immune response and presented with tumor recurrence may have a better chance with another intravesical therapy or even early cystectomy. This issue has to be studied on a larger scale of patients and longer follow up period.
It can be suggested that the immune response to BCG can be our guide in the coming era to adjust the BCG treatment aiming for the best outcome. More research should be directed to this field to reach the optimal management for each individual patient receiving BCG therapy.
Flowcytometery is a feasible clinical method for monitoring the BCG immune response by measuring the percentage of T lymphocytes in urine; accordingly we can tailor the treatment on individual basis. The limitations of the current study are; small number of patients, lack of long term follows up and lack of a cut off values for the flowcytometric percentage of the lymphocyte response. More research is needed in this field to customize tools for the optimal regimen.