Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
ISSN: 2329-8790
Research Article - (2014) Volume 2, Issue 1
Background: Anemia impairs cognitive development, reduces physical work capacity and in severe cases increases risk of mortality particularly during prenatal period. There are no previous studies done on anemia in pregnancy in the study area.
Objective: To assess the prevalence and determinant factors of anemia among pregnant women attending antenatal care follow up at Tikur Anbessa specialized hospital.
Methods: Health institutional based cross-sectional study design was conducted from November 23, 2013 - March8, 2013 among 395 pregnant mothers who had been attending antenatal care. Blood sample was taken to determine the hemoglobin concentration and haematocrit value. Interviewer administered structured questionnaire was used to assess different socio-demographic characteristics, obstetrics and dietary factors related to anaemia. Simple random sampling technique was used to select study subjects. Data were entered with EPI info version 3.5.1 Cleaning and analysis was done using SPSS version 17 and statistical tests were performed at the level of significance of 5%.
Result: The overall prevalence of anemia in this study using a cut off level of hemoglobin <11 g/dl (<33% haematocrit) was 21.3% (84/395). Out of 84 anemic pregnant mothers, 80.95% (68/84) were mildly anemic, 17.86% (15/84) were moderately anemic and 1.19% (1/84) were severely anemic. The following variables were significantly associated with anemia: Age (39-45 yrs (AOR=1.21)), education status (illiterate (AOR=2.12)), family size (greater than four (AOR=2.04), gestational age (third trimester (AOR=2.04)), birth intervals (less than two years (AOR=1.21)), history of blood loss (AOR=1.67)), antenatal care (no ANC (AOR=1.11)), contraception (no contraception (AOR=2.31)), gravidity (multigravid (AOR=1.22)), parity (multiparous (AOR=2.19)).
Conclusion: The present study showed high prevalence of anemia and the majority of them were of the mild type (hemoglobin: 10-10.9 g/dl).
Keywords: Anemia; Pregnancy; Prevalence; Hemoglobin
Anemia refers to a condition in which the hemoglobin content of the blood is lower than normal for a person´s age, gender and environment, resulting in the oxygen carrying capacity of the blood being reduced [1,2]. The mean minimum acceptable hemoglobin level during pregnancy by WHO criteria is taken to be 11 g/dL [2]. WHO further divides anemia in pregnancy into: mild anemia (hemoglobin 10-10.9 g/dL), moderate anemia (hemoglobin7.0-9.9 g/dL) and severe anemia (hemoglobin <7 g/dL [2]. It is a global health problem affecting both developing and developed countries with major adverse effects on human health as well as social and economic development [1-5]. In 1993, WHO ranked anemia as the 8th leading cause of disease in girls and women in the developing world [2]. Estimates from the World Health Organization report that 35% to 75% of pregnant women in developing countries, and 18% in developed countries are anemic [2]. The greatest burden of anemia is born by Asia and Africa where it is estimated that 60% and 52% of pregnant women, respectively, are anemic and between 1% and 5% are severely anemic (hemoglobin <7 g/dl) and is associated with women of age less than 20years, third trimester of pregnancy, rural residents, and multiparous women [6,7]. United Nations expert panel considered severe anemia an associated cause in up to half of the maternal deaths worldwide [8]. Estimates of maternal mortality resulting from anemia range from 34/100,000 live births in Nigeria to as high as 194/100,000 in Pakistan [6,7]. In sub-Saharan Africa it is estimated that 20% of maternal deaths are associated with anemia [2].
In developing countries, the cause of anemia during pregnancy is multi-factorial and includes nutritional deficiencies of iron, folate, and vitamin B12 and also parasitic diseases, such as malaria and hookworm. The relative contribution of each of these factors to anemia during pregnancy varies greatly by geographical location, season, and dietary practice. In sub-Saharan Africa, iron and folate deficiencies are the most common causes of anemia in pregnant women [1,9]. Vitamin B12 deficiency may be an unrecognized contributor to anemia in this region of the world due to reliance of the population on grains as dietary staples and low consumption of foods of animal origin which are the primary source of dietary vitamin B12 [9].
Although Ethiopia has different climatic conditions and grows a variety of cereals, root crops and vegetables, some of these are not fully utilized [10,11]. There appears to be dependency on a single food crop by region although the specific crop varies in the different regions [10]. The staple crops consumed in the North and Central part of Ethiopia are teff and cereals; in the South and Southwest staple crops are enset, maize, cereals and root crops; and in the East staple crops are sorghum and maize [10]. The lack of dietary diversity results in a shortage of minerals and vitamins which suggests that the bio-availability of much of the iron in the average Ethiopian diet is restricted and this restriction may have affected the iron status [10]. The present study was designed to see the hemoglobin levels in pregnant women at Tikur Anbesa specialize hospital. The results of this study will help to motivate ante natal care providers towards early detection and management of anemia in pregnancy
A cross-sectional study design was conducted at Tikur Anbessa Specialized Hospital from November 23, 2012- March8, 2013. Source population were all pregnant women who live in Addis Ababa and study population were pregnant women attending antenatal care at Tikur Ambessa specialized hospital, Addis Ababa Ethiopia and study subjects were pregnant women attending antenatal care during the study period and who met the inclusion criteria. A total of 395 pregnant mothers were enrolled in this study.
Sampling
The required sample size for this study was calculated using formula for single population proportion based on the prevalence rate of 62.7% reported from the previous study and using the 95% confidence interval and 5% marginal error. By adding 10% for none response the final sample size will be 395.
The study participants were selected based on the inclusion and exclusion criteria by using simple random sampling method. Exclusion criteria were pregnant women who were severely sick due to other medical conditions and those who were on treatment for anemia.
Inclusion criteria
In this study, pregnant mothers who were residents of Addis Ababa, not recently transfused, who had no chronic medical diseases, no diagnosed haemoglobinopathies, and who had no early bleeding or antepartum hemorrhage were included.
Data collection
A structured and interviewer administered questionnaire was used to collect data on the socio-demographic variables, dietary habit, and obstetric factors. The questionnaire of this study was developed from the Ethiopian Demographic and Health Survey (EDHS) guide lines which essentially contains the same information of the WHO guide lines. Data was collected by midwives of the hospital. Venous blood was collected to determine haemoglobin concentration after an informed consent is obtained from the study subjects.
Data analysis
Data were entered with EPI info version 3.5.1. Analysis was done by using SPSS version 17. Mean frequency and p-value has been calculated. After multivariate logistic regression analysis was used variables significant at the p value<0.05 are kept in the final model
Ethical considerations
Ethical approval and clearance was taken from institutional review board of College of Health Sciences, Addis Ababa University and permission letter for data and sample collection has also been received from the Department of Obstetrics and gynecology. Data and blood sample collection was started after written informed consent was obtained and after the objectives, benefits and risks of the study were explained to the study participants. Participation in the study was voluntary, and refusal to participate involved no loss of benefits to which the mothers were otherwise entitled. Study participants had the right to accept or refuse participation in the study at any time.
Socio-demographic characteristics of study subjects
Total of 395 informed and consented pregnant women who came for their antenatal follow up were enrolled in this study and all were urban dwellers. The mean age of the attendants was 28.8 years old (range from 18-46). Majority of the study groups were in the age range of 25-31 years. Many of the respondents were married 380 (96.6%). One hundred ninety two (48.6%) of the respondents were housewife and 27 (6.8%) were merchants. Forty percent of the respondents had educational status of 9-12 grade and 122 (30.9%) had diploma/degree. One hundred twenty seven of the respondents did not know their income and 125(31.6%) had an average income. Two hundred fifteen (54.4%) respondents had family size of greater than four (Table 1).
| Variables | Frequency(n) | Percentage (%) | |
| Age | 18-24 | 71 | 17.97 |
| 25-31 | 182 | 46.1 | |
| 32-38 | 108 | 27.3 | |
| 39-45 | 31 | 7.8 | |
| >45 | 3 | 0.8 | |
| Ethnicity | Amhara | 179 | 45.3 |
| Oromo | 96 | 24.3 | |
| Tigre | 40 | 10.1 | |
| Gurage | 52 | 13.2 | |
| Others | 28 | 7.1 | |
| Religion | Orthodox | 285 | 72.2 |
| Muslim | 65 | 16.5 | |
| Protestant | 39 | 9.9 | |
| others | 6 | 1.5 | |
| Marital status | Married | 380 | 96.2 |
| Single | 8 | 2 | |
| Divorced | 5 | 1.3 | |
| Widowed | 2 | 0.5 | |
| Occupation | House wife | 192 | 48.6 |
| Civil servant | 89 | 22.5 | |
| Merchant | 27 | 6.8 | |
| others | 87 | 22 | |
| Education status | Illiterate | 20 | 5.1 |
| Read and write | 14 | 3.5 | |
| 1-8 grade | 81 | 20.5 | |
| 9-12 grade | 158 | 40 | |
| Diploma/degree | 122 | 30.9 | |
| Income | < 230 ETB | 1 | 0.3 |
| 231-850ETB | 55 | 13.9 | |
| 851-2350ETB | 125 | 31.6 | |
| >2350ETB | 87 | 22 | |
| I don’t know | 127 | 32.2 | |
| Family size | <=4 | 108 | 45.6 |
| >4 | 215 | 54.4 | |
Table 1: Socio demographic characteristics of pregnant women attending antenatal care at Tikur Anbessa Specialized Hospital from November 23, 2012 - March 8, 2013.
Prevalence and severity of anemia
The overall prevalence of anemia using a cut off level of hemoglobin <11 g/dl (<33% haematocrit) was 21.3% (84/395). The mean haematocrit value was 0.36 (36%), ranging from 19-45%. Out of all anemic pregnant women about 80.95% (68/84) were mildly anemic, 17.86% (15/84) were moderately anemic and 1.19% (1/84) were severely anemic (Figure 1).
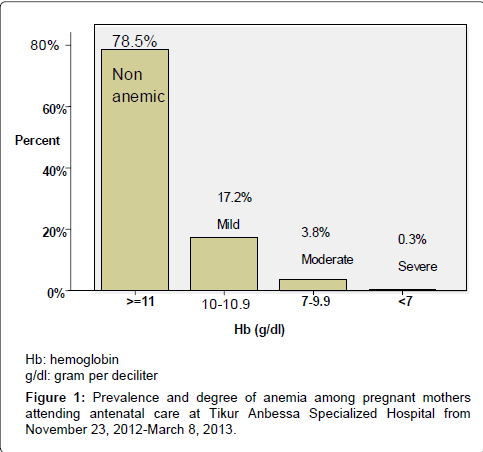
Figure 1: Prevalence and degree of anemia among pregnant mothers attending antenatal care at Tikur Anbessa Specialized Hospital from November 23, 2012-March 8, 2013.
Anemia and socio-demographic characteristics
About 41.9%, 33.3%, 32.4% of the pregnant women who were in the age range of 39-45, >45 and 32-38 years were anemic respectively. Forty percent of anemic pregnant women were divorced and 21.3% were married. Forty five percent (45%) and 31.6% of anemic pregnant women were illiterate and had family size of greater than four respectively (Table 2).
| Characteristics | Anemic (N=84) | Non anemic (N=311) | Total | AOR(95%CI) | P-value | |
| age | 18-24 | 4 (4.8) | 67 (21.5) | 71 | 1 | |
| 25-31 | 31(36.9) | 151(48.6) | 182 | 0.75(0.84,9.12) | 0.81 | |
| 32-38 | 35 (41.7) | 73 (23.5) | 108 | 0.23(0.43,2.14) | 0.51 | |
| 39-45 | 13 (15.5) | 18 (5.8) | 31 | 1.21(1.93,11.1) | 0.033 | |
| >45 | 1 (11.9) | 2 (0.6) | 3 | 2.12(0.65,1.34) | 0.81 | |
| Ethnicity | Amhara | 41(48.8) | 138 (44.4) | 179 | 1 | |
| Oromo | 20 (23.8) | 76 (24.4) | 96 | 1.3(0.56,2.76) | 0.588 | |
| Tigre | 11(13.1) | 29 (9.3) | 40 | 0.97(0.35,2.67) | 0.946 | |
| Gurage | 7 (83.3) | 45 (14.5) | 52 | 0.57(0.198,1.6) | 0.286 | |
| others | 5 (59.5) | 23 (7.4) | 28 | 0.54(0.15,1.97) | 0.352 | |
| Religion | Orthodox | 64 (76.2) | 221 (71.1) | 285 | 1 | |
| Muslim | 15 (17.9) | 50 (16.1) | 65 | 0.76(0.33,1.8) | 0.521 | |
| Protestant | 4 (4.8) | 35 (11.3) | 39 | 0.74(0.21,2.6) | 0.641 | |
| Others | 1(1.2) | 5 (1.6) | 6 | 1.78(0.16,2.2) | 0.64 | |
| Marital status | Married | 81(96.4) | 299 (96.1) | 380 | 1 | |
| Single | 1(1.2) | 7 (2.3) | 8 | 1.51(0.14,1.7) | 0.74 | |
| Divorced | 2 (2.4) | 3 (0.96) | 5 | 1.2 (0.3 ,7.7) | 0.07 | |
| Widowed | 0 (0) | 2 (0.6) | 2 | 1 | ||
| occupation | House wife | 43 (51.1) | 149 (47.9) | 192 | 0.59(0.47,4.2) | 0.584 |
| Civil servant | 15 (17.9) | 74 (23.8) | 89 | 0.61(0.23,1.4) | 0.234 | |
| Merchant | 5 (59.5) | 24 (7.7) | 27 | 0.75(0.22,2.6) | 0.652 | |
| others | 21(25) | 66 (31.2) | 87 | 1.13(0.51,2.5) | 0.768 | |
| Education status | Illiterate | 9 (10.7) | 11(3.5) | 20 | 2.12(2.47,6.8) | 0.037 |
| Read and write | 4 (47.6) | 10 (3.2) | 14 | 1 | ||
| 1-8 grade | 20 (23.8) | 61(19.6) | 81 | 1 | ||
| 9-12 grade | 33 (39.3) | 125 (40.2) | 158 | 0.78(0.21,3.45) | 0.56 | |
| Diploma/degree | 18 (21.4) | 104 (33.4) | 122 | 0.89(0.91,1.9) | 0.66 | |
| Income | < 230 ETB | 0 (0) | 1(0.32) | 1 | ||
| 231-850ETB | 7(83.3) | 45 (14.5) | 55 | 0.66(0.27,1.6) | 0.361 | |
| 851-2350ETB | 28 (33.3) | 97 (31.2) | 125 | 0.434(0.15,1.3) | 0.134 | |
| >2350ETB | 17 (20.2) | 70 (22.5) | 87 | 0.63(0.17,2.41) | 0.613 | |
| I don’t know | 31(36.9) | 96 (30.9) | 127 | 1.547(0.67,3.5) | 0.290 | |
| Family size | <=4 | 16 (19) | 164 (52.7) | 180 | 1 | |
| > 4 | 68 (81) | 147(47.3) | 215 | 1.73(1.13,4.2) | 0.043 | |
Table 2: Anemia and socio-demographic characteristics among pregnant women attending antenatal care follow up at Tikur Anbessa Hospital, from November 23, 2012 – March 8, 2013.
Obstetrics and other characteristics and anemia
Two hundred sixty two (66.3%) of the respondents were multigravidae and one hundred thirty five (34.2%) were multiparous. About 40.3% of the respondents had birth interval of greater than two years and 42.5% of the multiparous pregnant women delivered their children at health institutions. Two hundred forty one (61%) of them had no history of excess blood loss/abortion in their previous pregnancy and 49.1% of the responded that they use contraceptives.
10.4% of the multigravidae did not follow ANC in their previous pregnancy. Small number of the respondents, 2.5% and 1.5% had history of blood transfusion and malarial infection in the last one year respectively
The prevalence of anemia in this study was 17.29% and 23.37% for primigravida and multigravida respectively. The prevalence of anemia in multipara was more 24.44% (33/135) than primipara 22.22% (26/117) and in those who were nulliparous 25/143 (17.48%). Anemia was also found to increase as the gestational age increases, showing the highest prevalence in the third trimester 35.48% (33/93) than second 21.64% (29/134) and first trimester 13.09% (22/168). Women with birth interval of less than two years had shown more prevalence of anemia (32/93(34.4%)) than those with an interval of greater than or equal to two years 29/159 (18.23%) and women with no history of delivery 23/143(16.08%). Place of delivery also showed difference in prevalence of anemia (28.9% in the pregnant women who delivered at home and 22.02% in women who delivered at health institution).Contraceptive users showed lower prevalence of anemia (18.04%) compared to none users (24.37%) (Table 3).
| Variables | Anemic (N=84) Number (%) | Non-anemic (N=311) Number (%) | Total | AOR(95%CI) | p-value | |
| Gravida | Primi gravida | 23(27.38) | 110 (35.37) | 133 | 1 | |
| Multi-gravida | 61(72.62) | 201(64.63) | 262 | 1.22(1.01,3.42) | 0.021 | |
| Trimester | <13wks | 22 (26.2) | 146 (46.95) | 168 | 0.71(0.23,1.63) | 0.72 |
| 13-24wks | 29 (34.52) | 105(33.76) | 134 | 1.1(0.49,1.17) | 0.62 | |
| >24wks | 33 (39.28) | 60 (19.29) | 93 | 2.04(2.65,5.12) | 0.41 | |
| Parity | Nulli parous | 25(29.76) | 118 (37.94) | 143 | 1 | |
| Primipara | 26 (30.95) | 91(29.26) | 117 | 1 | ||
| Multipara | 33 (39.3) | 102 (32.8) | 135 | 2.19(3.19,4.32) | 0.031 | |
| Birth interval | <2years | 32(38.09) | 61(19.61) | 93 | 1.21(2.16, 5.19) | 0.012 |
| >=2years | 29 (34.52) | 130 (41.8) | 159 | 1 | ||
| Place of delivery | At home | 24(28.57) | 59 (18.97) | 83 | 0.33(0.11,2.19) | 0.576 |
| At health institution | 37 (44.04) | 131(42.12) | 168 | 0.88(0.94,3.18) | 0.73 | |
| Blood loss | Yes | 8 (9.52) | 13 (4.18) | 21 | 1.67(4.01,20.13) | 0.04 |
| No | 53 (63.09) | 188 (60.45) | 241 | 1 | ||
| Contraception | Yes | 35 (41.67) | 159 (51.13) | 194 | 0.93(0.73,4.71) | 0.069 |
| No | 49 (58.33) | 152 (48.87) | 201 | 2.31(1.2,4.41) | 0.011 | |
| ANC | Yes | 57 (67.86) | 164 (52.73) | 221 | 0.31(2.32,4.13) | 0.07 |
| No | 4 (4.76) | 37 (11.9) | 41 | 1.11(1.67,25.1) | 0.007 | |
| Transfusion | Yes | 2 (2.38) | 8 (2.57) | 10 | 0.33(0.67,5.19) | 0.72 |
| No | 82 (97.62) | 303 (97.42) | 385 | 0.59(0.92,4.23) | 0.82 | |
| Malaria | Yes | 2 (2.38) | 4 (1.3) | 6 | 1 | |
| No | 82 (97.38) | 307 (98.7) | 389 | 0.91(0.18,6.19) | 0.71 | |
Table 3: Distribution of anemia among pregnant women with Obstetric and other variables attending antenatal care at Tikur Anbessa Specialized Hospital from November 23, 2012-March 8, 2013
Dietary habits and anemia
Out of 395 respondents 146 (36.96%) had the habit of eating meat and animal products once per week, 102 (25.82%) once in a month, 83 (21%) every other day and 11 once in a year. One hundred thirty three (33.67%) of the respondents had the habit of eating green leafy vegetables. 127 (32.15%), 90 (22.78%), and 37 (9.36%) had the habit of eating green leafy vegetables every other day, once per week and once in a month respectively. Two hundred eighty eight (72.9%) of the study subjects had the habit of drinking coffee/tea immediately after meal and two hundred sixty three (66.58%) had the habit of eating fruits after meal. Multiple logistic regressions did not show statistically significant association between anemia and any of the dietary habits (Table 4).
| Eating habit | Anemic (N=84) Number (%) | Non-anemic (N=311) Number (%) | Total | AOR(95%CI) | p-value | |
| Frequency of eating animal foods | I don’t eat | 0(0) | 1(0.32) | 1 | 1.19(0.91,4.32) | 0.061 |
| Daily | 7 (8.33) | 45 (14.47) | 52 | 1 | ||
| Every other day | 14 (16.7) | 69 (22.2) | 83 | 0.94(0.23,5.7) | 0.072 | |
| Once per week | 33 (39.3) | 113 (36.33) | 146 | 1 | ||
| Once in a month | 25 (29.76) | 77 (24.76) | 102 | 1 | ||
| Frequency of eating green leafy vegetables | I don’t eat | 1 (1.19) | 6 (1.93) | 7 | 3.21(0.87,6.78) | 0.063 |
| Daily | 24(28.57) | 66 (21.22) | 90 | 1.12(0.29,3.21) | 0.054 | |
| Every other day | 29 (34.52) | 104 (33.44) | 133 | 1 | ||
| Once per week | 26 (30.95) | 101(32.48) | 127 | 1.45(0.57,2.19) | 0.063 | |
| Once in a month | 4 (4.76) | 33 (10.61) | 37 | 1 | ||
| Taking tea/coffee immediately after meal | Yes | 63 (75) | 225 (72.35) | 288 | 1 | |
| No | 21(25) | 86 (27.65) | 107 | 1.98(0.61,4.32) | 0.069 | |
| Taking fruit after meal | Yes | 53 (63.1) | 210 (67.5) | 263 | 1.48(0.97,3.17) | 0.076 |
| No | 31(36.9) | 101 (32.5) | 132 | 1 | ||
Table 4: Distribution of anemia with dietary habit among pregnant mother attending antenatal care at Tikur Anbessa Specialized Hospital from November 23, 2012- March 8, 2013
The prevalence of anemia in this study population using a cut off level of Hb <11 g/dl (<33% haematocrit) was 21.3% (84/395). This result is almost consistent with across sectional study carried out in Gonder (23%) and in the University of Port Harcourt Teaching Hospital, Port Harcourt in Nigeria which had shown a prevalence rate of 23.2% [12,13]. In contrast to this study, a study conducted at Health Promotion Hospital Nakhonsawan, in Thailand showed a prevalence rate of 14.1% [14].This may be due to a difference in socio-economic and educa tional status between the study populations in the two study areas. The result of the present study is much lower than that of Jima (57%), Assendabo (62.7%), Peru (50%), Western Maharashtra, India (92.38%), highlands of Tibet (China) (70%) and most of the pregnant women of developing countries (35-75%) [2,5,15-17]. Other similar studies conducted in east Anatonian province; Turkey, the highlands of Tanzania and in rural areas of Kenya had shown prevalence of 27.1%, 28% and 33% respectively [11,18,19]. This discrepancy might be because of the strengthened health educations given at health institutions during ANC follow up and that there was time difference and this study is done only in the urban women. Additionally, it could be due to the variation of the method where sahli’s method was used in previous studies conducted in Jimma and Assendabo. In comparison to the standard method (Fluid based system hematology analyzer) used in this study, the Sahli’s technique was reported to be much less satisfactory under operational circumstances, chiefly because of dilution problems involved in the use of ordinary manual pipettes and subjective bias during visual comparison [20,21].
Out of all anemic pregnant mothers, 80.95% (68/84) of them had mild anemia, 17.86% (15/84) had moderate anemia and 1.19% (1/84) had severe anemia according to WHO classification for degree of anemia. In contrast to this study, a study conducted in Kenya and in Jimma had shown moderate anemia in 68% and 74.3% respectively [11,22]. This inconsistency may be because of the strengthened health education given on risk factors and prevention of anemia and interventions given at health institutions during ANC follow up in an attempt to reduce the prevalence and severity of anemia among pregnant mothers. In addition, it might because of time and place difference between the present study and the study conducted in Kenya and in Jima.
Anemia in pregnancy is related to different socio-demographic factors [23]. In different studies, age, educational status, economic position have been found to be significantly associated with anemia during pregnancy [24,25]. This study has assessed socio-demographic variables associated with anemia but only age (39-45 yrs (AOR=1.21)), educational status (illiterate (AOR=2.12)) and family size (greater than four (AOR=1.73)) had shown statistically significant association with anemia which indicates the higher prevalence of anemia in illiterates, large family size and aged pregnant mothers. This high prevalence of anemia in these study participants might be due to inadequate knowledge on factors causing anemia and on how to prevent the risk factors. Similar study conducted on prevalence and risk factors of anemia in rural areas of India and in Jimma showed a statistical significant association between education and anemia and in Turkey, between anemia and large family size which are consistent with this study [16,18,23].
Obstetric factors are known determinants of anemia. In the present study, anemia was 2.04 times more prevalent at third trimester (AOR=2.04). The 26.2% prevalence of anemia at the first trimester increased to 39.28% at the third trimester. This might be due to hemodilution but, it might also indicate poor prenatal care. Anemia was 2.19 and 1.22 times more prevalent in multiparous, multigravidae respectively. This is may be due the fact that multiparity and multigravidity induce anemia by reducing maternal iron reserves at every pregnancy and by causing blood loss at each delivery. There was also a statistically significant association between anemia and history of blood loss (AOR=1.67)), ANC (no ANC (AOR=1.11)) and contraception (no contraception (AOR=2.31)) on multivariate logistic regression analysis which indicates the need for proper follow up of pregnant women starting from the first trimester to the third trimester and the need of attention to multigravidae and multiparous mothers. These findings are consistent with the study conducted in rural areas of Malaysia, in Thailand, in rural areas of Kenya, in the high lands of Tibet and in Jimma which had shown high prevalence of anemia in multiparous, multigravidae and during the third trimester [11,16,17,26].
Appropriate time after each pregnancy for recuperation and replenishment of nutrient stores and circulating levels is a minimum of three to five years. Pregnancy with a short birth interval leads to iron deficiency anemia as iron requirements are substantially higher than the average [27]. The present study has shown a statistically significant association between birth interval and anemia (birth interval of less than two years (AOR=1.21)). Similar finding has also been documented in a study conducted at Jimma hospital [22]. Thus, this finding indicates the need for strengthening of interventions related to child spacing and awareness [28]. One of the major contributory factors for anemia in developing countries is consumption of plant based food containing insufficient iron, especially insufficient available hem iron from meat [29]. Meat is a good source of high quality protein, iron and zinc and of all the B-vitamins except folic acid. Iron absorption is enhanced when consumed with foods high in vitamin C such as orange juice but substances in coffee and tea inhibit iron absorption [27]. This study has tried to assess different dietary risk factors associated with anemia. Eating animal food, green leafy vegetables, taking fruit after meal and drinking tea/coffee did not show significant association with anemia on multivariate logistic regression which may be due to no difference in eating habit among the study participants.
This study is done only at single institution; hence, further studies have to be conducted in different hospitals of Addis Ababa to have findings representing the whole population. Additionally, further laboratory studies have to be conducted to identify the specific causes of anemia in the pregnant mothers so as to guide the health care givers to work alleviating the existing problems.
The overall prevalence of anemia in this study using a cut off level of haemoglobin <11 g/dl (<33% haematocrit) was 21.3% and the majority of them were of the mild type (haemoglobin: 10-10.9 g/dl). Though the prevalence of anemia in this study is lower than prevalence of anemia in previous studies conducted in other areas of Ethiopia, it still remains higher. The present study has shown a statistically significant association between anemia and age, gestational age, gravidity, parity, antenatal care, birth interval, blood loss, family size and educational status (illiterates).This emphasizes the need for continuing strengthening of interventions on factors associated with anemia.
This research was funded by Addis Ababa University Grants for Graduate Research. Therefore, we are grateful to Addis Ababa University, College of Health Sciences for their financial support. Our gratitude also goes to all staff members of Obstetrics and Gynecology of Addis Ababa University for their support and cooperation during the data & sample collection period.