Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Review Article - (2013) Volume 3, Issue 2
Various factors have been shown to be associated with the development of post-ERCP pancreatitis. They are generally classified as patient-related factors and procedure-related factors. These factors exert a synergistic effect on the risk for pancreatitis after ERCP. The pathogenesis of post-ERCP pancreatitis has not been fully understood, but several factors (i.e., mechanical injury, hydrostatic injury, chemical and allergic injury, enzymatic injury, infection, and thermal injury) may act independently or in combination to provoke post-ERCP pancreatitis. Since the introduction of ERCP, numerous pharmacologic agents have been evaluated to prevent post-ERCP pancreatitis on the assumption that they pharmacologically inhibit one or more of the factors associated with pancreatic damage. Pancreatitis is the most common and feared complication of ERCP. Identification of risk factors before and during ERCP is of paramount importance. The benefit of performing ERCP should be outweighed by the risk of post-ERCP pancreatitis.
<Keywords: Post-ERCP pancreatitis; Risk factors; Hydrostatic injury
Acute pancreatitis remains the most common complication of diagnostic and therapeutic ERCP, with a reported incidence of 3-15% in recent prospective multicenter studies [1-3]. Fortunately, most cases of post-ERCP pancreatitis are graded as mild or moderate in severity. Nevertheless, severe or even fatal pancreatitis could occur after ERCP. For example, in a systemic survey of prospective studies, while the rates of mild and moderate post-ERCP pancreatitis were 45% and 44%, respectively, severe pancreatitis developed in 11% of cases with a mortality rate of 3% [4].
Various factors have been shown to be associated with the development of post-ERCP pancreatitis. They are generally classified as patient-related factors and procedure-related factors (Table 1). These factors exert a synergistic effect on the risk for pancreatitis after ERCP [1]. Identification of these risk factors in each patient before and during ERCP is crucial to implement measures for preventing and ameliorating post-ERCP pancreatitis.
The pathogenesis of post-ERCP pancreatitis has not been fully understood, but several factors (i.e., mechanical injury, hydrostatic injury, chemical and allergic injury, enzymatic injury, infection, and thermal injury) may act independently or in combination to provoke post-ERCP pancreatitis. Since the introduction of ERCP, numerous pharmacologic agents have been evaluated to prevent post-ERCP pancreatitis on the assumption that they pharmacologically inhibit one or more of the factors associated with pancreatic damage (Figure 1) [5]. These attempts, however, have been largely disappointing, and agents that have shown a preventive effect against post-ERCP pancreatitis in a multicenter randomized controlled trial (RCT) are limited (gabexate, ulinastatin, and NSAIDs) [6-8]. In the latest meta-analysis, while ulinastatin showed significant efficacy, gabexate was not effective in reducing the incidence of post-ERCP pancreatitis [9]. These protease inhibitors are used exclusively in Japan and are not available globally.
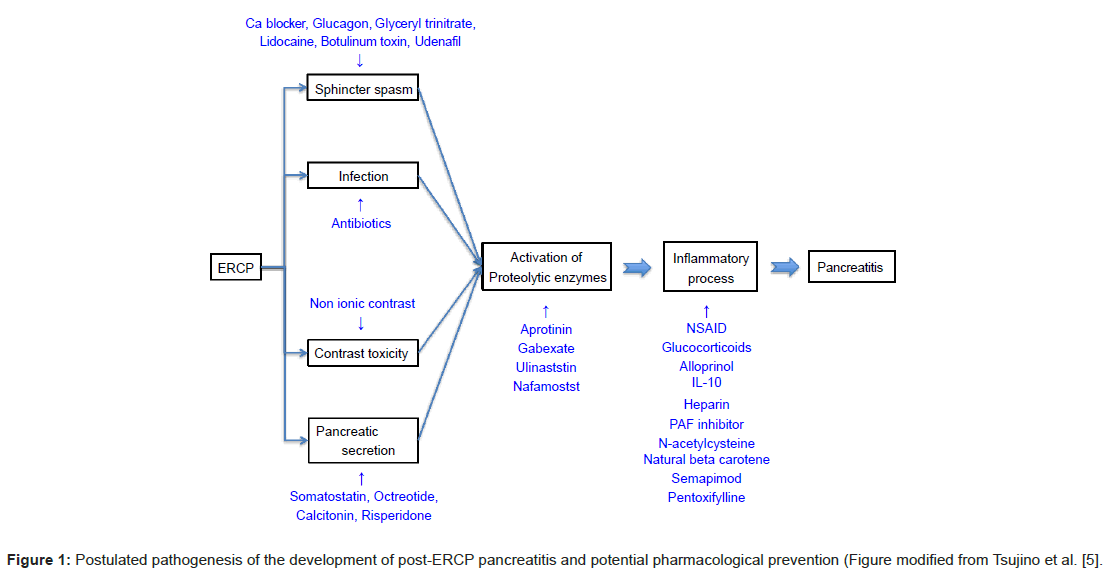
Figure 1: Postulated pathogenesis of the development of post-ERCP pancreatitis and potential pharmacological prevention (Figure modified from Tsujino et al. [5].
Currently, the rectally administration of NSAIDs (diclofenac or indomethacin) is the most promising for the prevention of post-ERCP pancreatitis [8]. In fact, the European Society of Gastrointestinal Endoscopy recommends routine rectal administration of 100 mg diclofenac or indomethacin immediately before or after ERCP [10]. However, it does not seem that this recommendation has become prevailing in routine clinical practice.
Mechanical and/or thermal damage to the papilla and subsequent pancreatic outflow obstruction have been considered as one of the main pathogenesis of post-ERCP pancreatitis. Pancreatic duct stents are prophylactically placed to secure the pancreatic outflow in an attempt to prevent pancreatitis after ERCP. Two meta-analyses showed that pancreatic duct stent placement significantly reduced the incidence of post-ERCP pancreatitis in patients at high risks for this complication [11,12].
Compared with pharmacological prevention, placement of pancreatic duct stent is not easy to perform even in tertiary referral centers and success rate for this procedure is highly operator depend. Moreover, failed attempt of pancreatic duct stent insertion is associated with a high risk of pancreatitis [13]. Prophylactic pancreatic stent placement should be performed by expert endoscopists in patients with the high risk of developing pancreatitis.
Contrast injection into the pancreatic duct and difficult cannulation are risk factors for post-ERCP pancreatitis (Table 1). To avoid unnecessary pancreatography as well as to increase the success rate of primary cannulation, wire-guided cannulation has recently been introduced. In meta-analyses of RCTs comparing wire-guided cannulation with standard contrast-assisted cannulation, wire-guided cannulation significantly decreases the risk of post-ERCP pancreatitis [14,15].
| Patient-related factors | Procedure-related factors |
|---|---|
| Sphincter of Oddi dysfunction | Precut sphincterotomy |
| Female | Pancreatic duct injection |
| Previous pancreatitis | Pancreatic sphincterotomy |
| Younger age | Papillary balloon dilation |
| Absence of chronic pancreatitis | Difficult cannulation |
| Normal serum bilirubin |
Table 1: Risk factors for post-ERCP pancreatitis.
Pancreatitis is the most common and feared complication of ERCP. Identification of risk factors before and during ERCP is of paramount importance. The benefit of performing ERCP should be outweighed by the risk of post-ERCP pancreatitis. To prevent post-ERCP pancreatitis in high-risk patients, the use of rectal NSAIDs, prophylactic pancreatic duct stent placement, and wire-guided cannulation should be considered.