Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2014) Volume 3, Issue 2
Background: A cytology diagnosis of a Hurthle cell lesion does not provide information regarding the presence or absence of thyroid cancer. The risk of malignancy in Hurthle cell lesions varies in the literature, ranging from 4% to 69%. Objectives of this study are to determine what percent of Hurthle cell lesions are found to be malignant on final pathology and to determine if there are demographics, risk factors, or ultrasound characteristics that will preoperatively help predict malignancy. Methods: A total of 99 consecutive patients had a cytology diagnosis of a Hurthle cell lesion. All fine needle aspirations were performed and interpreted at a single tertiary care referral hospital. Final surgical pathology as well as pre-operative variables including demographics, risk factors, and ultrasound characteristics were reviewed. Results: Eighteen of 50 (36%) patients had thyroid cancer on final surgical pathology. None of the pre-operative variables were significantly associated with the final histopathological diagnosis on univariate analysis. Conclusions: A thyroid lobectomy is an acceptable approach for the patient with a cytology diagnosed Hurthle cell lesion, proceeding with a completion thyroidectomy if cancer is seen on final surgical pathology.
<Keywords: Hurthle cell, Lesions, Neoplasms, Risk factors, Cancer
Tuberculosis can affect several sites of the head and neck. The most common form of tuberculosis (TB) of the head and neck area is the TB of the lymph nodes (85%); at other regions tuberculosis is extremely rare, it can affect the larynx (7%), the ear (3%), the pharynx (1.5%), the sinus cavities (1%), the eye (1%), the skull base (1%) and more rarely the thyroid (0.5%) [1].
Swelling of the thyroid gland by tuberculosis is one of the rarest disease, its relative resistance to TB infection has not been adequately explained; around 200 cases of thyroid tuberculosis are reported. Tuberculosis in the thyroid is found in 0.1% of postmortem studies and it has been reported in the 0.1 - 0.4% of cases of thyroid disease treated surgically, however, thyroid tuberculosis microscopic foci may occur in up to 7% of patients with miliary tuberculosis.
First description of secondary thyroid tuberculosis was reported by Lebert in 1862 in a patient with miliary tuberculosis, however, in 1893 Bruns first described primary thyroid tuberculosis accompanied by regional lymphadenitis in a patient without pulmonary tuberculosis [2].
The majority of the cases represent forms of secondary thyroid tuberculosis, in cases of pulmonary or disseminated miliary TB, with primary sources located outside of the thyroid gland; secondary thyroid tuberculosis arises from lymphatic or hematogenous spread of Mycobacteria, or by direct extension from cervical lymphadenitis [1-6].
The primary extrapulmonary form of tuberculosis within the thyroid gland is difficult to explain, it possibly originates from a source of latent intrathyroid infection [3].
Young women are more commonly affected. Duration of symptoms has been reported from a few weeks up to year [2].
The clinical presentation is variable, in the majority of cases it manifests as a thyroid nodule simulating carcinoma with subacute or chronic enlargement of the gland, with or without abscess formation, accompanied by lymphadenopathy, with or without signs and symptoms related to the compression and fibrosis such as dysphagia and dysphonia from vocal cord paralysis; some cases are asymptomatic. There may be signs of systemic disease like fever and weight loss.
In the early stages, thyroid tuberculous disease manifests as a solitary thyroid nodule, firm and painless, later, multiple nodules (with cheese abscesses) can be seen in association with cervical lymphadenopathy or abscesses of soft tissues (with or without fistula); rarely presents as an abscess in the thyroid gland.
Thyroid function is preserved normal clinically and biochemically in the vast majority of cases, although thyrotoxicosis, usually at the beginning of the glandular affection; hypothyroidism caused by replacement of thyroid tissue is extremely rare.
The diagnostic workup includes imaging studies such as ultrasound, computed tomography scan, as well as fine needle aspiration biopsy with Ziehl Neelsen stain, culture and histopathological study [2,5].
The ultrasound findings include a heterogeneous mass or multiple hipoecoic areas in thyroid associated with growth of cervical lymph nodes. The CT scan shows nodules with necrotic centers seen as central attenuation with peripheral reinforcement in the thyroid gland; abscesses in the adjacent cervical soft tissues may also be seen [1,9].
Biopsy aspiration in some cases can be diagnostic if identify acid alcohol resistant staining bacilli, it can report inflammatory process or be inadequate for diagnosis; material for culture and PCR study can be obtained [2,5,7].
Histological examination of the surgical specimen (which is usually removed by suspicion of thyroid carcinoma) reveals that the thyroid tissue has been replaced in one or more areas by granulomatous inflammation where can be identified epitheloid cells and Langhans multinucleated giant cells within whitish tuberculous nodules, whose central portion shows pockets of caseous necrosis, calcification and fibrosis. Ziehl Neelsen stain may identify tuberculosis bacilli [1,2].
The three histological criteria for the diagnosis of tuberculosis in the thyroid, described by Seed in 1939 are presence of acid-fast bacilli, necrosis or abscess in the gland and presence of a focus of TB outside the thyroid (not essential criteria) [2,8,9].
Although there is some controversy about the treatment of primary thyroid tuberculosis, medical treatment with rifampin, isoniazid and pyrazinamide for nine months, generally has been accompanied by some form of surgical treatment, since most cases occur as suspicious lesion of malignancy that requires surgical assessment or requires drainage of an abscess [10].
A 69-year-old male patient with history of alcoholism and malnutrition, who denies family history of tuberculosis, is presented. His past medical history includes a cervical abscess with fistula to the skin 5 years ago.
He began his current condition 1 year ago, presenting with a not painful mass in his anterior cervical region, with slowly progressive growth, accompanied by weight loss of 5 kg, then presented additional masses at his left neck chain and ipsilateral supraclavicular triangle. No pulmonary symptoms or fever were reported.
Physical examination showed increased neck volume located at the left thyroid lobe, of 4x4cm, with firm consistency, scrolling with swallowing, with a cutaneous fistula of approximately 3mm in diameter at the midline and other supraclavicular fistula without secretions, many lymphadenopathies of 3×2 cm in diameter, located at the ipsilateral jugular chain were palpated (Figure 1), 70° laryngoscopy revealed normal mobility of the vocal cords.
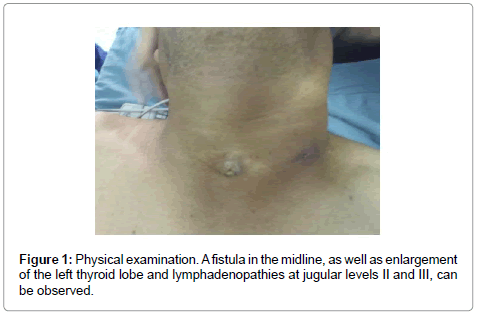
Figure 1: Physical examination. A fistula in the midline, as well as enlargement of the left thyroid lobe and lymphadenopathies at jugular levels II and III, can be observed.
Thyroid carcinoma with cervical metastases versus lymph node tuberculosis was considered and clinical tests were performed.
Laboratory studies: Leukocytes count of 8400/mm3, hemoglobin 12.1 mg/dl, glucose 100 mg/dl, HIV negative, normal thyroid function tests, normal calcitonin.
It was reported on a fine needle aspiration biopsy of a neck node and thyroid nodule compatible with chronic granulomatous hyperplasia; all cultures were negative. Computed neck tomography scan showed a dependent mass of the thyroid lobe with inside calcifications, cervical lymphadenopathies and a prevertebral abscess (Figures 2 and 3); a low uptake nodule in the left lobe appeared on a 99tc scan. Thorax radiography was normal.
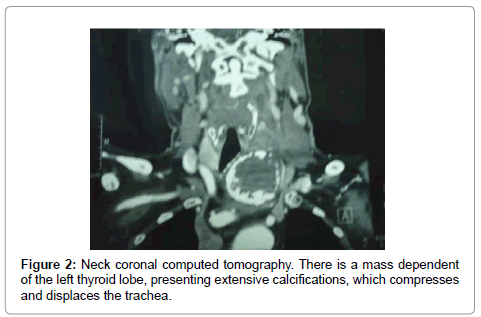
Figure 2:Neck coronal computed tomography. There is a mass dependent of the left thyroid lobe, presenting extensive calcifications, which compresses and displaces the trachea.
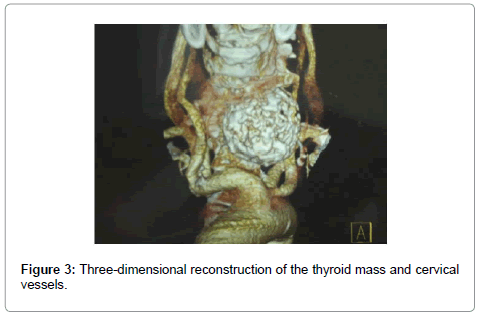
Figure 3: Three-dimensional reconstruction of the thyroid mass and cervical vessels.
Surgical treatment for drainage of the prevertebral abscess, hemi thyroidectomy and modified neck dissection with intraoperative study were performed (Figures 4 and 5).
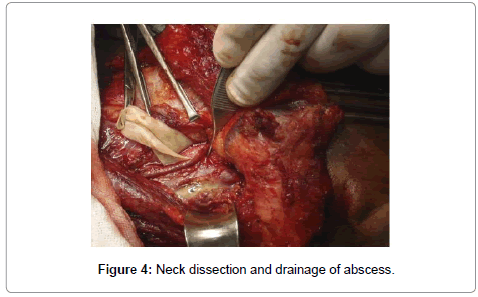
Figure 4: Neck dissection and drainage of abscess.
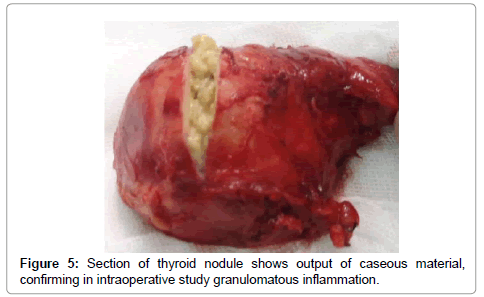
Figure 5: Section of thyroid nodule shows output of caseous material, confirming in intraoperative study granulomatous inflammation.
Surgery was carried out through a hockey stick incision, which included the fistula tracts, subplatismal plane flaps were elevated and a modified neck dissection was done by removing the lymph nodes attached to the internal jugular vein by fibrosis at levels II and III. Prevertebral abscess was drained by blunt dissection. Following, the left thyroid lobe was removed which was found firmly attached to the adjacent tissues by fibrosis; recurrent laryngeal nerve and one of the ipsilateral parathyroid gland were preserved. Surgical procedure was terminated after an intraoperative study was reported compatible with TB granulomatous inflammation. No postoperative complications resulted. A definitive histopathological report confirmed granulomatous inflammation by tuberculosis (Figures 6 and 7). For the following 9 months, patient completed a supervised standard TB medical treatment.
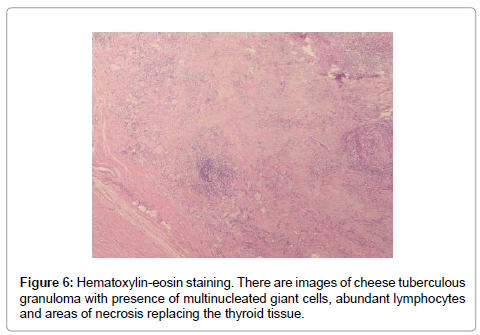
Figure 6: Hematoxylin-eosin staining. There are images of cheese tuberculous granuloma with presence of multinucleated giant cells, abundant lymphocytes and areas of necrosis replacing the thyroid tissue.
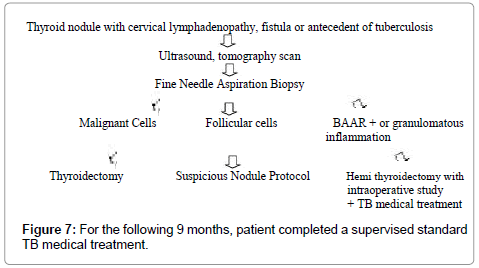
Figure 7: For the following 9 months, patient completed a supervised standard TB medical treatment.
To our knowledge, this is the first case of primary thyroid tuberculosis diagnosed by intraoperative study reported in Mexico. Primary thyroid tuberculosis is still very rare, although several forms of extrapulmonary tuberculosis are seen more often, particularly in patients with HIV infection or diabetes mellitus. In this case, the patient had malnutrition and alcoholism as risk factors [3,4].
Diagnosis of thyroid tuberculosis is rarely performed by preoperative clinical suspicion. The clinical presentation usually imitates cancer or thyroid gland abscess and, in general, as in the case presented, is diagnosed with the histopathological study after thyroidectomy; imaging studies are not specific, and in fact, when there are primary pulmonary lesions caused by tuberculosis, they have been confused with metastases [2].
The preoperative diagnosis is feasible when the FNAB made in the evaluation of a thyroid nodule, is found positive for tuberculosis; or also, when an abscess is formed in a patient with known pulmonary tuberculosis. Other studies diagnostic as a culture, erythrocyte sedimentation and tuberculin skin test can be useful. The test QuantiFERON TB (QFT-GIT) that measures the release of interferon-γ in blood in response to stimulation by TB antigen can diagnose latent tuberculosis infection; clinical evaluation and additional tests are needed to differentiate between latent or active TB. In the case presented, the presence of cutaneous fistula could have woken up the clinical suspicion, but we have also seen cases of undifferentiated thyroid carcinoma with fistula and abscess [3,5,7,11,12].
A preoperative or intraoperative diagnosis could allow a more limited surgery as drainage of abscess or hemi thyroidectomy; in addition, to reduce surgical risks as there may be significant fibrosis that makes it a very difficult dissection, as in the case here presented and other reports [2-4,13-15].
Thyroid tuberculosis, although it is not common, need to be included in the differential diagnosis of thyroid cancer (which can coexist), giant cell thyroiditis and other granulomatous diseases such as sarcoidosis and actinomycosis, particularly in patients with a history of familial tuberculosis, immunosuppressed or with malnutrition [1,2].
A study protocol for thyroid nodules accompanied by cervical lymphadenopathy, which emphasizes the importance of considering the clinical presentation with fistula or history of tuberculosis, the results of the FNAB Ziehl Neelsen stain, QFT-GIT, and the intraoperative study for the diagnosis of thyroid tuberculosis is proposed.