Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2013) Volume 2, Issue 2
Vascular endothelial growth factors are the most powerful molecules related to angiogenesis and lymph angiogenesis stimulation and are frequently associated to a worse prognosis in many malignancies. Currently, anti-angiogenic VEGF-A165b has been described and it have been demonstrated to efficiently block the angiogenic sprout. We sought to investigate the VEGF family members expression involved with angiogenesis (including the anti-angiogenic VEGF-A165b) and lymph angiogenesis. The casuistic was composed by 196 cases. The frequencies of thyroid lesions were: 53 (27%) goitres, 16 (8%) thyroiditis, 9 (5%) follicular adenomas, 84 (43%) papillary carcinomas, and 34 (17%) follicular carcinomas. The immunohistochemical reactions for VEGF-A, VEGF-A165b, VEGF-B, VEGF-C and VEGF-D were performed and semi-quantitatively assessed. We observed a widespread positive immunoexpression of VEGF-A and VEGF-A165b in benign and malignant lesions. None of the benign samples of this casuistic had positive immunoexpression of VEGF-B and only a few positive cases were detected in both papillary and follicular carcinomas. The highest levels of VEGF-C and VEGF-D expression were found in papillary carcinomas. There was a relevant association of VEGF-D and a worst tumoral staging (p=0.004) in papillary carcinomas. We also identified a significant association between VEGF-A and vascular invasion (p=0.049) and patient’s age and an increased expression of VEGF-B (p=0.047) in papillary thyroid carcinomas. No association was found for follicular carcinomas.
<Keywords: Thyroid cancer; Angiogenesis; Lymph angiogenesis; Immunohistochemistry; Vascular endothelial growth factor
The regulation of vasculogenesis, haematopoiesis, angiogenesis, lymph angiogenesis and vascular permeability are very complex. Several molecules, such as the family of VEGFs (vascular endothelial growth factors) and other growth factors have been described as important regulators of tumour angiogenesis and lymph angiogenesis, and are thus considered important therapeutic targets [1,2]. In the early 70s, Folkman’s postulates [3] showed that angiogenesis is a crucial step of neoplastic development and a vital parameter to understanding the process of cancer biology, first for his essential role in neoplastic proliferation by supplying the energy required for tumour growth, and because of its potential as a therapeutic target. Currently several pro or anti angiogenic drugs have been approved by the FDA or are in clinical trials [4].
The family of VEGFs comprises a group of highly conserved factors regulating vasculogenesis, haematopoiesis, angiogenesis, lymph angiogenesis and vascular permeability [5,6]. The VEGF family members in mammals comprise VEGF-A, VEGF-B, VEGF-C, VEGF-D and placental growth factor (PlGF). These glycoproteins belong to a super family of factors that include platelet-derived growth factor (PDGF). There are also three tyrosine kinase receptors (TKR) that belong to the family: VEGFR-1 (Flt-1), VEGFR-2 (KDR) and VEGFR-3 (Flt-4). The VEGFR-1 (vascular endothelial growth factor receptor 1) binds to VEGF-A and-B, VEGFR-2 binds to VEGF-A, -C and-D and VEGFR-3 binds to VEGF-C and - D [6,7]. Neuropilin - 1 (NP-1) and Neuropilin - 2 (NP-2) are co-receptors for some VEGF isoforms and subtypes [7].
VEGF-A is primarily related to angiogenesis while VEGF-C and VEGF-D are involved in lymph angiogenesis [8]. Little is known about the meaning of the expression of VEGF-B in tumours [5]. Recently, new isoforms generated by alternative splicing has been identified such as VEGF-A165b. Alternative splicing of the splicing distal site of exon 8 generates this isoform. Currently, it is known that VEGF-A has two isoforms of mRNA produced: the pro-angiogenic isoforms (VEGF-Axxx) and the anti-angiogenic (VEGF-Axxxb), where xxx is the number of amino acids of the mature protein. The structure of VEGF-A protein contains the dimerization sites and the heparin binding sites for VEGFR-1 and -2, which are present in all isoforms. The six amino acids from the c-terminal end of the protein will determine whether the isoform of VEGF is pro-angiogenic or anti-angiogenic. This difference promotes profound implications for the structure, interaction with receptors and function [9]. The VEGF-A165b binds with equivalent affinity to VEGF165 in VEGFR-2 receptor; however, does not promote their activation or stimulation for subsequent signalling pathways [10].
The VEGFs are important peptides that have been widely investigated in several conditions, physiological such as the growth of the endometrium and embryonic development and pathological such as in tumour growth and metastasis [1,2,7,8,11]. The increased expression of VEGF in tumours has been associated with a poor prognosis or increased risk of recurrence or metastasis in several types of cancers [12]. In recent years some studies have demonstrated the expression of VEGF family members and its receptors in angiogenesis and lymph angiogenesis of different thyroid lesions [13-17], but the involvement of angiogenesis and lymph angiogenesis in the pathogenesis of thyroid carcinomas has not yet been elucidated. The pattern of tumour behaviour and metastasis vary with the type of tumour and has not been fully explored whether the differences in the angiogenic and lymphangiogenic phenotypes determine a more aggressive behaviour and influence tumour metastasis [13]. In addition, only few studies evaluate the expression of anti-angiogenic variants in human cancers.
The objective of the present study was to determine the immunohistochemical expression of pro-angiogenic vascular endothelial growth factors VEGF-A, VEGF-B, VEGF-C and VEGF-D, and his anti-angiogenic variant VEGF-A165b in a series of malignant and benign thyroid lesions and correlate their expressions with the clinicopathological data.
The casuistic comprised a series of formalin-fixed, paraffinembedded tissues from 196 patients submitted to thyroidectomy. The frequencies of different thyroid lesions were: 53 (27%) goitres, 16 (8%) thyroiditis, 9 (5%) follicular adenomas, 84 (43%) papillary carcinomas, and 34 (17%) follicular carcinomas.
The papillary carcinoma samples comprised 55 samples (65.5%) of papillary carcinoma of conventional form, 14 samples (16.7%) of follicular variant of papillary carcinoma, one sample (1.2%) of tall cell variant of papillary carcinoma, three samples (3.6%) of oxyphilic variant of papillary carcinoma, 8 samples (9.5%) of papillary micro carcinoma and 3 samples (3.6%) of follicular variant of papillary micro carcinoma. For statistical purposes, all papillary carcinomas were grouped as a single type.
All patients were submitted to surgical resection by the same surgeon (RSC) and the diagnoses were categorized according to the World Health Organization classification [18] by one of the authors (KSES).
Pathological features herein evaluated included macroscopic presentation, principal site of the tumour, histological type, and status of resection margins, vascular and capsular invasion, metastasis and TNM staging.
Tissue microarray construction
Slides from all 196 specimens were reviewed and mapped, and tissue microarrays were building using manual tissue arrayed (MTA-1 Beecher Instrument, USA). Representative areas of the thyroid lesions were selected and cores of 1.0 mm in diameter were twice sampled and arranged at 0.3 mm, one from each other, in the recipient paraffin block. A database was build for every block produced, including the coordinates of each core and case of origin.
Immunohistochemistry
The immunohistochemical expressions of VEGF-A, VEGF-A165b, VEGF-B, VEGF-C and VEGF-D were semi-quantitatively assessed.
VEGFs protocol followed Garcia et al. [17] recommendations. Briefly, deparaffinised and rehydrated sections were immersed in 0.01 M citrate buffer (pH 6.0) and heated at 98°C for 20 min for epitope– antigen retrieval. Subsequently, endogenous peroxidase was blocked with 0.3% hydrogen peroxide in methanol. Primary antibody incubation step was done with 1:800 dilution for VEGF-A (monoclonal antibody clone VG-1, Abcam, USA), 1:50 dilution for VEGF-A165b (monoclonal antibody clone MRVL56/1, Abcam, USA), 1:50 dilution for VEGF-B (monoclonal antibody clone 58013, R&D Systems, USA), 1:200 dilution for VEGF-C (polyclonal antibody, Zymed Laboratories, USA) and 1:200 dilution for VEGF-D (monoclonal antibody clone 78923, R&D Systems, USA), all overnight at 4°C. All primary antibodies were diluted in bovine serum albumin (BSA) (Sigma, USA) and 1.0% sodium azide NaN3 (Inlab, Brazil) 0.1% in PBS buffer. The amplification method used was the polymer system Novolink (Novocastra Laboratories, UK). Visualization was developed with 3,3’-diamino-benzidine (DAKO Corporation, USA) and counterstaining with Harris haematoxylin (Merck, Germany). Negative controls were obtained by omitting the primary antibody incubation step; and human tonsil was used as positive controls.
Immunohistochemical evaluation
Expression of VEGF-A, VEGF-A165b, VEGF-B, VEGF-C and VEGF-D by neoplastic and non-neoplastic samples was semi-quantified under 200× magnification, considering positive reaction decorating membrane and/or cytoplasmic of normal, follicular, or malignant thyroid cells. The evaluation was performed blindly and the tissue microarray spot of each sample were fully analyzed. The following grading system was used: negative (0) absence of expression, + positive staining with expression in up to 10% of cells, ++ positive expression in over 10% up to 25% of cells, +++ positive expression in over 25% up to 50% of cells, and ++++ positive expression in over 50% of cells. For statistical analyses purposes, VEGF-A, VEGF-A165b, VEGF-B, and VEGF-C and VEGF-D expression was dichotomized in two categories: negative (0 up to 10% of positivity) and positive (over 10% of positive reaction).
Statistical analysis
The data were obtained from the available information on patient’s files and tissue samples revised. Accordingly, the statistics were based on these variables.
The relationship between VEGF-A, VEGF-A165b, VEGF-B, VEGF-C and VEGF-D expression and clinicopathologic features were examined using Pear- son’s chi-square (X2) test or Fisher’s exact test when appropriate and considered significant when p<0.05. The Mann– Whitney test was used for continuous variables.
Data were analyzed with Statistical Package of Social Sciences software, version 13.0.
Considering all samples, a total of 196 thyroidectomy specimens were evaluated. Women were 5.1-fold more likely to be affected than men (83.7% female and 16.3% male patients) and the mean age was 45.9 years old.
In the papillary thyroid carcinomas group women were 5.4-fold more likely to be affected than men (84.3% female and 15.7% male patients). In this patient setting the age for 54.2% (n = 45) was 45 years or less and for 45.8% (n = 38) was 45 or greater than this. The mean tumour size was 1.78 cm ± 1.5 (mean ± SD) and they were found predominantly in the in the right lobe (31.1%), left (24.3%) or with diffuse presentation (21.6%). Association with goitre was present in 22.6% (n = 19), with thyroiditis in 17.9% (n = 15) and both in 1.2% (n = 1) of papillary carcinomas studied. In 58.3% (n = 49) of the studied cases we did not detect any association. Capsular invasion was present in 17.9% (n = 15) of cases and was not detected in 82.1% (n = 69) and vascular invasion was observed in 16.7% (n = 14) of cases and was not detected in 83.3% (n = 70). Perithyroidal soft tissue was invaded in 10.7% (n = 9) and metastasis was detected in 13.1% (n = 11). Papillary thyroid carcinomas showed staging (TNM) I in 80.5% (n = 66), II 8.5% (n = 7), III 4.9% (n = 4) and IVA at 6, 1% (n = 5) (Table 1).
| n | % | ||
|---|---|---|---|
| Gender | |||
| (n=83) | M | 13 | 15.7% |
| F | 70 | 84.3% | |
| Age | |||
| (n=83) | < 45 y.o. | 45 | 54.2% |
| > or = 45 y.o. | 38 | 45.8% | |
| Size (cm) Mean (+ SD) | 1,78 + 1,5 | ||
| Capsular Invasion | |||
| (n=84) | Present | 15 | 17.9% |
| Non-detected | 69 | 82.1% | |
| Vascular Invasion | |||
| (n=84) | Present | 14 | 16.7% |
| Non-detected | 70 | 83.3% | |
| Perithyroidal Soft Tissue Compromise | |||
| (n=84) | Present | 9 | 10.7% |
| Non-detected | 75 | 89.3% | |
| Metastasis | |||
| (n=84) | Present | 11 | 13.1% |
| Non-detected | 73 | 86.9% | |
| Staging (TNM) | |||
| (n=82) | I | 66 | 80.5% |
| II | 7 | 8.5% | |
| III | 4 | 4.9% | |
| IVA | 5 | 6.1% | |
Table 1: Summary of clinicopathological features in the papillary thyroid carcinomas
group
In the follicular thyroid carcinomas group wmomen were 7.4-fold more likely to be affected than men (88.2% female and 11.8% male patients). In this patient setting the age for 55.9% (n = 19) was 45 years or less and for 44.1% (n = 15) was 45 or greater than this. The mean tumour size was 2.55 cm ± 0.98 (mean ± SD) and they were found predominantly in the in the right lobe (57.6%), left (15.2%) or with diffuse presentation (24.2%). Association with goitre was present in 17.6% (n = 6), with thyroiditis in 8.8% (n = 3) and both in 5.9% (n = 2) of follicular carcinomas studied. In 67.6% (n = 23) of the studied cases we did not detect any association. Vascular invasion was present in 26.5% (n = 9) of cases and was not detected in 73.5% (n = 25). Perithyroidal soft tissue was invaded in 5.9% (n = 2) and metastasis was not observed in any of these cases. The follicular carcinoma showed staging (TNM) I in 64.7% (n = 22), II in 29.4% (n = 10) and III in 5.9% (n = 2) (Table 2).
| n | % | ||
|---|---|---|---|
| Gender | |||
| (n=34) | M | 4 | 11.8% |
| F | 30 | 88.2% | |
| Age | |||
| (n=34) | < 45 y.o. | 19 | 55.9% |
| > or = 45 y.o. | 15 | 44.1% | |
| Size (cm) Mean (+ SD) | 2,55 + 0,98 | ||
| Vascular Invasion | |||
| (n=34) | Present | 9 | 26.5% |
| Non-detected | 25 | 73.5% | |
| Perithyroidal Soft Tissue Compromise | |||
| (n=34) | Present | 2 | 5.9% |
| Non-detected | 32 | 94.1% | |
| Metastasis | |||
| (n=34) | Non-detected | 34 | 100% |
| Staging (TNM) | |||
| (n=34) | I | 22 | 64.7% |
| II | 10 | 29.4% | |
| III | 2 | 5.9% | |
Table 2: Summary of clinicopathological features in the follicular thyroid carcinomas group.
Illustrative photomicrographies of the immunohistochemical expression patterns obtained for VEGF-A, VEGF-A165b, VEGF-B, VEGF-C and VEGF-D in papillary and follicular carcinomas are shown in figure 1.
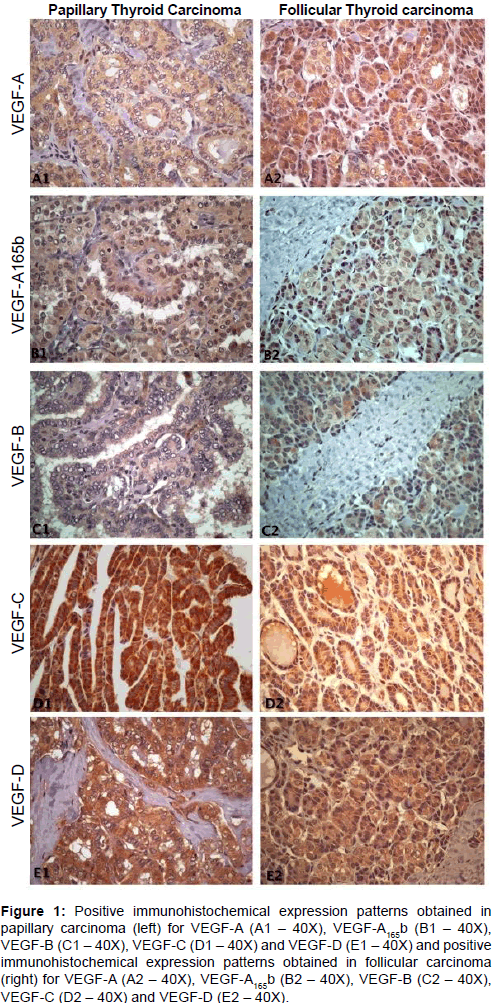
Figure 1: Positive immunohistochemical expression patterns obtained in papillary carcinoma (left) for VEGF-A (A1 – 40X), VEGF-A165b (B1 – 40X), VEGF-B (C1 – 40X), VEGF-C (D1 – 40X) and VEGF-D (E1 – 40X) and positive immunohistochemical expression patterns obtained in follicular carcinoma (right) for VEGF-A (A2 – 40X), VEGF-A165b (B2 – 40X), VEGF-B (C2 – 40X), VEGF-C (D2 – 40X) and VEGF-D (E2 – 40X).
Our findings demonstrate a gradual increase in the intensity of immunohistochemical expression of all vascular endothelial growth factors studied from thyroid tissue with normal phenotype (data not shown), benign proliferative lesions and malignant neoplasms (Table 3).
| VEGF-A | VEGF-A165b | VEGF-B | VEGF-C | VEGF-D | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Negative (< 10%) | Positive (> or equal 10%) | n | Negative (< 10%) | Positive (> or equal 10%) | n | Negative (< 10%) | Positive (> or equal 10%) | n | Negative (< 10%) | Positive (> or equal 10%) | n | Negative (< 10%) | Positive (> or equal 10%) | n | |
| Papillary Carcinoma | 3 (5%) | 63 (96%) | 66 | 12 (19%) | 51 (81%) | 63 | 58 (92%) | 5 (8%) | 63 | 9 (14%) | 56 (86%) | 65 | 0 | 66 (100%) | 66 |
| Follicular Carcinoma | 2 (11%) | 17 (90%) | 19 | 3 (16%) | 16 (84%) | 19 | 21 (91%) | 2 (9%) | 23 | 5 (22%) | 18 (78%) | 23 | 4 (17%) | 19 (83%) | 23 |
| Goiter | 4 (8%) | 47 (92%) | 51 | 14 (28%) | 36 (72%) | 50 | 49 (100%) | 0 | 49 | 33 (65%) | 18 (35%) | 52 | 11 (22%) | 38 (78%) | 49 |
| Thyroiditis | 6 (35%) | 10 (65%) | 16 | 11 (71%) | 5 (29%) | 16 | 16 (100%) | 0 | 16 | 6 (35%) | 10 (65%) | 16 | 6 (35%) | 10 (65%) | 16 |
| Follicular Adenoma | 1 (17%) | 5 (83%) | 6 | 4 (67%) | 2 (33%) | 6 | 6 (100%) | 0 | 6 | 5 (83%) | 1 (17%) | 6 | 4 (67%) | 2 (33%) | 6 |
Table 3: Percent and number of negative and positive VEGF-A, VEGF-A165b, VEGF-B, VEGF-C and VEGF-D expression cases among papillary carcinomas, follicular thyroid carcinomas, and follicular adenomas.
Despite the wide expression of VEGF-A in both carcinomas we have also observed a wide immunoexpression of VEGF-A165b, the anti-angiogenic splice variant. The immunohistochemical expression of VEGFs in the adjacent peritumoral thyroid tissue was always less intense and dispersed than the observed within the tumoral area. In relation to the VEGF-B immunoexpression we found only a few positive cases in both papillary and follicular carcinomas. The highest levels of VEGF-C and VEGF-D immunoexpression were founded in papillary carcinomas but almost all carcinomas of this study have expressed some level of VEGF-D (Table 3).
Immunohistochemical expression of VEGFs and the clinicopathological data correlation, when analyzed from 0 to ++++, demonstrated a statically relevant association of VEGF-D and a worst tumoral staging (p=0.004) in papillary carcinomas. Moreover, using the dichotomized evaluation (positive or negative immunoexpression), we also identified a weak, but statically relevant, association between VEGF-A and vascular invasion (p=0.049) and patient’s age and an increased expression of VEGF-B (p=0.047) in papillary thyroid carcinomas. Clinicopathological available data and the VEGFs immunoexpression of follicular carcinomas did not show significant statistical associations (Table 4).
| VEGF-A | VEGF-A165b | VEGF-B | VEGF-C | VEGF-D | |
|---|---|---|---|---|---|
| p | p | p | p | p | |
| Age | 0.852 | 0.447 | 0,047* | 0.642 | - |
| Gender | 0.454 | 0.793 | 0.326 | 0.168 | - |
| Side | 0.300 | 0.090 | 0.197 | 0.095 | - |
| Capsular Invasion | 0.654 | 0.518 | 0.207 | 0.359 | - |
| Vascular Invasion | 0,049* | 0.706 | 0.945 | 0.412 | - |
| Perithyroidal Soft Tissue Compromise | 0.309 | 0.793 | 0.355 | 0.433 | - |
| Metastasis | 0.428 | 0.936 | 0.298 | 0.648 | - |
| T | 0.707 | 0.263 | 0.671 | 0.949 | - |
| N | 0.763 | 0.794 | 0.723 | 0.758 | - |
| M | - | - | - | - | - |
| Staging | 0.905 | 0.582 | 0.809 | 0.321 | - |
| Follicular Carcinoma | |||||
| Age | 0.937 | 0.466 | 0.156 | 0.538 | 0.315 |
| Gender | 0.608 | 0.517 | 0.567 | 0.602 | 0.435 |
| Side | 0.266 | 0.439 | 0.704 | 0.515 | 0.093 |
| Vascular Invasion | 0.08 | 0.348 | 0.636 | 0.433 | 0.482 |
| Perithyroidal Soft Tissue Compromise | 0.725 | 0.656 | 0.752 | 0.052 | 0.639 |
| Metastasis | - | - | - | - | - |
| T | 0.811 | 0.354 | 0.706 | 0.791 | 0.89 |
| N | - | - | - | - | - |
| M | - | - | - | - | - |
| Staging | 0.597 | 0.440 | 0.558 | 0.780 | 0.275 |
Table 4: Comparison between VEGFs immunoexpression and clinicopathological features.
In benign lesions, goitres (92% of positive cases), follicular adenomas (83% of positive cases) and thyroiditis (65% of positive cases) were observed a widespread positive immunoexpression of VEGF-A. Positive immunoexpression of VEGF-A165b was also founded in goitre (72% of positive cases), follicular adenomas (33% of positive cases) and thyroiditis (29% of positive cases). The immunoexpression levels of VEGF-C and VEGF-D were generally lesser than those founded in the carcinomas. None of the benign samples of this casuistic had positive immunoexpression of VEGF-B (Figure 1).
The results of this study demonstrated significant differences in the expression of VEGFs family members among a varied of benign and malignant thyroid lesions, which were more evidently established when a dichotomized positive or negative score of immunohistochemical expressions was applied. Generally, the expression of VEGF family members have a tendency to be higher in malignant than in benign lesions. These findings corroborate previous studies that verified an increased expression of vascular endothelial growth factors, both angiogenic and lymphangiogenic, in thyroid neoplasms [13,19]; this also occur similarly in other types of malignancies such as, for example, lung, bladder, cervix, breast and kidney [20]. Taking together, our results have showed a gradual enhancement of the VEGFs proteins immunoexpression from the phenotypically normal thyroid tissue, benign proliferative lesions and malignant neoplastic areas. The associations between the immunoexpression of VEGFs and the clinicopathological data highlighted some significant correlations in papillary carcinomas.
Most VEGFs were widely and strongly immunoexpressed in both papillary and follicular carcinomas. In these neoplasms the number of cases with immuno-positive expression for VEGF-A, VEGF-A165b, VEGF-C and VEGF-D was higher than 75% reaching 100% of positive cases for VEGF-D in papillary carcinomas. Only VEGF-B showed a weak immunoexpression, with only 8% of positive cases in the papillary carcinomas and 9% in follicular carcinoma.
Both types of tumours have showed significant differences between the VEGF-A immunohistochemical expression in the neoplastic area when compared to its expression in areas of thyroiditis, goitre and morphologically normal adjacent tissue. This finding is relevant because higher expression of VEGF-A is often associated with tumour growth due to his potential contribution for providing nutrients for cell proliferation. In agreement with other articles in the literature, our study demonstrates that the levels of immunoexpression of VEGF-A in morphologically normal adjacent regions is lower than that found in the papillary and follicular neoplasms of the thyroid [21]. We demonstrate that almost 100% of papillary and follicular carcinomas showed immunohistochemical positive expression of VEGF-A in cancer cells. In contrast, 81% of papillary carcinomas and 84% of follicular carcinomas express VEGF-A165b, an isoform that inhibit angiogenesis [9]. So far we are not aware of any other paper that has described the participation of VEGF-A165b in thyroid neoplasms; this interesting observation may explain, at least in part, the indolent behaviour of most thyroid carcinomas and demonstrates the existence of a balance between pro and anti-angiogenic factors. We could not observe variations in the immunohistochemical expression of VEGF-A165b in different variants of papillary carcinoma. In adjacent tissues with phenotypically normal thyroid, goitre or thyroiditis VEGFs immunoexpression were always inferior to those found in the neoplastic region. Nevertheless, the expression of VEGF-A was quite expressive. Thyroiditis and goitre express high amounts of TSH (thyroid stimulating hormone), firstly because of the destruction of follicles, and secondly because of deficiency on thyroid hormone synthesis mostly caused by deficiency in iodine supply. Both changes lead to increased TSH, admittedly, an important regulator of VEGF-A expression [22]. This fact potentially explains the high levels of VEGF-A observed in adjacent regions of papillary and follicular carcinomas containing goitre and thyroiditis. Moreover, the high immunoexpression of the main mediator of angiogenesis, VEGF-A, is consistent with the significant increase in the neovascularisation observed in chronic inflammation and also with the fact of the thyroid, because of their endocrine functions, require a precise regulation of their microvasculature [23]. According to Klein and Catargi [23], thyroid inflammatory processes may be accompanied by the development of vasculature and increased vascular permeability, which explains the swelling usually observed in thyroiditis. In agreement with our findings, significant levels of VEGF-A expression in different etiologic thyroiditis types have been reported in the literature [24]. Angiogenesis mediated by VEGF-A is particularly related to inflammatory reactions as a whole, because inflammatory cytokines (including those involved with thyroiditis) are mediators of VEGF-A expression, such as for example interleukin-6 [25]. Although high levels of immunohistochemical positivity expression for VEGF-A were find in non neoplastic lesions, and even in morphologically normal tissues adjacent to thyroid papillary and follicular carcinomas, an important immunoexpression of VEGF-A165b was also found in these areas which can be speculate as part of the anti-angiogenic features that will oppose the angiogenic stimulus provided by VEGF-A.
The other members of VEGF family have had lesser impact in thyroid lesions. Interestingly, VEGF-B was expressed in only few cases of thyroid malignancies what could be further explored to explain such differences between benign and malignant lesions. Peritumoral thyroiditis also expressed VEGF-B but the tumour microenvironmental could be influencing this result. Tanaka et al. [14] reported VEGF-B mRNA activity in all 41 papillary carcinomas studied. VEGF-B is still poorly studied in comparison to the other members of VEGF family; little is known about it physiologic role in vivo [23] or its involvement in cancer [26,27]. Currently, VEGF-B expression in thyroid lesions is a controversial finding. VEGF-B is a non-hypoxia inducible VEGF family member and it seems not affect angiogenesis directly or vascular permeability; VEGF-B is believed to probably be a survivor factor for endothelial cells, pericytes and smooth muscle cells [27].
The VEGF-C expression shown in this study corroborated previous reports that observed that VEGF-C is more importantly expressed in papillary carcinoma than in other thyroid malignancies [15,28]. VEGF-C is the most important lymphangiogenic stimulation factor [1]. Its overexpression is consistently associated to lymph node invasion and distant metastasis [29,30]. However, the role of VEGF-C in thyroid carcinomas as prognostic marker is still disputable [17,31]. Similarly, VEGF-D expression was reported in thyroid carcinoma, mainly in those with papillary phenotype [16]. This is in agreement with our results that demonstrated that all papillary carcinomas and 83% of follicular carcinomas stained for VEGF-D. Non-neoplastic lesions were also decorated with VEGF-D, which limits its importance for prognostic proposals. Of interest, our results corroborates previous reports that showed higher expression of VEGF-D in papillary than in follicular carcinomas, which seems to be logical because papillary carcinomas preferentially metastasise through lymphatic conduits [23]. Additionally, VEGF-D expression is more likely correlated with augmented risk for lymph node invasion and distant metastasis [16,23].
Summarising, despite higher VEGF-A expression be commonly associated to the parameters of worse prognostic in literature, some controversial results were herein reported. First, as other reports, we did not find any important correlation between tumour size and more aggressive behaviour [13,32,33]; neither as an independent marker for lymph node invasion or distant metastasis [34]. Our findings corroborated those found by Huang and colleagues [35] that did not find any association between VEGF-A and tumour size, tumour extension, invasion and AGES (Patient’s age, tumour size, histological grade, tumoral extension and metastasis) or MACIS (metastasis, age, resection margin , invasion and tumour size). VEGF-A165b was importantly expressed in thyroid carcinomas and it seems act like a balance against the VEGF-A pro-angiogenic force. Since we still do not understand which and how factors induce the selection of those splicing variants the real meaning of this expression (in both benign and malignant cases) is still obscure and should be ratified in further studies.
We thank the supply of the histological samples by the histopathology laboratories of Sírio Libanês Hospital, Oswaldo Cruz Hospital CICAP, Diagnóstika Laboratory and the technical support of the Medical Research Laboratories 14 (LIM- 14) and 26 (LIM-26) of Faculty of Medicine of São Paulo University. The authors declare that there is no conflict of interest that would prejudice the impartiality of this scientific work.