Journal of Hematology & Thromboembolic Diseases
Open Access
ISSN: 2329-8790
![]() +44 1478 350008
+44 1478 350008
ISSN: 2329-8790
![]() +44 1478 350008
+44 1478 350008
Case Report - (2013) Volume 1, Issue 4
Reactive bone marrow plasmacytosis occurs in association with a variety of conditions. In such reactive cases, Plasma Cells (PCs) usually account for 10%-20% of cells in bone marrow trephine biopsy sections and rarely exceed 50%. Here in we report an unusual case of bone marrow aplasia associated with prominent atypical plasma cell proliferation and hypoplastic bone marrow.
Keywords: Plasma cells; Reactive plasmacytosis
Reactive bone marrow plasmacytosis occurs in association with a variety of conditions, such as chronic infections, autoimmune diseases, connective tissue and chronic granulomatous disorders, diabetes mellitus, hypersensitivity states, drug-related agranulocytosis, iron deficiency, megaloblastic and hemolytic anemia, hemopoietic and non-hemopoietic malignant diseases, angio-immunoblastic lymphadenopathy, and multicentric Castleman’s disease [1-3]. In such reactive cases, Plasma Cells (PCs) usually account for 10%-20% of cells in bone marrow trephine biopsy sections and rarely exceed 50% [3-5]. Herein we report an unusual case of bone marrow aplasia associated with prominent atypical plasma cell proliferation (96% of all nucleated cells exhibited transient pancytopenia) and hypoplastic bone marrow.
A 61-year-old woman presented to our clinic in July 2009 with complaints of sustained high fever, productive cough, and fatigue. One week earlier she was diagnosed by a general practitioner with acute pharyngitis and was given oral amoxicillin+clavulanate 2 g/day [1]. Despite antibiotic therapy her complaints exacerbated and general status deteriorated. The patient was re-evaluated by her physician and referred to our clinic, because of newly developing pancytopenia and signs of pneumonia. Her medical history was positive for diabetes mellitus type 2, which was diagnosed 15 years earlier, and regular use of oral antidiabetic drugs. She had similar complaints 3 years earlier and laboratory results that confirmed pancytopenia following acute tonsillitis and use of amoxicillin+clavulanate. Bone marrow examination was recommended at that time, but the patient declined.
Upon admission she was very pale, with tachycardia and fever. Axillary temperature was 38.5°C. Lymphadenopathy and organomegaly were not observed. Laboratory examination results were as follows: leukocyte count: 204×109/l with 76% lymphocytes; Hb: 8.7 g/dl; HCT: 26%; PLT: 10×109/l. Serum potassium level was 2.6 mmol/l and serum C-reactive protein was 31.79 mg/dl (normal: <0.5 mg/dl). Serology was negative for Epstein-Barr virus (EBV), Cytomegalovirus (CMV), parvovirus, and Human Immunodeficiency Virus (HIV). Serum globulin was 3 g/dl [1-5] and albumin was 2.7 g/dl. Serum level of IgG, IgA, and IgM was 844, 171, and 49 mg/dl, respectively. An increase in polyclonal immunoglobulin was observed based on serum immunoelectrophoresis.
Bone marrow was hypocellular for age, the cellularity-to-fat ratio was 1:3, granulocytic and erythroid cells and their precursors were low in number, and most of the cells observed in the biopsy specimen were plasma cells, some of which formed small interstitial aggregates, and lymphocytes were few in number. Bone marrow aspirate was also hypocellular and about 96% of the nucleated cells were plasma cells, mostly of mature morphology, but a small number of binuclear and atypical forms were also observed. Immunohistochemical analysis results of the biopsy specimen were as follows: CD138 highlighted the increased population of plasma cells, but kappa and lambda immunoglobulin light chain staining exhibited a polyclonal pattern; IgG, IgA, IgD, and IgM heavy chain-positive cells were polytypic; the number of CD20- and CD5-positive B- and T-lymphocytes didn’t indicate infiltration (Figure 1).
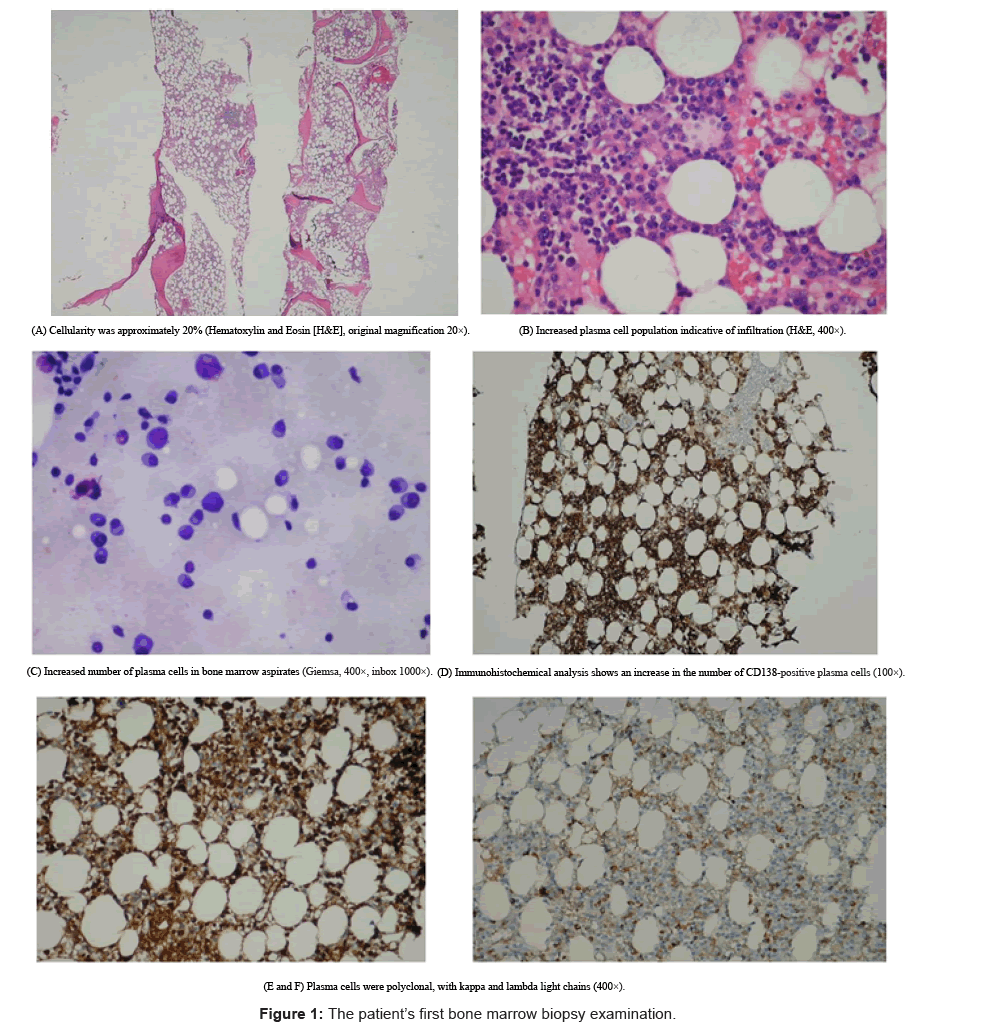
Figure 1: The patient’s first bone marrow biopsy examination.
Chest X-ray and thorax Computed Tomography (CT) showed evidence of pneumonic infiltrate in the left lower lobe. After blood, urine, and sputum cultures were obtained, the patient was treated with imipenem 5 μg/kg/day for febrile neutropenia and Granulocyte Colony-Stimulating Factor (G-CSF). Sputum culture was positive for Pseudomonas aeruginosa and urine culture was positive for Klebsiella pneumoniae.
During the course of hospitalization the patient’s fever resolved, which resulted in dramatic clinical improvement, and radiological findings markedly improved. After 3 weeks her leukocyte count increased to 4500×103/mm3, Hb was 9.9 g/dl, HCT was 29.7%, and platelet count was 101×103/mm3. Follow-up bone marrow biopsy results, performed 3 weeks after admission, were hypercellular for age; in particular, granulocytic cells and their precursors increased in number, as did erythroid and megakaryocytic cells. In bone marrow aspirate the plasma cell rate was about 5%-7%, which resulted in polytypic immunophenotyping for kappa and lambda light chains (Figure 2).
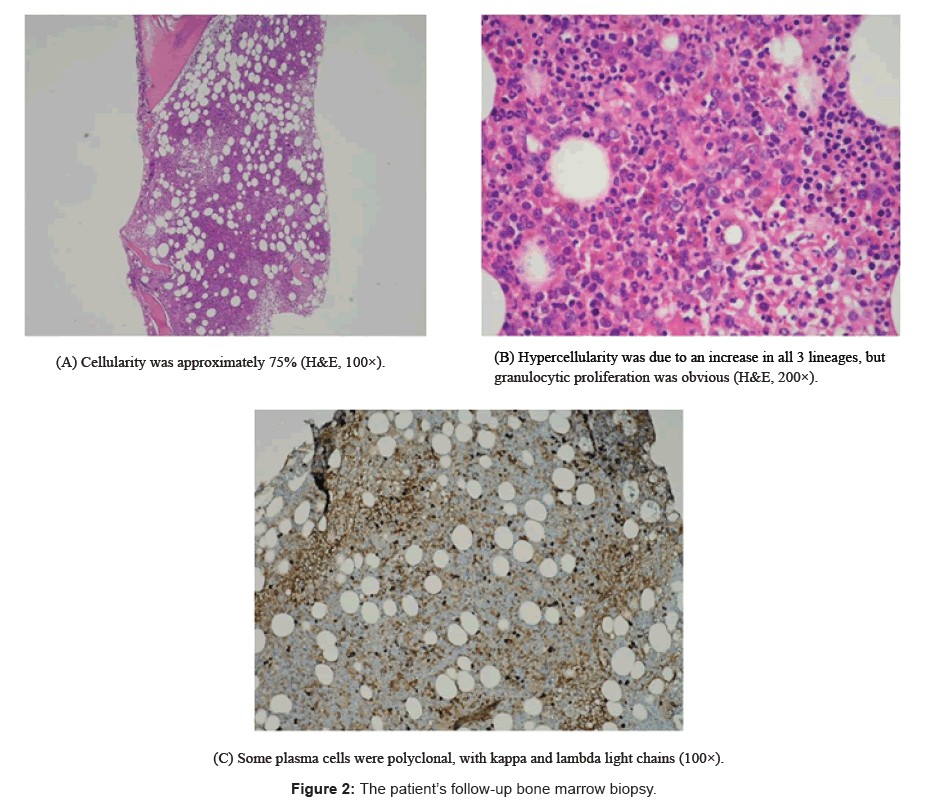
Figure 2: The patient’s follow-up bone marrow biopsy.
The patient presented with pancytopenia and hypoplasia; bone marrow was infiltrated by plasma cells at the rate of 96%. Although plasma cell dyscrasias were diagnosed based on morphological findings, protein electrophoresis and bone marrow immunohistological examination showed polyclonal protein restriction in both reactive processes. Generally, reactive plasma cell proliferation seen in bone marrow does not exceed 20%. In the presented case we observed a plasma cell increase of approximately 80%-90%, which is unusual. The literature contains 2 pediatric cases of Acute Lymphoblastic Leukemia (ALL) following polyclonal B-cell proliferation, pancytopenia, and bone marrow aplasia. Whitlock and Mc Curley [6] described these findings as newly developing chromosomal anomalies. Chromosome anomalies and growth factor-associated gene changes may explain both pancytopenia and ALL, but they do not clarify the association between B-cell proliferation and ALL. Finlay et al. [7] reported an ALL case with pancytopenia and polyclonal B-cell proliferation following chronic, persistent EBV infection. The patient’s EBV infectionassociated polyclonal lymphoproliferative status was the main cause of insufficient immunity and the development of ALL. To the best of our knowledge the same characteristics in an elderly patient have not been reported.
The presented case didn’t have any clinical or laboratory abnormalities during 2 years of post-treatment follow-up. According to her medical history, 3 years earlier she had similar complaints, which may have been related to viral infection, secondary to bacterial infection, or amoxicillin+clavulanate-related polyclonal plasma proliferation and immunological response. Some types of infection and abnormal immune reactions are characterized by a marked proliferation of plasma cells; however, the pathogenesis of reactive polyclonal plasma cell proliferation is uncertain [8]. When these 2 reactive processes present with pancytopenia and B-cell proliferation it may be a sign of lymphoproliferative disease or other hematological malignancies, and such patients should be followed up closely.