Journal of Cancer Science and Research
Open Access
ISSN: 2576-1447
ISSN: 2576-1447
Research Article - (2018) Volume 3, Issue 1
Background: TC (a combination of 75 mg/m2 docetaxel and 600 mg/m2 cyclophosphamide q3W) is used for neoadjuvant/adjuvant chemotherapy in the treatment of primary breast cancer. We have recently encountered many cases of skin eruption related to TC therapy, but the effectiveness of prophylactically using anti-allergic drugs remains unclear. In this study, we aimed to determine whether the prophylactic use of anti-allergic drugs could be beneficial for the prevention of TC-related skin toxicity.
Methods: We retrospectively investigated the incidence of skin eruption related to TC or a combination of docetaxel, cyclophosphamide, and trastuzumab (HER-TC) among patients with or without prophylactic anti-allergic drug administration by performing a sub-analysis of data from a previous clinical trial. For neoadjuvant chemotherapy (NAC), four cycles of either TC or HER-TC (docetaxel: 75 mg/m2; cyclophosphamide: 600 mg/m2; trastuzumab: 6 mg/kg loading dose, then 8 mg/kg thereafter) were administered intravenously every 3 weeks. 120 mg per day of fexofenadine (an antihistamine) was administered from the first day of TC or HER-TC treatment until three weeks after completion of the four cycles of TC/HER-TC treatment.
Results: Four cycles of TC or HER-TC therapy were administered to 94 patients. The incidence of skin eruption with and without prophylactic drug administration was 27.7% (26/38) and 10.6% (10/56), respectively, indicating that prophylactic anti-allergic drug usage did not decrease the incidence of skin eruption.
Conclusions: Administration of prophylactic anti-allergic drugs may not be useful for prevention of TC- or HERTC– related skin eruption.
Keywords: Breast cancer; TC or HER-TC Therapy-related skin eruption; Anti-allergic drugs; Neoadjuvant chemotherapy
We retrospectively investigated the incidence of skin eruption related to TC or a combination of docetaxel, cyclophosphamide, and trastuzumab (HER-TC) among patients with or without prophylactic anti-allergic drug administration by performing a sub-analysis of data from a previous clinical trial. Administration of prophylactic antiallergic drugs may not be useful for prevention of TC- or HER-TC– related skin eruption.
The US Oncology 9735 trial was the first randomized controlled trial to directly compare the efficacy of anthracycline- and taxane-based postoperative adjuvant chemotherapy regimens in breast cancer, and the results of the analysis after a median of 7 years of follow-up have now been reported [1]. The results showed that docetaxel/cyclophosphamide (TC) adjuvant regimens resulted in superior overall survival rates than those achieved with anthracycline/cyclophosphamide (AC) adjuvant regimens in breast cancer patients. TC therapy was also shown to be superior to AC therapy regardless of patient age, hormone receptor status, and lymph node status. Thus, TC has recently been established as a standard adjuvant chemotherapy regimen for operable breast cancer [2].
TC and HER-TC are well known to cause skin eruption, indicating that they have a degree of non-hematological toxicity. However, the cause of this toxicity is unclear, and reliable treatment methods have not yet been established. As a result, prophylactic methods to prevent TC/ HER-TC–related skin eruption are urgently needed. Anti-allergic drugs are sometimes administered to treat skin eruption, but their prophylactic effectiveness has not yet been investigated. We hypothesized that the prophylactic use of anti-allergic drugs would decrease the incidence of TC/HER-TC-related skin eruption. We have already reported the efficacy and tolerability of TC neoadjuvant chemotherapy (NAC) and HER-TC NAC in patients with breast cancer in previous studies [3,4]. Therefore, in this work, we re-analyzed the data from those studies to retrospectively evaluate the prophylactic effectiveness of anti-allergic drugs against TC/HER-TC–related skin eruption among the patients in our clinical trial.
The objective of our study was to evaluate the efficacy of prophylactic anti-allergic drug administration against TC-related skin eruption in patients with primary breast cancer. This study is a subanalysis of data that we previously reported as part of a combined phase 2 study of TC NAC and HER-TC NAC [3,4]. This study was an openlabel, nonrandomized study, which was conducted at seven different institutions.
Patient Eligibility
Patients eligible for inclusion in this study were women who were 20-70 years old with stage I, II, or III breast cancer (1-7 cm; stage N0, N1, and M0) that had an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. Patients with T1a or T1b stage tumors were ineligible for inclusion. All patients were diagnosed as having invasive breast cancer by a core needle or Mammotome biopsy before treatment. Estrogen receptor (ER) and progesterone receptor (PgR) expression was assessed using immunostaining. A positive result was defined as staining of 10% or more of the cells. The HER2 status of the patients was assessed using the HercepTest (DakoCytomation, Glostrup, Denmark). A score of <2 was considered negative and a score of >3 was considered positive. In patients with a HercepTest score between 2 and 3, the HER2/neu amplification rate was determined via fluorescence in situ hybridization, and a ratio greater than 2.2 was considered to indicate HER2 positivity. This study was approved by the Institutional Review Board of Kyoto Prefectural University of Medicine (Kyoto, Japan) on March 19, 2012, and was conducted in accordance with the Helsinki Declaration of 1975, as revised in 1983. All patients provided written, informed consent before their enrollment in the study. A diagram showing patient enrolment is shown in Figure 1.
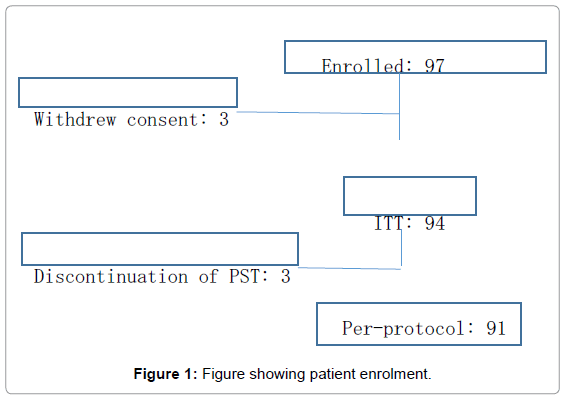
Figure 1: Figure showing patient enrolment.
Treatment plans
The patients were premedicated with 5-hydroxytryptamine-3 receptor antagonists and corticosteroids. Then, standard doses of docetaxel (75 mg/m2) and cyclophosphamide (600 mg/m2) with or without trastuzumab (loading dose 8 mg/kg, followed by 6 mg/kg every 3 weeks) were administered every 21 days for four cycles. In addition, 120 mg per day of fexofenadine (an antihistamine) was administered in some patients at the attending physician’s discretion from the first day of TC or HER-TC treatment until three weeks after completion of the four cycles of TC/HER-TC treatment. A blood test was performed on the first day of administration and the criteria for initiating administration were a white blood cell count of ≥ 3000/mm2, a neutrophil count of ≥ 2000/mm2, a platelet count of ≥ 100,000/mm2, a hemoglobin level of ≥ 9.0 mg/dL, a creatinine level of ≤ 1.5 mg/dL, a total bilirubin level of ≤ 1.5 mg/dL, and a normal electrocardiogram.
During the treatment regimen, the doses of docetaxel and cyclophosphamide were reduced if either of the following adverse reactions was noticed in a previous administration cycle: (1) febrile neutropenia (FN; a fever of 38°C or higher with a neutrophil count of less than 1000/mm2 that persists for more than 3 days) or (2) grade 3 or severe non-hematological toxicity. The dose levels of docetaxel and cyclophosphamide were reduced to 60 mg/m2 and 500 mg/ m2, respectively. Only one dose reduction was allowed for docetaxel and cyclophosphamide, and no dose reduction was allowed for trastuzumab. The protocol was discontinued in patients who continued to experience adverse reactions despite the dose reduction. Adverse reactions were classified and graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events ver. 3.0. Granulocyte colony-stimulating factor and preventive oral antibiotics were administered during the treatment regimen at the attending physician’s discretion.
We used Fisher’s exact test and a chi-square test to analyze the data, and p values less than 0.05 were considered statistically significant.
Patient characteristics
The clinicopathological characteristics of the patients are shown in Table 1. The median age was 52 years (range, 32-72 years); all patients had an ECOG performance status of 0; 37.2% were premenopausal; 51.1% were estrogen receptor positive; 34.0% were progesterone receptor positive; and 44.7% were HER2 positive. None of the characteristics was significantly different between the group with prophylactic administration and that without, according to the chi-square test.
| Patients with prophylactic administration* (n=38) | Patients without prophylactic administration* (n=56) | All patients (n=94) | p value | |
|---|---|---|---|---|
| Age | ||||
| Median | 52 | 54 | 52 | 0.217 |
| Range | 32-72 | 38-70 | 32-72 | |
| Stage, no. (%) | ||||
| Ⅰ | 3 (7.9) | 6 (10.7) | 9 (9.6) | 0.863 |
| Ⅱ | 27 (71.1) | 42 (75.0) | 69 (73.4) | |
| Ⅲ | 8 (21.0) | 8 (14.3) | 16 (17.0) | |
| Menopausal status, no. (%) | ||||
| Premenopause | 12 (31.6) | 23 (41.1) | 35 (37.2) | 0.35 |
| Postmenopause | 26 (68.4) | 33 (58.9) | 59 (62.8) | |
| ER, no. (%) | ||||
| Positive | 23 (60.5) | 25 (44.6) | 48 (51.1) | 0.569 |
| Negative | 15 (39.5) | 31 (55.4) | 46 (48.9) | |
| PgR, no. (%) | ||||
| Positive | 13 (34.2) | 19 (33.9) | 32 (34.0) | 0.977 |
| Negative | 25 (65.8) | 37 (66.1) | 62 (66.0) | |
| HER2, no. (%) | ||||
| Positive | 20 (52.6) | 22 (39.3) | 42 (44.7) | 0.202 |
| Negative | 18 (47.4) | 34 (60.7) | 52 (55.3) | |
120 mg per day of fexofenadine (an antihistamine) was administered from the first day of TC or HER-TC treatment until three weeks after completion of the four cycles of TC/HER-TC treatment.
Table 1: Clinico-pathological characteristics of the patients.
Skin toxicities
The skin toxicities of the treatments were originally analyzed with the intention of treating the patients. The incidence of skin eruption events is summarized in Table 2. Grade 1 or 2 hand skin disorders (HSD) and facial erythema (FE) occurred in 20 (21.3%) and 14 (14.9%) of the patients, respectively. By contrast, grade 3 or 4 HSD and FE both occurred in only one patient (1.1%). One patient with HSD experienced grade 3 skin pain after three cycles of TC, and another patient with FE developed severe facial urticaria after two cycles of TC. Treatment was discontinued for these patients as per their wish. The occurrence of skin eruption in patients that were administered prophylactic anti-allergic drugs and those that were not is summarized in Table 3. As shown, the use of prophylactic anti-allergic drugs did not decrease the incidence of skin eruption. Instead, there was no significant difference between the incidences of skin eruption with and without administration of prophylactic drugs (p value=7.46).
| Total (n=94) | ||
|---|---|---|
| Grade 1 or 2, n (%) | Grade 3 or 4, n (%) | |
| HSDa | 20 (21.3) | 1 (1.1) |
| FEb | 14 (14.9) | 1 (1.1) |
| Total | 34 (36.2) | 2 (2.2) |
aHSD: hand skin disorders; bFE: facial erythema
Table 2: Incidence of skin eruption events.
| Patients with prophylactic administration | Patients without prophylactic administration | All patients | |
|---|---|---|---|
| (n=38) | (n=56) | (n=94) | |
| Patients with skin eruption | 26 (27.7) | 10 (10.6) | 36 (38.3) |
| Patients without skin eruption | 12 (12.8) | 46 (48.9) | 58 (61.7) |
a p value=7.46
Table 3: Skin eruption in patients with or without administration of prophylactic antiallergic drugsa.
The typical photos of HSD and FE were shown in Figure 2. The cumulative incidence of skin eruption every chemotherapy cycle is summarized in Figure 3. As shown in Figure 3, the onset of skin eruption mostly occurred after one or two cycles.

Figure 2: Typical photos of hand skin disorders (HSD) and facial erythema (FE).
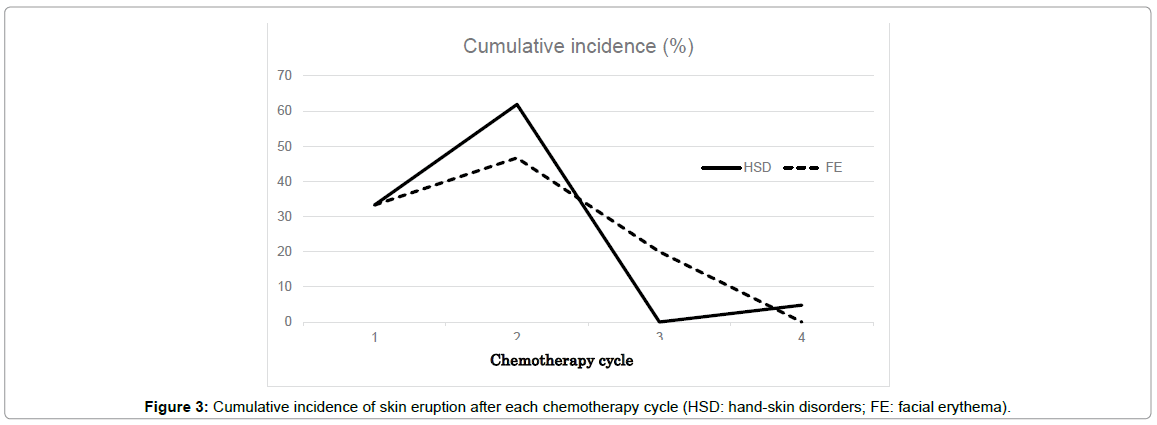
Figure 3: Cumulative incidence of skin eruption after each chemotherapy cycle (HSD: hand-skin disorders; FE: facial erythema).
Some of the side effects of TC/HER-TC therapy, such as febrile neutropenia and myelosuppression, are well managed with supportive therapy. Others, such as cutaneous reactions of the skin and leg edema, are relatively under-researched and neglected in clinical practice, despite their recognized impairment of cancer patients’ quality of life [5,6]. Thus, in recent years, non-hematologic toxicities have become more clinically important. In two Japanese reports, the incidence of skin eczema during TC/HER-TC therapy was reported to range from 54.8% to 65.6% [7,8]. However, the incidence of skin toxicity in docetaxel monotherapy is only reported to range from 20% to 48% [6,9-11], suggesting that the combination of docetaxel with cyclophosphamide increases the risk of eczema [12]. We have recently encountered many cases of TC/HER-TC–related HSD and FE. HSD, also known as palmar-plantar erythrodysesthesia, is a more severe skin reaction related to docetaxel, as well as other cytotoxic chemotherapy agents. This syndrome includes a prodrome of dysesthesia, a tingling sensation in the palms and soles, and progresses to a bilateral, symmetric, burning pain with swelling and erythema that may occasionally extend beyond the palmar and plantar regions. As shown in Figure 2, HSD did not occur after three or more cycles, but FE occurred even after three cycles; therefore, the mechanisms of HSD and FE may be different. However, little is known about the mechanisms of these syndromes.
In Japan, two reports have been published regarding TC therapyrelated toxicities [13,14]. One indicated that H2 blockers, especially lafutidine, significantly increased the incidence of HSD and FE. However, H2 blockers were not administered to any of the patients in our study. The other indicated that patients receiving cyclophosphamide prior to docetaxel were at an increased risk of rash/eczema. Cyclophosphamide was administered prior to docetaxel in all of the patients in our study; therefore, if we administer docetaxel prior to cyclophosphamide, we may be able to decrease the incidence of skin eruption in the future.
At present, effective preventive methods for TC or HER-TC-related skin eruption have not yet been established. McCarthy et al. reported that cryotherapy in the form of frozen gloves did not appear to reduce the incidence, severity, or time-to-onset of hand and nail toxicity associated with docetaxel [15]. In addition, this work did not indicate any benefit of prophylactic administration of anti-allergic drugs; hence, we would not recommend the routine use of prophylactic drugs for all patients who undergo TC or HER-TC therapy.
Although the findings of this study are important, this study has several limitations. The first limitation is that this is a retrospective study; thus, we were limited by the data available and were unable collect additional data to aid our investigation. However, initiating a new clinical trial to investigate TC-related skin toxicity would have been extremely costly and time-consuming. Therefore, we feel that a retrospective study was the best option in this case. The second limitation is the small sample size and nonrandomized design of the clinical study on which this analysis was based. A larger sample size and a randomized design could have provided more reliable results. However, it was not possible to ensure this retrospectively. The final limitation of our study is that a centralized dermatology review was not performed, as we felt that this was beyond the scope of this investigation. A more extensive review of the literature could provide additional data to support our findings in the future.
In conclusion, this study demonstrated that administration of prophylactic anti-allergic drugs may not be useful for preventing TCrelated skin eruption.
The authors have no conflicts of interest to declare.