Journal of Probiotics & Health
Open Access
ISSN: 2329-8901
ISSN: 2329-8901
Research Article - (2015) Volume 3, Issue 1
Constipation is one of the most serious problems concerning the care of mentally and physically handicapped people in nursing homes in Japan. The major causes of constipation are related to their physical abnormality. Therefore, Glycerol Enema (GE) is used to treat constipation. However, the administration of GE not only causes mental and physical stresses to handicapped people but also causes physical damage to nurses. Therefore, we explored whether the probiotic effect of Kefir-fermented milk can prevent constipation. We selected eleven participants, who have suffered from severe constipation. They did not show Bowel Movements (BMs) without the administration of GE. Kefir was taken three times a day for three months, and the numbers of BM and GE were investigated. Here, we found that four of the eleven participants showed improvement in BMs without the administration of GE. This study was carried out with the highly limited number of subjects, our results implicated that the adding of Kefir to the daily diet of handicapped people might have benefit for constipation prophylaxis. For future, we must investigate with the larger number of subjects to understand the effect of Kefir for preventing constipation. Even though further investigation is required, our study suggests that to add the oral intake of Kefir would contribute to the reduction of the physical labor of nurses spending much time and effort for the administration of GE, and also contribute to an increase in the quality of life for handicapped people.
Keywords: Constipation; Handicapped person; Probiotics; Dietary regimen; Enema
In Japan, many handicapped people staying in nursing homes and medical centers for mentally and physically handicapped people suffer from severe constipation due to one or more causes related to or stemming from their handicap(s). For example, most handicapped people in our hospital are incapable of doing enough exercises to activate their Gastro-Intestinal (GI) systems [1,2]. Some possess dysplasia and/or dysfunction of the GI system. Many of the handicapped people staying in our hospital have eating disabilities requiring that their food be processed to a paste. People with severe eating disabilities often use gastric or intestinal fistula, and such fistula may be yet another cause of constipation. Constipation is also one of the side effects of medicines taken for epilepsies and/or other illnesses [3,4]. Thus, handicapped people may have several specific causes of constipation, combining to result in severe constipation. To prevent and treat constipation, various kinds of aperients and enema agents are administrated to patients in Japan. The administration of an enema agent, typically a Glycerol Enema (GE), is the typical solution for the treatment of constipation in Japan, but this often causes a lot of problems. First, the administration of GE causes mental and physical stresses for patients. For example, patients, particularly those ranging in age from teenage to young adults, are quite burdened due to the embarrassing procedure. Also, chronic administration may increase the risk of unexpected side effects and/or physical damage in the GI system. Second, the administration of GE also causes physical stresses for administrators and their supporters. In our hospital, two or three nurses are needed to support the administration of GE per handicapped patient. The work of these supporters is to hold and carry the patient, and this effort continues until all constipated patients have been administered a GE. Therefore, some nurses in our hospital have to spend several hours a day for the physically demanding support of the administration of GE. Because of this, supporting nurses often injured their backs and knee(s) [5,6]. While this possibility of physical damage to nurses administering GE is significant, the assigning of three nurses for each GE procedure is also inefficient from the standpoint of a nurse manager. Third, these GE treatments cause an increase in medical expenses. Once a GE is administered, it continues for the rest of the patient’s life. In Japan, the budgets for medical costs in public nursing homes and medical centers for handicapped persons are quite limited and tight. Therefore, it is important to investigate more cost-efficient alternative methods for constipation prophylaxis.
To overcome these problems of stress to patients, supporters and hospital budgets, we have investigated the effects of various dietary regimens. We have previously examined the effects of dietary fibers, herbal teas, and so on. However, none of these were successful in our hospital. As a next strategy, we started to investigate the probiotic effect of fermented milk because it is well known that taking fermented-milk products can improve GI function and prevent diarrhea as well as constipation [7-9]. Among various fermented milk products, we focused attention on Kefir-fermented milk, which is part of the traditional diet in the northern Caucasus, Georgia, and is made with Kefir grains composed of yeasts and lactic acid bacteria in a matrix of proteins, lipids, and polysaccharides [10,11]. The reason why we are particularly interested in Kefir is that Kefir might not only improve GI function, but also have additional benefits for health. One benefit is that Kefir was capable of assisting lactose digestion [12]. Another merit is that Kefiran, a polysaccharide on lipids of Lactobacillus kefiranofaciens , which is one of the components of Kefir grain, could suppress an increase in blood pressure and decrease in serum cholesterols in rats [13]. In addition to its benefits for health, lyophilized Kefir is also available to use in probiotics [14]. Since some handicapped people have eating-disabilities, it is preferable that the supporters can select from several options for feeding. In the case of Kefir, the supporters can choose from among liquid, solid, and lyophilized products.
In this study, we investigated whether the oral intake of Kefirfermented milk could prevent constipation for handicapped persons, resulting in the reduction of GE procedures. To address this possibility, lyophilized Kefir-fermented milk was given orally to study participants for three months, and the number of BM and GE were investigated in the double-blind crossover examination.
Participants
We chose 11 people that have difficulty with BM without the administration of GE in our hospital. The requirement of the administration of GE for BM is nearly 100%. Therefore, doctors in our hospital constantly administrate the GE on every 2 to 4 day, depended on the individuals. For this study, approvals of ethics committees in Beppu Developmental Medical center (approval number: 2012-1) and Oita University (approval number: 692) were obtained, and informed consent was received in the presence of each participant’s family. The details of medical care for the participants, such as age, gender, height, weight, dietary intake, water intake, diagnosis, nursing status, and drug(s) used in habit were summarized in Table 1.
| ID | Age | Sex | Height | Weight | Dietary intake | Water intake | Diagnosis | Nursing status | Drugs used in habit | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (yr) | (cm) | (kg) | (kcal) | (ml) | ACA | AEA | LA | APU | Lax 1 | Others | ||||
| A-1 | 70 | M | 145 | 42 | 1100 | 1125 | Epilepsy | Total assistance | ○ | ○ | ○ | ○ | ○ | |
| Mental retardation | ||||||||||||||
| A-2 | 58 | M | 145 | 39.8 | 1000 | 925 | Klinefelter syndrome | Total assistance | ○ | ○ | ○a | ○ | ||
| Epilepsy | ||||||||||||||
| Mental retardation | ||||||||||||||
| A-3 | 28 | F | 156 | 38.7 | 1500 | 800 | Epilepsy | Total assistance | ○ | ○a | ○ | |||
| Sequelae ofmeningitis | ||||||||||||||
| Hydrocephalus | ||||||||||||||
| A-4 | 28 | M | 151 | 51.9 | 1200 | 800 | Cerebral palsy | Walking with support | ○ | ○ | ||||
| Epilepsy | ||||||||||||||
| Esophageal hiatus hernia | ||||||||||||||
| A-5 | 27 | F | 143 | 41.1 | 1400 | 800 | Cerebral palsy | Unsteady walking | ○ | ○ | ||||
| Epilepsy | ||||||||||||||
| A-6 | 26 | M | 149 | 38.2 | 1600 | 1000 | Mental retardation | Operating a whole chair | ||||||
| B-1 | 65 | M | 139 | 39.5 | 1200 | 800 | Mental retardation | Total assistance | ○ | ○b | ||||
| Gastric ulcer | ||||||||||||||
| Sequelae of encephalitis | ||||||||||||||
| B-2 | 57 | M | 162 | 52.6 | 1000 | 950 | Down syndrome | Total assistance | ○ | ○ | ○c | |||
| Sequelae of arsenic poisoning | ||||||||||||||
| B-3 | 44 | F | 150 | 44.9 | 1200 | 800 | Cerebral palsy | Total assistance | ○ | ○ | ○a | ○ | ||
| Epilepsy | ||||||||||||||
| B-4 | 30 | M | 160 | 48.9 | 1500 | 1000 | Epilepsy | Operate a whole chair | ○ | ○ | ○c | |||
| Callosaldysgenesis | ||||||||||||||
| B-5 | 27 | F | 131 | 32.3 | 1400 | 800 | Epilepsy | Walk on knees | ○ | ○ | ○b | |||
| Microcephalus | ||||||||||||||
| Mental retardation |
Table 1: Information of participants. AC: an anticonvulsant agent, AE: an antiepileptic agents, LA: a lapactic agent, APU: an agent for peptic ulcer, Lax: laxative 1Some individuals were administrated sodium picosulfate (Laxoberon) as a laxative. aThese were administrated sodium picosulfate every day,bThese were administrated sodium picosulfate every four day, these were administrated sodium picosulfate every three day.
Lyophilized Kefir-fermented milk and powdery milk
Lyophilized Kefir-fermented milk was used in this study. Lyophilized Kefir-fermented milk was prepared by Nippon Kefir Co. ltd. (Fujisawa, Japan). In Kefir, Lactobacillus delbrueckii subsp. bulgaricus , L. helveticus, L. kefiranofaciens subsp. kefiranofaciens, L. kefiranofaciens subsp. Kefirgranum , L. acidophilus, Lactococcus lactis subsp. lactis , L. lactis subsp. cremoris and Streptococcus thermophilus have been identified in kefir grains, and Lactobacillus kefiri , L. parakefiri , L. fermentum and L. brevis have been identified in the fermented beverage [15]. As a control, powdered milk ‘Gun-Gun’, a baby formula produced by Wokodo Co. ltd, Tokyo, Japan, for infants 9 months and older was used. 100 g of the powdered milk ‘Gun-Gun’ contains: total energy is 475 kcal; 14.4 g of proteins; 20.0 g of fat; 2.7 g of linoleic acids; 59.9 g of carbohydrates; 200 mg of sodium; 360 mg of vitamin A; 0.7 mg of vitamin B1; 0.8 mg of vitamin B2; 0.5 g of vitamin B6; 1.5 μg of vitamin B12; 50 mg of vitamin C; 5 μg of vitamin D; 6 mg of vitamin E; 10 μg of vitamin K; 5.3 mg of niacin; 80 μg of folic acids; 5 mg of pantothenic acids; 650 mg of calcium; 400 mg of phosphoric acids; 9.5 mg Ion; 680 mg of potassium; 65 mg of magnesium; 230 mg of phospholipids; 6 mg of nucleic acids; 1 g of oligosaccharides; 500 mg of chlorides; 30 μg of β-Carotene; 0.3 g of α-linolenic acid; and 50 mg of docosahexaenoic acid.
Examination of the effect of Kefir-fermented milk on the constipation prophylaxis
The examination was double-blindly performed with the cooperation of a nutritionist in our hospital. The nurses responsible for supporting the meals of handicapped people could obtain either Kefir or powdery milk blindly from a nutritionist. Before we started the oral administration of either Kefir or powdered milk formula, the BM and GE status of each participant was recorded for 30 days. This information was used to show ‘pretreatment’. Then 11 participants were divided into 2 groups; 6 participants in Group A and 5 participants in Group B as shown in Table 1. In the beginning, participants in Group A were administered 2 g of lyophilized Kefirfermented milk after meals (3 times per day; total 6 g per day) for 3 months. As a negative (placebo)-control, participants in Group B were administered 2 g of powdered milk formula after meals (3 times a day; total 6 g per day) for 3 months. To enhance the probiotic effect of Kefir, participants in Group A started to drink Oligo-One, which contains 3 g of oligosaccharide of lactose (H+B Life Co., Ltd., Tokyo, Japan), during the last 40 days of their Kefir-treatment period. Since the intake of Oligo-one is once a day, participants took 3 g of oligosaccharides. After 3 months, participants in Group A stopped taking Kefir and started to take powdered milk formula, while participants in Group B stopped taking powdered milk formula and started to take Kefir and then also Oligo-One in the last 40 days of the Kefir-treating period. During the entire period of examination, the BM and GE statuses of all participants in both Group A and Group B were recorded. In case the intake of Kefir showed the 25% reduction of the BM without administration of GE compared to pretreatment and Placebo control, we judged these are ‘Slightly effective’. In case the intake showed more than 50% improvement we judged these were ‘Effective’, and showed more than 75%, we judged these were ‘Very effective’. Some individuals have taken laxatives in habit before we start this study. These kept taking laxatives during all periods of investigation, including pretreatment. The results were statistically analyzed with Fischer’s exact test to see whether Kefir stimulates BM without GE.
To investigate whether the intake of Kefir can prevent constipation, Kefir-fermented milk was administrated to participants who suffer from severe constipation. Before we started the administration of Kefir, the number of BM and GE were investigated for one month, as a pretreatment control. We confirmed that most of the participants barely showed BM without administration of GE (Figure 1). After the investigation of pretreatment, the administration of Kefir was started. To increase the accuracy of the effect of Kefir-fermented milk on constipation prophylaxis of the small number of participants, a crossover examination between lyophilized Kefir and powdery milk was done (Figure 1a). Since participants in this study used to be administrated GE every 2 to 4 days, we aimed to observe more than 20 times of administration periods, at least more than 80 days. Either lyophilized Kefir or powdery milk was administered to the participants after each of their meals, for a total of three times per day. To perform the double-blind examination, the nutritionist prepared individual packages of Kefir and powdery milk and passed them to the nurses who were responsible for the administration to participants. Participants were divided into two groups (Table 1), and people in Group A took Kefir first and people in Group B took powdery milk first as a placebo control for three months. In Figure 1, Blue bars represented the percentages of the requirement of the administration of GE for BM, and red bars represented the percentages of BM without administration of GE. In Tables 2 and 3, the percentages of requirement of the administration of GE for BM, and the percentages of relative improvement were represented. Participant A-1 and A-2 in Group A immediately showed frequent BM without administration of GE compared to their results in pretreatment (Figure 1b and Table 2). However, the rest of the participants in Group A did not show any improvement from the intake of Kefir (Figure 1b and Table 2). Therefore, we judged that the intake of Kefir for the participant A-1 and A2 was ‘Very effective’ and ‘Effective’, respectively. While, the rest of the participants in Group A were ‘not effective’. In contrast, participant B-1, B-2, and B-5 in the placebo-control group did not show any difference, but two, B-2 and B-3, of the five participants in Group B showed the slight improvement of BM after the intake of powdery milk (Figure 1b and Table 3).
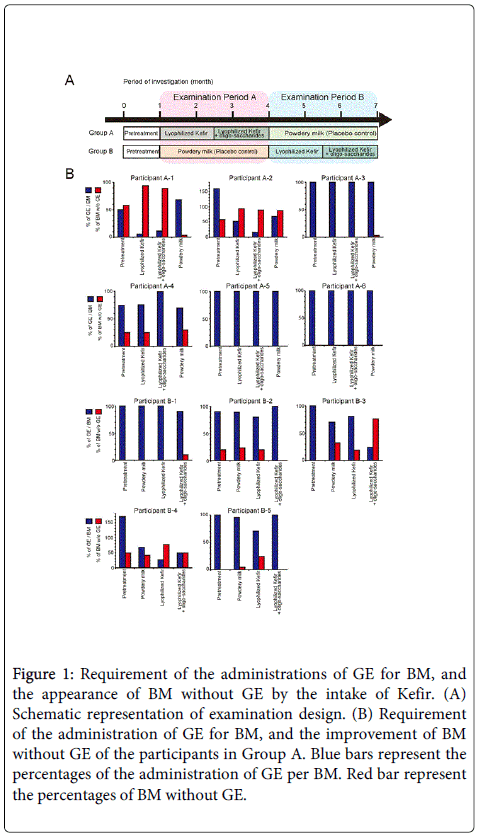
Figure 1: Requirement of the administrations of GE for BM, and the appearance of BM without GE by the intake of Kefir. (A) Schematic representation of examination design. (B) Requirement of the administration of GE for BM, and the improvement of BM without GE of the participants in Group A. Blue bars represent the percentages of the administration of GE per BM. Red bar represent the percentages of BM without GE.
| Participant | Percentages of the requirement of GE-administration for BM. 1( ) Percentages of improvement compared to pretreatment |
|||
|---|---|---|---|---|
| Pretreatment | Kefir | Kefir+Oligosaccharide | Powdery milk | |
| A-1 | 50 | 5.6 (89) |
11 (78) |
68 (-36) |
| A-2 | 160 | 52 (68) |
16 (90) |
15 (91) |
| A-3 | 100 | 100 (0) |
100 (0) |
100 (0) |
| A-4 | 75 | 76 (-1.3) |
100 (-33) |
70 (6.7) |
| A-5 | 100 | 100 (0) |
100 (0) |
100 (0) |
| A-6 | 100 | 100 (0) |
100 (0) |
100 (0) |
| Participant | Percentages of the requirement of GE-administration for BM. 1( ) Percentages of improvement compared to pretreatment 2[ ] Percentages of improvement compared to Powdery milk |
|||
|---|---|---|---|---|
| Pretreatment | Powdery milk | Kefir | Kefir+Oligosaccharide | |
| B-1 | 100 | 100 (0) |
100 (0) [0] |
90 (10) [10] |
| B-2 | 90 | 89 (1.1) |
80 (11) [12] |
100 (-11) [-12] |
| B-3 | 100 | 70 (30) |
81 (19) [-16] |
24 (76) [61] |
| B-4 | 170 | 68 (60) |
27 (84) [60] |
50 (71) [26] |
| B-5 | 100 | 96 (1.0) |
71 (29) [26] |
100 (0) [-6.3] |
Table 3: Investigation of the number of BM with or without administration of GE in the group B. 1( ) Percentages of improvement compared to pretreatment showed 25-50 represents ‘slightly effective’; 50-70 represents ‘effective’; and more than 75 represents ’Very effective’. Minus number represents the negative effect. 2[ ] Percentages of improvement compared to pretreatment showed 25-50 represents ‘slightly effective’; 50-70 represents ‘effective’; and more than 75 represents ’Very effective’. Minus number represents the negative effect. 3Bold letters showed effectiveness as a ‘slightly effective’, ‘effective’, or ’Very effective’.
Oligosaccharides are known to stimulate Bifidobacterium in the colon [16-18]. We wondered whether the combined intake of Kefir with oligosaccharides might support the effect of Kefir for BM. To address this, the intake of oligosaccharides was also added only in the Kefir-taking group during the last 40 days of Examination Period A. However, we could not see a clear difference in the first three months of the examination (Figure 1 and Examination Period A).
After 3 months of the initial Examination Period A finished, Examination Period B began and lasted for another 3 months. In Examination Period B, the participants in Group B started the intake of Kefir, and the participants in Group A started to take powdered milk formula. The participant B-4 immediately showed BM without administration of GE (Figure 1 and Table 3). The effect of Kefir on constipation of the participant B-4 was 84% improved compared to pretreatment and 60% improved compared to the intake of powdery milk (placebo control) (Table 3). The participant B-5 showed the mild improvement of BM without administration of GE (Figure 1 and Table 3). Kefir could improve by 29% reduction in the administration of GE compared to pretreatment and 26% reduction to the powdered milk formula intake period. Therefore, we judged the intake of Kefir for the participant B-5 was ‘slightly effective’. For the last 40 days of Examination Period B, oligosaccharide was added to the intake of Group B. The participant B-3 showed the improvement of BM, which showed a synergistic effect (Table 3).
Therefore, we judged the intake of Kefir to the participant B-3 was effective only in the presence of the support of oligosaccharides. However, we could not see any effect of the addition of oligosaccharides to the initial kefir on participants B-1 and B-2 (Figure 1 and Table 3).
In this case, it is likely that the microbial flora in A-2’s intestine has been changed in a positive direction due to the intake of Kefir. Second in success was the participant A-1, who showed increased the improvement of BM as long as the oral intake of Kefir was maintained. The third most successful was the participant B-4, who showed Kefir could prevent constipation but also that the intake of powdery milk could improve constipation. These three cases in particular suggest that including the Kefir-fermented milk in daily meals is effective for these people to prevent constipation. The effect of Kefir for these individuals is in fact “therapeutic” rather than “prophylactic”. Since this study was carried out with highly limited sample size, it might be insufficient to do the statistical analysis. However, to understand whether the intake of Kefir is statistically effective or not, Fischer’s exact test was done using the results from this study. Clear improvement of BM was observed in four participants, A-1, A-2, B-4 and B-5, who showed improvement by the oral intake of only Kefir, while other seven participants, A-3, A-4, A-5, A-6, B-1 B-2 and B-3, did not show noticeable Kefir-stimulated BM effects compared to untreated control and placebo controls. The result of Fischer’s exact test revealed that the oral intake of Kefir could significantly improve BM without administration of GE compared to untreated control and placebo controls (p = 0.045). This statistical result suggests that the oral intake of Kefir significantly improves BM without the administration of GE among handicapped persons.
The result of the intake of Kefir with oligosaccharides was a little bit complicated. The intake of Kefir with oligosaccharides showed stimulation of BM without GE in the participant A-1, A-2, B-3 and B-4 compared to untreated. This comparison was statistically significant (p = 0.045). On the other hand, in comparison to placebo control, the intake of Kefir with oligosaccharides showed stimulation of BM without GE in the participant A-1, A-2, and B-3, but not in the participant B-4. Moreover, the participants A-4 and B-5 showed negative effects. Because of this, this comparison was not significant (p=0.50). Therefore, we cannot suggest that the additional intake of oligosaccharides on Kefir have a significant benefit for the prevention of constipation. One problem is that the number of subjects is too small in this attempt. Further investigation is required to conclude whether the prebiotic effect induced by oligosaccharides stimulates the prophylactic effect of Kefir-fermented milk on constipation.
Constipation is one of the most serious problems for the care of handicapped people. Unlike normal individuals, the major causes of constipation are related to their physical abnormality, such as mobility limitations, dysfunctions of the GI system, pharmacological factors, and nutritional factors [19]. Therefore, it is extremely difficult to prevent and treat constipation. To date, many efforts to prevent constipation have been made, but effective ways to treat and prevent constipation of handicapped people have barely been reported. Since the effort for preventing constipation continues for the entire lifetime of the handicapped person, we aimed to explore effective constipationpreventing methods among foods, and found one, Kefir-fermented milk. Among various probiotic species, we selected Kefir because Kefir is composed with a variety of microorganisms, such as Lactobasilli , Lactococci , Enterococci , yeasts and etc. We expected that this nature of Kefir might increase the chance to release constipation, and 4 from 11 participants indeed showed the improvement of BM. This result suggests that Kefir possesses the prophylactic effect on constipation. For future, understanding how Kefir stimulates BM will become important topic in this field. One possibility of probiotic effect of Kefir is that probiotic species included in Kefir directly changes intestinal conditions, such as intestinal flora, pH, concentration of organic acids, and other components, and this results in the stimulation of Gastro- Intestinal (GI) function. In the next stage, we would like to determine which species in Kefir is responsible for the prophylactic effect on constipation. Another possibility, this can be a Kefir-specific mechanism, is that Kefirans may stimulate BM. Kefirans are polysaccharides produced by Lactobacillus kefiranofaciens , and it was shown that the oral feeding of Kefirans to constipated rats improved the BM function and released constipation [13]. So far, whether Kefirans improved the BM in human has not been reported, but our result is not in conflict with their study. Anyhow, we will continue to investigate the mechanism of probiotic effect of Kefir on constipation.
Although we need to point out the shortcomings of the study including the inadequate experimental units and the limited response among the subjects, we could at least observe that the oral intake of Kefir has benefits on the reduction of GE even though not all people are improved, and therefore that acting on our findings can help decrease medical costs, an contribute to easing the physical labor and to increasing the work efficiency of nurses spending much time and effort for the administration of GE, and also contribute to an increase in the quality of life for handicapped people.
We thank Ms Yuka Kobayashi and Satomi Onoda for the technical support for this study. We also thank Dr. Seiichi Chiba for giving us some advices about writing this manuscript.