Andrology-Open Access
Open Access
ISSN: 2167-0250
ISSN: 2167-0250
Research Article - (2014) Volume 3, Issue 2
Introduction: In Ethiopia, an estimated 676 maternal deaths occur for every 100,000 live births. The major causes of mortality and morbidity are direct obstetric causes; they mainly occur from the third trimester of pregnancy to the first week following delivery. This study elucidates the type, magnitude and associated factors of postpartum morbidity conditions among pregnant women who gave birth at the health institutions and is essential to understand the health care need for obstetric emergencies, postpartum conditions and to prepare health organizations to better monitoring and evaluation of safe motherhood programs.
Objective: To assess birth outcome and prevalence of postpartum morbidity among women attending antenatal care and gave birth at health institutions in Gondar town.
Methods: We have conducted a four-month follow up study among 203 randomly selected pregnant women from five health institutions in Gondar town. Data were collected between March 1, 2010 and June 30, 2010 through interviews and physical examinations at four follow up visits: antenatal care, labor and delivery, 12th and 42nd postpartum days. We have used Epi Info 2002 for data entry and Statistical Package for the Social Sciences (SPSS) for data analysis.
Results: A total of 203 (89.04%) pregnant women completed the four follow up visits and were included in the analysis. Postpartum morbidity conditions were found among 48 (23.6%) mothers, of whom 12 (5.9%) mothers had suffered two or more morbidity conditions. Overall, morbidity from postpartum hemorrhage had the highest prevalence 30 (14.8%) followed by sepsis and anemia. Intra-partum deviations were the main contributing factor to the postpartum morbidity conditions (AOR=4.148, P=0.027). There were 5(2.5%) still births and 38(18.7%) low birth weights.
Conclusion and recommendation: The occurrence of postpartum morbidity, low birth and still birth among pregnant women attending and giving birth at health institution in Gondar town was significant health concern. Intrapartum abonormalities were the main predictive factor triggering maternal morbidity conditions. The time from birth to the first 6 hrs of purperum was the peak time to postpartom hemorrhage. Therefore, interventions such as universal use of the partograpgh, active third stage management and encouraging all delivering women to stay in the health institution during the first 24 hours of delivery could play a key role in reducing postpartum morbidity
<APH: Ante Partum Hemorrhage; AIDS: Acquired Immuno Deficiency Syndrome; ANC: Antenatal Care; C/S: Caesarean Section; EPHA: Ethiopian Public Health Association; FGAE: Family Guidance Association of Ethiopia; HIV: Human Immuno Deficiency Virus; LB: Live Birth; LBW: Low Birth Weight LNMP: Last Normal Menstrual Period; MDG: Millennium Development Goal; MOH: Ministry of Health; PID: Pelvic Inflammatory Disease; PIH: Pregnancy Induced Hypertension; PNC: Post Natal Care; PPH: Postpartum Hemorrhage; RTI: Reproductive Tract Infection; SVD: Spontaneous Vaginal Delivery; UOG: University of Gondar; WHO: World Health Organization
The risk of maternal mortality in developing countries is of grave significance and accompanied by a high incidence of morbidity among women who survive childbearing. In 2008 an estimated 358,000 maternal deaths occurred worldwide [1], 99% of which were in developing countries and half of which occurred in Sub-Saharan Africa (SSA) [1,2]. For every maternal death in SSA another 16 to 100 women will be disabled or permanently impaired [3]. Over 54 million women in developing countries are estimated to suffer acute complications yearly, with over 20 million considered so serious as to warrant referral care. Around 30 million women suffer from short or long-term illness related to childbirth that adversely affects the quality of their lives and those of their families. Additionally, some women who survive delivery become chronically ill and eventually die from chronic or infectious diseases [4,5].
The majority of maternal morbidity and death occurs from the third trimester of pregnancy to the first week following delivery [1]. The postpartum period is defined as a period from approximately one hour after the delivery of the placenta through to the following six weeks. Traditionally the postpartum period is considered as the mother’s time of rest and rapid return to normal function; however, more than 60% of maternal deaths occur in this period [6]. Hemorrhage, pregnancy induced hypertensive disorders, obstructed labor, obstetric infections and thromboembolism are the most common causes of postpartum deaths and morbidities. It is also noteworthy to consider urinary complications and mental disorders as significant contributors to maternal morbidity [6].
There had been various factors associated with maternal morbidity and mortality. The most commonly indicated associated factors in varying studies were poverty, low education, adolescent pregnancy, grand multi-parity, absence of family planning, poor access to health services and underlying infection like HIV. The named associated factors are all considered problematic on an epidemic level in Sub- Saharan Africa [7-10].
International efforts had been made to reduce maternal and neonatal mortality and morbidity through provision of antenatal care, skilled delivery attendance at birth and postpartum services since the launch of the Safe Motherhood Initiative in 1987 [11]. Interventions such as; provision of family planning services, education and empowerment for women, early referral during pregnancy, labor and delivery, and postpartum services designed for low resource settings are all significant in reducing the maternal and neonatal morbidity and mortality rates [12-14].
In Ethiopia the levels of maternal and infant mortality and morbidity are among the highest in the world. According to Ethiopian Demographic Health Survey 2010, an estimated 676 maternal deaths occur for every 100,000 live births. The major causes of mortality and morbidity are obstetric hemorrhage, pregnancy induced hypertension, sepsis, obstructed labor and predominantly unsafe induced abortion.
Moreover, although access to primary health care services, as expressed in the potential health services coverage reaches 92% [15], maternal health care service utilization is still considerably low. For example, only 34% of mothers reported receiving antenatal care from health professionals. In urban areas, health professionals provide antenatal care for seventy six percent of mothers, in comparison to rural areas, which only provides antenatal care for approximately twenty six percent of mothers.
Despite the fact that only 10% of deliveries were attended at the health facilities, the proportion of deliveries in urban and rural Ethiopia is grossly varied. For instance, 50 percent of births to urban mothers were delivered in a health facility, compared with 4 percent of births to rural women. Postnatal Care Provision (PNC) is considerably poor, with only 11 percent of mothers reporting postnatal care within the critical first two days after delivery [15].
Safe motherhood programs have increased their emphasis on the importance of postnatal care due to a large proportion of maternal and neonatal deaths occurring within the first few days after delivery [13-18]. Addressing postnatal conditions is one of the most prominent strategies to reduce the MMR especially for countries like Ethiopia, who has one of the highest contributing figures of maternal mortality. Therefore, assessing the magnitude and associated factors for postpartum morbidity is useful to understand the health care need for obstetric emergencies, postpartum conditions and to prepare health organizations to better monitoring and evaluation of safe motherhood programs.
General objective
Prospectively assess birth outcome and prevalence of postpartum morbidity conditions among women attending antenatal care service and give birth at health institutions in Gondar town, North West Ethiopia.
Specific objectives
To determine prevalence of postpartum morbidity among women attending antenatal care & give birth at health institutions in Gondar town.
To describe the birth outcomes of women who receive antenatal care.
To elucidate factors associated with postpartum morbidity conditions.
Methods
Study settings
Institutional based prospective study was implemented from March 1, 2010 to June 30, 2010 in Gondar town, which is located 741 km north west of Addis Ababa. In the North Gondar zone there are 3 hospitals, 33 urban and 69 rural health centers, 449 health posts, and 6 private clinics and one private hospital [16,17]. According to the 2007 census, the total population of Gondar town reached 206,987, of which 108,902 are female. The health institutions targeted by this study were: Gondar Health Center, Maraki Health Center, Azezo Health Center, Gondar branch Family Guidance Association, and the University of Gondar Hospital. The University of Gondar Hospital is the only referral hospital in the zone, serving for over 6 million people. This hospital facilitates approximately 6000 surgeries and 2000 deliveries every year. Although the five health institutions mentioned above provided maternal health care services, most women in Gondar town preferred to give birth at the University Hospital. Despite the fact that the ANC coverage at the health centers was high, the reported monthly delivery service in each health centers was not more than 10-20 deliveries per month.
Study population
The participants of the study were pregnant mothers who had ANC follow up and gave birth at health institutions in Gondar town. All women who were lived in Gondar town; had ANC follow up in the government and non-government health institutions were included in the study. However, women who failed to complete the maternal postpartum interviews, gave birth at home and lost form follow up examinations were excluded from the study.
Sample size and sampling procedure
The sample size was determined by using a single population proportion formula  considering the following assumptions: magnitude of postpartum morbidity 50%, (p=0.5); 5% level of significance (α=0.05); 5% marginal error (d=0.5), 95% confidence interval (1.96), N=408 which was the total number of pregnant women population who were living in Gondar town, whose gestational age greater or equal to 37 completed weeks and services at the targeted health institutions by this study: Gondar hospital, Gondar, Azezo and Maraki Health Centers and the Gondar branch Family Guidance Association clinic. Among those who attended the ANC follow up only 408 were fulfilled the eligibility criteria (term pregnancy; estimated from the first date of last menstrual period, resided in Gondar town and planned to give birth in the health institutions) and of which 228 women were selected through systematic random sampling technique, (Figure 1) attending ANC during the study period. The final sample size was adjusted by 15% non-response rate/loss to follow up and became 228. The antenatal registration books were used as a sampling frame and a total of 228 women were selected using a systematic random sampling technique. During the study period there were a total of 2173 women attending ANC
considering the following assumptions: magnitude of postpartum morbidity 50%, (p=0.5); 5% level of significance (α=0.05); 5% marginal error (d=0.5), 95% confidence interval (1.96), N=408 which was the total number of pregnant women population who were living in Gondar town, whose gestational age greater or equal to 37 completed weeks and services at the targeted health institutions by this study: Gondar hospital, Gondar, Azezo and Maraki Health Centers and the Gondar branch Family Guidance Association clinic. Among those who attended the ANC follow up only 408 were fulfilled the eligibility criteria (term pregnancy; estimated from the first date of last menstrual period, resided in Gondar town and planned to give birth in the health institutions) and of which 228 women were selected through systematic random sampling technique, (Figure 1) attending ANC during the study period. The final sample size was adjusted by 15% non-response rate/loss to follow up and became 228. The antenatal registration books were used as a sampling frame and a total of 228 women were selected using a systematic random sampling technique. During the study period there were a total of 2173 women attending ANC
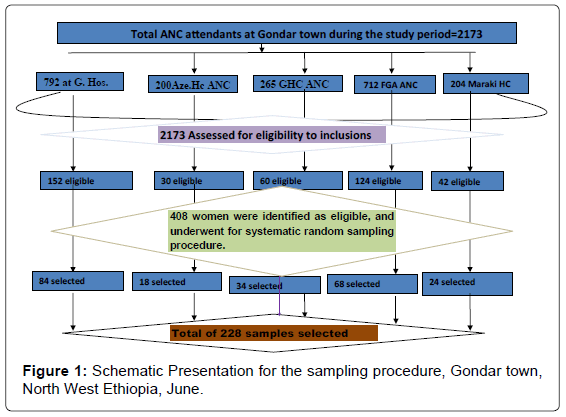
Figure 1: Schematic Presentation for the sampling procedure, Gondar town, North West Ethiopia, June.
Study variables
Dependent variables: Postpartum morbidity: (Postpartum hemorrhage, pregnancy induced hypertension and puerperal sepsis). Birth outcome: (birth weight, live vs. still birth)
Independent variables: Maternal age, level of education, household income status, parity, mode of delivery (SVD, C/S, Instrumental), labor abnormality (long duration on the rupture of membranes, retained placenta, long duration of labor), presence of episiotomy or perennialtear, maternal HIV infection status, and past obstetrical complications
Data collections
Data were collected through face to face interview and physical examination using interview guides and examination checklists, which were prepared both in English and Amharic languages. Twenty two midwives were collecting the data after they had been given two days training. The study tools were validated by pretesting on 11 ANC attendant mothers. The data collectors were using the Amharic version questioners for interview, and undertook observation/examinations based on the observation checklists. All enrolled study participants had been interviewed and examined at four time points. For easy communication identification card was given to each of the study participants; on the card only participant’s code and appointment dates were indicated.
The first interviews and examinations were made at antenatal care delivery points, during that time socio-demographic and other background information were collected. Then after for the subsequent follow up visits, all enrolled study participants were instructed to visit the health institutions at their specific appointment dates or for any reason if they feel sick.
The second follow up visits were at the period of labor and delivery. At that visit, birth outcomes and birth-related complications were assessed. Up on the third and fourth follow up appointment periods on the 12th and 42nd days of postpartum, early and late postpartum morbidities were investigated.
The serious of examinations undertaken during all follow up periods were: measurements of vital signs, a visual assessment of conjunctiva and hemoglobin determination to detect severe anemia, assessment of protein urea, examination of breast, palpation of the abdomen, a visual check of the perineum for (tears, vaginal discharge, uterine inversion or prolapsed) as required.
Quality assurance
The data collectors were given two days training on the methods of data collection, supervised and assisted by duty intern physicians and principal investigator during data collection. The data collectors used pretested Amharic version interview guide and examination checklists to abstract information from participants.
Outcome measurements
The primary outcome measurements for postpartum morbidity were: Postpartum hemorrhage, Pregnancy induced hypertension, and puerperal sepsis. The following operational definitions were used to synthesize maternal reports of signs and symptoms into specific complications and morbidities.
? Postpartum hemorrhage: Estimated loss of >500 ml of fresh or clotted blood immediately after birth in SVD or >1000 ml in C/S birth. Furthermore maternal self-report of much bleeding that cause loss of consciousness or seek medical attention after 24 hrs to 6 weeks of delivery discharged from the health institutions also considered as PPH.
? Hypertensive disorder of pregnancy (pre-eclampsia). Diastolic pressure >90 plus protein uria, headache or dizziness, where symptoms began only during the last trimester of pregnancy
? Retained placenta: estimated placenta delivery of >30 min after birth or history of manual or metallic uterine evacuation.
? Abnormal labor: Any course of labor fulfilling one or more of the following criteria: labor is augmented or terminated by C/S for dystocia, fetal presentation not by vertex, birth not through the natural effort of the mother and assisted by Instrument, labor not accomplished with reasonable time span for delivery of placenta >15 minutes, rupture of membrane 1 hour before onset of labour, membrane rupture >12 hrs before delivery of fetus, and total course of labor >24 hrs.
? Non-specific postpartum illness: Illness did not meet Operational Definition of specific conditions, but had selfreported poor health on the days of postpartum period.
Data analysis
The operational definitions were used to synthesize maternal reports of signs and symptoms into specific complications and morbidities. Data entry was done by using EPI Info 2002 and exported to SPSS version 15.0 software package for analysis. The data was analyzed using logistic regression to determine the effect of various factors on the outcome variable and to control confounding effects. The results were presented in the form of tables, figures and texts using frequencies and summary statistics such as mean, standard deviation, and percentage to describe the study population in relation to relevant variables (Maternal age, level of education, household income status, parity, mode of delivery (SVD, C/S, Instrumental), labor abnormality (long duration on the rupture of membranes, retained placenta, long duration of labor), presence of episiotomy or perennial-tear, maternal HIV infection status, and past obstetrical complications). The strength of association between independent and dependent variables was assessed using the odds ratio with 95% confidence interval.
Ethical consideration
Ethical clearance was obtained from the ethical review board of University of Gondar. On top of that following discussion of the study objectives, all study participants were asked to give their verbal informed consent. Confidentiality of participants’ response and clinical findings were assured by protecting participants’ name; study participants were only identified by their code numbers. Moreover, all participants and their babies were treated for any morbidity conditions identified during the study period.
Socio demographic characteristics
Out of 228 pregnant women who participated in the study, 203 (89.04%) completed the four follow up visits and were included in the analysis. The remaining 25 (10.96%) women withdrew from the follow up appointments and excluded from the analysis. The mean age of study participants was 25.3 years with standard devotions of +4.72 SD. In fact most respondents 79 (38.9%) were found in the age group of 20- 24 years. One hundred thirteen women were house wives, and nearly half of women completed secondary and above level of education. Over ninety seven percent of the study subjects were Amhara in ethnicity and most were Orthodox Christian by their religion (Table 1).
| Variable | N=203 | Percentage |
|---|---|---|
| Age of mother | ||
| <20years | 13 | 6.40 |
| 20-24 years | 79 | 38.91 |
| 25-29 years | 67 | 33.00 |
| 30-34 years | 31 | 15.27 |
| 35-39 years | 13 | 6.40 |
| Level of education | ||
| no education | 39 | 19.21 |
| Primary education | 29 | 14.28 |
| Secondary cycle | 99 | 48.77 |
| Higher education | 36 | 17.73 |
| House hold income | ||
| 100-600 Eth. Birr | 76 | 37.44 |
| 601-1500 Eth. Birr | 74 | 36.45 |
| 1501-5000 Eth. Birr | 53 | 26.11 |
| Marital Status | ||
| Married | 188 | 92.61 |
| Divorced | 4 | 1.97 |
| Unmarried | 11 | 5.42 |
| Religion | ||
| Orthodox | 159 | 78.33 |
| Muslim | 41 | 20.19 |
| Other | 3 | 1.48 |
| Ethnic group | ||
| Amhara | 198 | 97.54 |
| Tigray | 5 | 2.46 |
| Occupation | ||
| civil servant | 37 | 18.23 |
| House wife | 113 | 55.66 |
| Maid servant | 6 | 2.95 |
| Student | 17 | 8.37 |
| Trader | 20 | 9.85 |
| Wage worker | 10 | 4.93 |
Table 1: Distribution of women by their socio demographic characteristics (N=203) Gondar town, North West Ethiopia, June 2010.
Past obstetric history
Majority 123 (60.6%) of study participants were multi parous, of whom 6 (4.9%) had previous caesarean delivery and 43 (35%) were having past obstetrical complications like: obstetric hemorrhage, pregnancy induced hypertension and still birth (Table 2).
| Variable | N=203 | Percentage |
|---|---|---|
| Parity | ||
| I | 80 | 39.41 |
| II-IV | 120 | 59.11 |
| ≥V | 3 | 1.48 |
| prolonged labor | 22 | 10.83 |
| obstructed labor | 7 | 3.45 |
| Abortion | 25 | 12.32 |
| Still birth | 11 | 5.42 |
| Obstetric Interventions | ||
| Caesarean Section | 6 | 2.95 |
| Instrumental delivery | 23 | 11.33 |
Table 2: Distribution of women by their past obstetric history (N=123) Gondar town, North West Ethiopia, June 2010.
Current obstetric conditions
In the current pregnancy, 85 (41.9%) of women were received iron and folic acid supplementation, and 182 (89.7%) women were tested negative for HIV infection. Among all women participated in this study, there were 51 (25%) unplanned and 24 (11.8%) unwanted pregnancies respectively. The large majority 175 (86.21%) of study participants gave birth at the University of Gondar Hospital. By the time of delivery, the mean age of gestation was 39.9 weeks with standard deviation of +1.5. Among the total study participants, twenty five gave birth through caesarean section, and thirty two women were facing abnormal labour conditions: 6 (3.0%) had prolonged labor, 11(5.4%) had premature rupture of membranes and 5 (2.5%) had manual removal of placenta (Table 3).
| Variable | N=203 | Percentage |
|---|---|---|
| Current obstetrical information | ||
| Place of Delivery | ||
| Hospital | 175 | 86.21 |
| Health Center | 28 | 13.79 |
| HIV status | ||
| Unknown | 4 | 1.97 |
| Positive | 17 | 8.37 |
| Negative | 182 | 89.65 |
| Desire of mother for recentpregnancy | ||
| Planed and wanted | 128 | 63.05 |
| Unplanned | 51 | 25.12 |
| Unwanted | 24 | 11.82 |
| Labor and delivery condition | ||
| Spontaneous vaginal delivery | 176 | 86.69 |
| Instrumental delivery | 2 | 0.99 |
| Caesarean section | 25 | 12.32 |
| Prolonged labor | 6 | 2.96 |
| Prolonger rupture of membranes | 11 | 5.42 |
| Retained placenta | 5 | 2.46 |
| Augmentation | 8 | 3.94 |
Table 3: Distribution of women by their current obstetric conditions (N=203) Gondar town, North West Ethiopia, June 2010.
Among women who had vaginal birth, there were 25 (12.3%) episiotomies and 20 (9.9%) perennial tears. The rate of episiotomy 22 (88%) and perennial tear 11 (55%) were high among nulli-para mothers, and the caesarean section rates were high among multipara mothers 16 (64%). See Figure 2 and Table 4 for detailed description of birth related complications and obstetric interventions by parity groups.
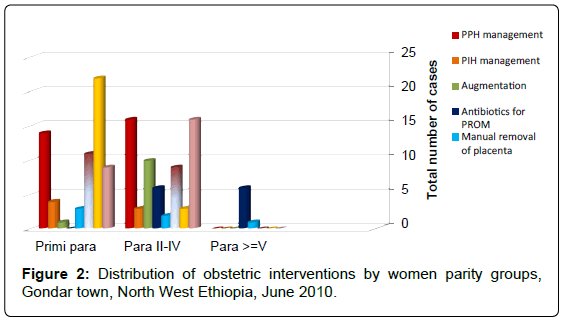
Figure 2: Distribution of obstetric interventions by women parity groups, Gondar town, North West Ethiopia, June 2010.
| Type ofcomplication&obstetric interventions | Percent within parity groups with the condition | Total % of all Parity | ||
|---|---|---|---|---|
| Para I(N=80) | Para II-IV(N=120) | Para>=V(N=3) | ||
| PPH | 14(17.50 | 16(13.33) | 30(14.78) | |
| Pre-eclampsia | 4(5.00) | 3(2.50) | 7(3.45) | |
| Total course of labor | ||||
| <16 hours | 50(62.50) | 91(75.83) | 3(100.00) | 144(70.94) |
| 16-<24 hours | 30(37.50) | 23(19.17) | 53(26.11) | |
| >=24 hours | 6(5.00) | 6(2.96) | ||
| Duration of membranes rupture | ||||
| <6hours | 68(85.00) | 95(79.17) | 3(100.00) | 166(81.77) |
| 6-<12 hours | 11(13.75) | 15(12.50) | 21(12.34) | |
| >=12 hours | 1(1.25) | 10(8.33) | 11(5.45) | |
| Duration of placental delivery | ||||
| <15 minutes | 77(96.25) | 118(98.33) | 2(66.70) | 197(97.04) |
| 15-<30Minutes | 3(3.75) | 1(0.83) | 1(33.30) | 5(2.46) |
| >=30minutes | 1(0.83) | 1(0.49) | ||
| Episiotomy | 22(27.50) | 3(2.50) | 25(12.32) | |
| Perennial tear | 11(13.75) | 9(7.50) | 20(9.85) | |
| Caesarean section | 9(11.25) | 16(13.33) | 25(12.32) | |
Table 4: Distribution of labor and delivery related complications and obstetric interventions by women parity groups. Gondar town, North West Ethiopia, June 2010.
Postpartum morbidity
During the four months data collection period, postpartum morbidity meeting at list one major direct obstetrical cause case definition was found among 48 (23.6%) mothers, of whom 12 (5.9%) were having two or more morbidity conditions. Over all morbidity from postpartum hemorrhage had the highest prevalence 30 (14.8%) followed by sepsis 14 (6.9%) and anemia 13 (6.4%). The main documented causes of maternal sepsis among study participants were: pelvic infection 6 (42.8%), mastitis 2 (14.4%) and wound infections 6 (42.8%), (Table 5). Most of the postpartum morbidities were occurred, after 6 hours of delivery to the first week of puerperium. However, magnitudes of morbidity like hemorrhage 24 (80%) and anemia 10 (76.9%) were peak at delivery and low at 12th postpartum day on wards (Figure 3).
| Type of morbidity | During Pregnancy, N=34 | During Delivery, N=46 | From Discharge to 12 day of postpartum, N=58 | At 42 day of postpartum, N=8 | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| Hemorrhage | 24 | 52.17 | 6 | 10.34 | 2 | 25.00 | ||
| Pre-eclampsia | 8 | 23.53 | 7 | 15.23 | ||||
| Anemia | 9 | 26.47 | 10 | 21.74 | 5 | 8.62 | 1 | 12.50 |
| Breast | ||||||||
| -Engorgement | 4 | 6.91 | ||||||
| -Mastitis | 2 | 3.45 | ||||||
| Genitourinary tract | ||||||||
| -UTI | 6 | 17.65 | 1 | 2.17 | 3 | 5.17 | 1 | 12.50 |
| -Abnormal Vaginal discharge | 4 | 11.76 | 2 | 4.35 | 10 | 17.24 | 1 | 12.50 |
| -Pelvic infection | 6 | 10.35 | ||||||
| Wound infection | ||||||||
| -C/S | 1 | 1.72 | ||||||
| -Perineal tear | 3 | 5.17 | ||||||
| -Episiotomy | 2 | 3.45 | ||||||
| Non-specific and otherillness | 7 | 20.56 | 2 | 4.35 | 16 | 27.58 | 3 | 37.50 |
Table 5: Distribution of maternal morbidity from third trimester pregnancy to the end of postpartum period (N=203), Gondar town, North West Ethiopia, June 2010.
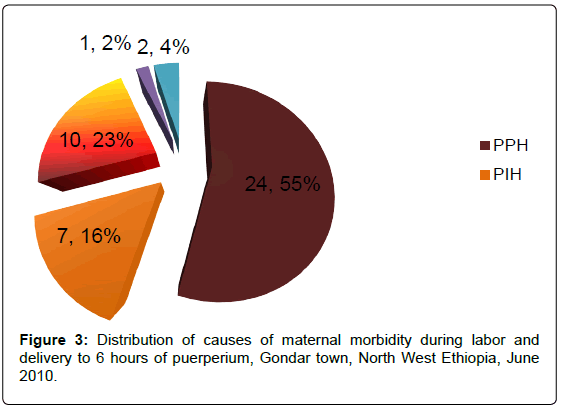
Figure 3: Distribution of causes of maternal morbidity during labor and delivery to 6 hours of puerperium, Gondar town, North West Ethiopia, June 2010.
Among women who had hemorrhage during delivery, six were resuscitated with IV fluid for severe bleeding. At the third trimester of pregnancy, there were 7 (3.4%) preeclampsia cases but no women were developed pregnancy induced hypertension during delivery and postnatal period.
Large proportions of postpartum morbidities were reported during the first week of puerperium. At which time 54 women had developed some sort of morbidity conditions (Table 5). Of which 6 (2.9%) had postpartum hemorrhage, 14 (6.9%) had sepsis, 5 (2.5%) had anemia, 3 (1.5%) had urinary tract infection, 10 (4.9%) had abnormal vaginal discharge, and 16 (7.9%) mothers had developed morbidity condition which were not satisfying the specific case definitions of major direct obstetrical cause morbidities (Figure 4).
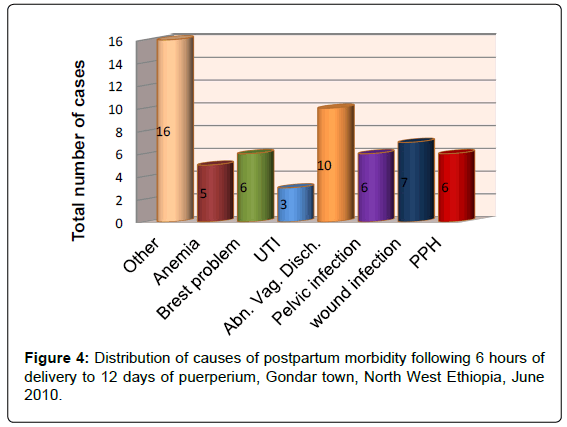
Figure 4: Distribution of causes of postpartum morbidity following 6 hours of delivery to 12 days of puerperium, Gondar town, North West Ethiopia, June 2010.
During the 42nd days of purperum, most women were recovered from their morbidity conditions and transferred to their non-gravid state; however some women were not recovered yet. At which time there were 8 women suffered from: vaginal bleeding 2 (1%), anemia 1 (0.5%), UTI 1 (0.5%), abnormal vaginal discharge 1 (0.5%), and other non-specific symptoms 3 (1.5%) (Table 5).
Birth outcome
Among the total infants born during the study period 111 (54.7%) were male and 92 (45.3%) were female. The mean birth weight was 2.95 Kg with the standard deviation of ± 0.48 SD. Eighteen point seven percent of infants were born with low birth weight (<2.5 kg.), and there were 5 (2.5%) still births (Table 6).
| Birth outcome | Percent within parity groups with the outcome | Total % of all Parity, N=203 | ||
|---|---|---|---|---|
| Para I, N=81 | Para II-IV, N=120 | Para>=V, N=3 | ||
| Sex | ||||
| Male | 36(44.44) | 72(60.00) | 3(100) | 111(54.68) |
| Female | 44(54.32) | 48(40.00) | 92(45.32) | |
| Weight | ||||
| 2.5 -4 Kg | 58(71.60) | 104(86.67) | 3(100) | 165(81.28) |
| <2.5 Kg | 22(27.16) | 16(13.33) | 38(18.72) | |
| Live status at birth | ||||
| Live birth | 79(97.53) | 116(96.67) | 3(100) | 198(97.54) |
| Still Birth | 1(1.23) | 4(3.33) | 5(2.46) | |
Table 6: Distribution of birth outcome by maternal parity groups, Gondar town, North West Ethiopia, June 2010.
Factors associated for postpartum morbidities
The bivariate model have showed an increased risk of postpartum morbidity among uneducated women (COR=2.4), women whose age less than 20 years (COR=1.6) and greater than 35 years (COR=4.8), unmarried women (COR=1.2), and women whose monthly household income below 600 Eth. birr/month (COR=1.6).
Similarly, an increased postpartum morbidity was identified among women whose parity greater or equal to five (COR=1.5), women who had past obstetric complication (COR = 1.5), and women who had labor abnormality for the recent delivery (COR=6.043).
Over all after the effects of all potential confounding factors held constant by multiple logistic regression, postpartum morbidities were significantly associated with labor abnormality (AOR=4.148, 95%CI :1.180, 14.578) (Table 4). The multivariate model has also showed statistically significant association between PPH and obstetric risk factors. Women who had labor abnormality during recent delivery were about 4 times (AOR=4.071, 95%CI: 1.161, 14.272) more likely to develop PPH than women whose labor was normal. Moreover, the likely hood of PPH was about three and twelve times higher among women who had episiotomy or perennial tear (AOR=3.289, 95% CI: 1.329, 8.149), and preeclampsia (AOR=12.794, 95% CI: 2.537, 64.525) respectively (Table 7).
| Variables | Bivariate Analysis | Multivariate analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|
| % having postpartum morbidity | P-value | Crude OR | 95% CI | P-value | Adjusted OR | 95% CI | |||
| Lower | Upper | Lower | Upper | ||||||
| HIV status | |||||||||
| Positive | 12.50 | 0.287 | 0.438 | 0.096 | 2.002 | 0.291 | 0.409 | 0.078 | 2.149 |
| Negative | 24.62 | 1 | 1 | ||||||
| Preeclampsia during pregnancy& delivery | 25.00 | 0.927 | 1.080 | 0.211 | 5.533 | 0.706 | 1.414 | 0.234 | 8.535 |
| No | 23.61 | 0.534 | 1 | 1 | |||||
| Anemia during delivery | 50.00 | 0.637 | 1.956 | 0.0120 | 31.754 | 0.189 | 0.125 | 0.006 | 2.784 |
| No | 23.45 | 1 | 1 | ||||||
| Iron supplementation during pregnancy | 22.45 | 0.713 | .883 | 0.456 | 1.710 | 0.775 | 0.899 | 0.432 | 1.870 |
| No | 24.62 | 1 | |||||||
| Mode of delivery | |||||||||
| Caesarean section | 56.00 | 0.000 | 5.390 | 2.250 | 12.913 | 0.418 | 1.732 | 0.458 | 6.546 |
| Spontaneous Vaginal delivery | 19.10 | 1 | 1 | ||||||
| Labor abnormality | 56.32 | 0.000 | 6.043 | 2.710 | 13.475 | 0.027 | 4.148 | 1.180 | 14.578 |
| No | 17.50 | 1 | 1 | ||||||
| Episiotomy or perennial tear | 22.24 | 0.799 | 0.902 | 0.409 | 1.992 | 0.904 | 0.940 | 0.342 | 2.583 |
| No | 24.11 | 1 | 1 | ||||||
| Postpartum hemorrhage within 6 hour of birth | 31.46 | 0.236 | 1.623 | 0.728 | 3.617 | 0.940 | 0.958 | 0.316 | 2.908 |
| No | 22.00 | 1 | 1 | ||||||
Table 7: Bivariate and multivariate analysis of recent and past obstetrical factors for post partum morbidities, Gondar town, North West Ethiopia, June 2010.
Postpartum hemorrhage was the leading cause of morbidity and it was higher among women who had labor abnormality (COR=4.403), caesarean section (COR=4.809), episiotomy or perennial tear (COR=2.385), not received iron and folic acid supplementation during pregnancy (COR=1.159), and women who had preeclampsia (COR=3.930) (Table 8).
| Variables | Bivariate Analysis | Multivariate analysis | |||||||
|---|---|---|---|---|---|---|---|---|---|
| % having postpartum hemorrhage | P-value | Crude OR | 95% CI | P-value | Adjusted OR | 95% CI | |||
| LowerUpper | LowerUpper | ||||||||
| Episiotomy or perennial tear | |||||||||
| yes | 28.90 | 0.290 | 1.98 | 1.091 | 5.210 | 0.010 | 3.289 | 1.329 | 8.141 |
| No | 14.63 | 1 | 1 | ||||||
| Caesarean section | |||||||||
| Yes | 44.00 | 0.001 | 4.809 | 1.963 | 11.777 | 0.260 | 2.202 | 0.557 | 8.699 |
| No | 14.00 | 1 | 1 | ||||||
| Preeclampsia during pregnancy | |||||||||
| Yes | 62.51 | 0.004 | 3.93 | 2.401 | 7.355 | 0.002 | 12.794 | 2.537 | 64.525 |
| No | 15.93 | 1 | 1 | ||||||
| Abnormal labor | |||||||||
| Yes | 40.61 | 0.000 | 4.403 | 1.918 | 10.108 | 0.028 | 4.071 | 1.161 | 14.272 |
| No | 13.50 | 1 | 1 | ||||||
| Iron supplementation during pregnancy | 16.25 | 0.623 | 1.159 | 0.566 | 4.820 | 0.775 | .899 | 0.832 | 32.070 |
| No | 18.43 | 1 | |||||||
Table 8: Bivariate and multivariate analysis for associated risk factors for postpartum hemorrhage during labor and delivery, Gondar town, North West Ethiopia, June 2010.
This institution based prospective study tried to measure the incidence and prevalence of postpartum morbidity among women who were using maternal health care service at Government and Non- Government health institutions in Gondar town. The study findings have indicated significant health concerns to pregnant women. Postpartum hemorrhage was the leading cause of morbidity, followed by sepsis, anemia and preeclampsia respectively. These findings were in line with many other studies conducted in west & East African countries [6-9].
The time from delivery to one week of postpartum was critical period that large proportions of postpartum morbidity conditions were reported. The peak incidences of PPH and anemia were recorded during delivery time and over the subsequent postpartum periods their magnitude sharply declined. These findings were agreed with the statements made by WHO and Zambia’s study [1,6]. In this study all pre-eclamptic women were completely recovered from their illnesses within one week of delivery, and no single woman has died or developed near-miss complication. This would remark the medical care provided to all pregnancy induced hypertension cases was successful and would strengthen the fact that severe morbidity and mortality from most direct obstetric causes is preventable.
In our study, the overall prevalence of postpartum morbidity was much lower as compared to a community based prospective study conducted in Dhaka. In the Daka’s study there were 36% serious delivery related complications, 75% reported postpartum morbidity, and two maternal deaths [7]. On the other hand the findings of our study were the highest when compared to a study conducted in Benin, Cote d’lvoire and morocco Hospitals [18]. The reasons for these discrepancies might be the variation in case classifications, study settings, and study designs.
The major direct obstetric causes remain similar to this study and most other studies conducted both in developed and developing countries. In some low-resource regions, obstructed labor and sepsis remain significant causes of severe maternal morbidity [6-9,19,20]. Two studies from Ethiopia have also showed obstructed labor was a cause of 9.1% maternal death in Jimma Hospital, [21,22] and 3.3% hospital admissions in Adigrat town [23]. In contrast in our study obstructed labor, uterine prolapse and other direct obstetric morbidity cases were not identified. The possible explanation might be our study investigated only the urban segment of the society and did not evaluate pregnant women who have poor access and utilization behavior to the maternal health care service.
In this study the magnitudes of specific morbidity causes like PPH, PIH, and sepsis were higher when compared with a study conducted in six West African countries [24]. On the other hand this study finding was consistent with a hospital based study conducted in Uganda [9]. The reasons for the similarity might be, Ethiopia and Uganda are found in the Sub-Saharan Africa regions with similar population, living standard, and the studies were conducted in similar study settings.
The results of this study showed that, the likelihood of postpartum morbidity was high among women age <20 and >35 years, low household monthly income, unmarried, primipara for preeclampsia, low level of education, and past obstetric complication. Almost all of these predisposing factors described and agreed with the findings of many other studies [21-23]. Therefore this similarities lead to theoretical generation about the predisposing factors for postpartum morbidity.
The results of this study showed that, postpartum morbidity was significantly associated & influenced by labor abnormality. Moreover, women who did have labour abnormality, episiotomy or perennial tear, and preeclampsia would have significantly increased risk of postpartum hemorrhage. The association between PPH and preeclampsia lack precision (AOR=12.794, 95% CI: 2.537, 64.525), this could be due to small number of preeclampsia cases.
Measuring morbidity was not an easy task and we feel our study might over or underestimate postpartum morbidity conditions because of the following reasons: as the study did not include women who have poor access to the maternal health care service, limited in evaluating morbidities from the urban segment of the society where access to health care service was not a problem. Therefore, we were not able to measure the burden of morbidities like obstructed labor, fistula and many more other morbidity conditions. Furthermore, in this study we could not able to include home deliveries and we believe most of women who came to hospital might have an increased health problem. In addition, the lost to follow up cases were relatively healthy so we feel it may have an impact on the overall results of this study.
Despite the fact that aforementioned reasons limit the study, the prospective data collection from multiple data collection points using skilled and well trained health professionals were enabled us to measure the pattern of maternal morbidity conditions during pregnancy, delivery and over the postpartum period. In addition, procedures such as supervision, pretest of data collection tool, and adequate training of data collectors and supervisors were helped us to improve the data quality.
The occurrence of postpartum morbidity, low birth and still birth among pregnant women attending & giving birth at health institution in Gondar town was significant health concern. Intrapartum abonormalities were the main predictive factor triggering maternal morbidity conditions. The time from birth to the first 6 hrs of purperum was the peak time to postpartom hemorrhage. Therefore, interventions such as universal use of the partograpgh, active third stage management and encouraging all delivering women to stay in the health institution during the first 24 hours of delivery could play a key role in reducing postpartum morbidity.
• As a starting point for reducing postpartum morbidity physicians, midwives and other maternal health care providers need to strictly follow laboring mothers with partograph to detect and manage risk factors that cause labor abnormality.
• It would be advisable to keep prennial tear and epiziotomy at lower rate
• All deliverying mothers need to be assessed carefully during the first 6 hours of delivery and it would be good if they stay for 24 hours in the health institutions for observation as it was recommended by safe motherhood programs, especialy if they have encountered any form of labour abnormality.
• There is a need to increase awarness of all women about the level of postpartum morbidity prevailing during delivery and postpartum period. Moreover, we recommend maternal health care providers to educate and sensitize all pregnant women to give birth in the health institution and utilize postpartum care services while they provide ANC.
• Strengthen a well organized and equiped maternal and neonatal health care service that can provide all essential cares Interms of infrastracture, skilled man power and supplies.
• Strengthen monitoring and evaluation system for ANC, delivery and posnatal care.
• Conduct surveys that include the different segment of population and definitive investigation tools on maternal morbidity, to monitor changes across populations and care practices in different regions of Ethiopia.
• Evidence based best care practices and guidelines need to be made available, to improve obstetric care during intrapartum and reduce postpartum morbidity, emphasizing postpartum hemorrhage. Women, who did supplement with iron antenatally, would have a significantly improved physiological response to a PPH in comparison to a woman who delivered with a borderline hemoglobin status
We would like to forward our heartfelt thanks to Professor Yigzaw Kebede for his indispensable comments and advice during this paper work. We thank our entire data collectors for their unreserved and dedicated cooperation to make this paper work come out true. Our acknowledgement also goes to all study participants for their exceptional cooperation and to their punctuality to the study follow ups. We also would like to present our heartfelt thanks to University of Gondar for the valuable support and funding the paper. At last but not least, we thank people who are working at the Gondar zone and Gondar town health departments; antenatal clinics of Gondar hospital, Family Guidance Association, Gondar, Azezo, and Maraki health centers for their indispensable information and cooperation.