Fungal Genomics & Biology
Open Access
ISSN: 2165-8056
ISSN: 2165-8056
Research Article - (2016) Volume 6, Issue 1
Background: Granulomatous prostatitis is an uncommon inflammatory process of the prostate, which in most cases, is nonspecific. Clinical presentation, treatment, and evolution are similar to those of benign prostatic hypertrophy, but this lesion is also a clinical mimicker of prostate. Fungal granulomatous prostatitis is rare and there are only a few reported cases.
Clinical case: We report the case of a patient diagnosed with prostatitis blastomycosis. The patient had obstructive and irritative lower urinary tract symptoms, which showed slight improvement the first days of medical treatment. Finally, he underwent transurethral resection of the prostate due to the persistence of the obstructive symptoms.
Results: The histopathologic result showed granulomatous prostatitis with features of blastomycosis fungal structures. Diagnosis was confirmed through molecular biology techniques.
Conclusion: Despite its low incidence, the diagnosis of fungal granulomatous prostatitis is important to keep in mind, because it can mimic other prostatic pathologies.
Keywords: Blastomycosis, Granulomatous prostatitis, Fungal prostatitis
Granulomatous prostatitis is an unusual benign inflammatory process [1]. It is a heterogeneous entity encompassing infectious, iatrogenic (post-surgery), or idiopathic (nonspecific) lesions, malakoplakia, and other cases associated with systemic granulomatous disease, such as Wegener granulomatosis and allergy [2]. Nonspecific granulomatous prostatitis is the most common type [1,3], and the most frequent etiologic factor is surgery (transurethral resection) or prostatic needle biopsy [4,5]. Clinical presentation may be similar to that of benign prostatic hypertrophy or it may even be clinically indistinguishable from that of prostate carcinoma [6], since it is frequently associated with an abnormal digital rectal examination [7], an elevated prostate-specific antigen (PSA) [8], or both. Infectious granulomatous prostatitis can be caused by Mycobacterium tuberculosis [9,10], BCG instillation for transitional cell carcinoma of the bladder [11,12], syphilis [13], malakoplakia [14], viruses [15], and various fungi [16]. Fungal granulomatous prostatitis is rare [17]. The fungal species that most frequently cause prostatitis are candida, aspergilla, and cryptococcus. The patients that are at higher risk for developing fungal infections are chronically ill, debilitated, and immune-compromised. Other factors include changing patterns of patient demographics that increase environmental exposure [18]. There are few cases of prostate affection reported as an initial presentation of blastomycosis in the literature. The case presented here is interesting because of its low incidence and potential to mimic other prostatic diseases including malignancy, justifying our report.
A 70-year-old man, born and raised in a rural community (Cerralvo) in the north-eastern Mexican state of Nuevo León, stated in the medical interview that he had no pathologic history of diabetes, high blood pressure, or any immunodeficiency. The patient said he was a farmer and denied having travelled to other regions of North America in recent years. His deficient hygiene habits were apparent, but his nutritional status was adequate. The patient came to the emergency room due to acute urinary retention and bladder distention and he complained of having irritative and obstructive urinary symptoms for the past 6 months. Upon physical examination a Grade II-III prostate was found. A Foley catheter was placed and 1500cc of urine was drained. He was discharged with an appointment at the urology outpatient clinic. Ten days later the patient was re-admitted to the emergency room presenting with fever, pallor, and haematuria. Abnormal laboratory findings included neutrophilia on complete blood count and a PSA of 8.3 ng. Transrectal ultrasound was performed showing a marked distention of the bladder and a bladder calculus. The prostate showed a moderate increase in size measuring 4.76 x 5.3 x 4.4 cm and a volume of 59.4 cc, with heterogeneous echogenicity and borders with a lobular appearance. The initial clinical diagnosis was benign prostatic hypertrophy complicated by acute prostatitis; however, due to the increase in PSA and the ultrasound characteristics, a transrectal biopsy (TRB) was decided upon to rule out other prostate pathologies, mainly carcinoma. Using the traditional hematoxylin and eosin technique, the histologic TRB sections revealed a predominantly lymphocytic inflammatory process, with scarce epithelioid histiocytes that clumped together and formed granulomas; giant cells were also observed (Figure 1 and 2). Yeast fungal structures were identified inside these giant cells and granulomatous formations and Grocott staining was performed to study the morphologic characteristics of these fungal structures; they measured 8 to 15 microns in width and showed broad-based budding. These findings led to the diagnosis of granulomatous prostatitis associated with fungal structures consistent with blastomycosis. Diagnosis was confirmed through molecular biology techniques. Total genomic DNA was extracted from a slice of paraffin-embedded tissue that then underwent PCR to amplify fungal ribosomal RNA sequences (ITS1-5.8S ribosomal RNA-ITS2) with the ITS4 (TCCTCCGCTTATTGATATGC) and ITS5 (GGAAGTAAAAGTCGTAACAAGG) consensus primer set [18]. The amplification product of 666 base pairs (bp) were sequenced for both borders, assembled, and used as a hook in the Basic Local Alignment Search Tool (BLAST) of the NCBI. The results were 100% Ajellomyces dermatitidis (anamorph Blastomyces dermatitidis). Imaging studies were ordered and the patient underwent a thorough physical examination to rule out a systemic condition. Pulmonary involvement was intentionally evaluated and imaging studies and examination identified no abnormalities. The patient began medical treatment with 400 mg daily of itraconazole p.o. for 6 months. After one week of treatment the patient showed slight improvement, but due to the persistence of the obstructive symptoms, it was decided to perform a transurethral resection of the prostate (TURP). Histologic tissue sections from the TURP showed the same findings previously described in the TRB, supporting the diagnosis of granulomatous prostatitis due to prostatic blastomycosis. The TURP resolved the obstructive urinary symptomatology and the patient were released from the hospital to continue his treatment as an outpatient for at least 6 months. He was asymptomatic at that last follow-up visit.
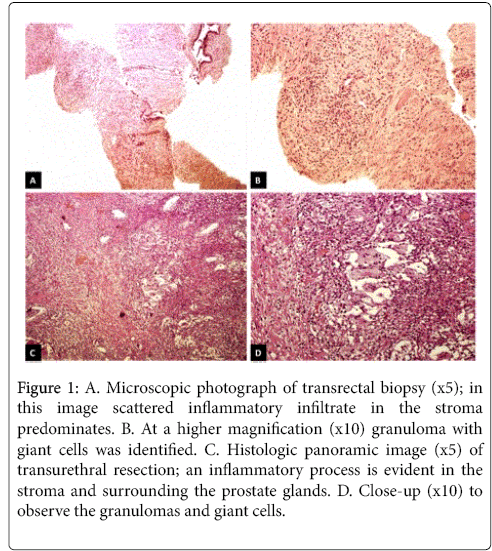
Figure 1: A. Microscopic photograph of transrectal biopsy (x5); in this image scattered inflammatory infiltrate in the stroma predominates. B. At a higher magnification (x10) granuloma with giant cells was identified. C. Histologic panoramic image (x5) of transurethral resection; an inflammatory process is evident in the stroma and surrounding the prostate glands. D. Close-up (x10) to observe the granulomas and giant cells.
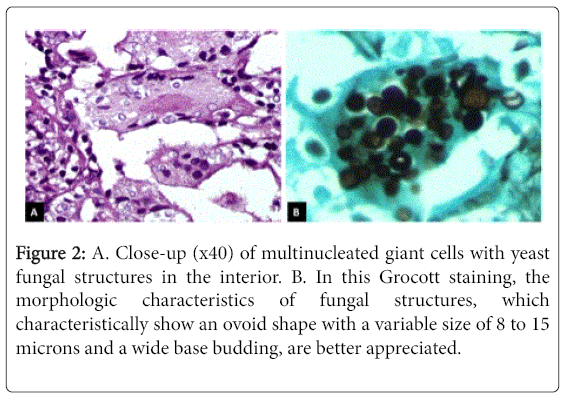
Figure 2: A. Close-up (x40) of multinucleated giant cells with yeast fungal structures in the interior. B. In this Grocott staining, the morphologic characteristics of fungal structures, which characteristically show an ovoid shape with a variable size of 8 to 15 microns and a wide base budding, are better appreciated.
The genitourinary system is a target for fungal infections such as Candida, Cryptococcus and Aspergillums, Blastomyces, Coccidioides, and Histoplasma, which can be present and are more aggressive in vulnerable patients [19]. Blastomyces dermatitidis is a dimorphic fungus that predominates in North America and is endemic to the Ohio and Mississippi River Valley regions, which is why this fungal infection is also known as North American Blastomycosis, Chicago disease, and Gilchrit's disease [20]. Blastomycosis usually presents as a systemic infection. It is acquired after inhaling the infectious conidia that is aerosolized as the mycelial form of the fungus growing as a saprophyte in soil, and thus, in most cases, the lungs are the primary focus of infection. Primary cutaneous infection is rare and is usually caused by accidental inoculation in clinical microbiologists and pathologists; it has also occurred following dog bites [21]. There is no racial predilection, but the male-to-female ratio is as high as 15 to 1 [22]. Most cases of pulmonary blastomycosis are asymptomatic and self-limiting in immunocompetent patients, but may spread from the lung to other organs hematogenously. Like most other fungal infections, severely immunodeficient patients are at increased risk for blastomycosis [23]. The organs most commonly affected are the skin, larynx, bones and joints, central nervous system, lymph nodes, heart, adrenal gland, and the genitourinary tract [24]. Eickenberg et al. [25] carried out a retrospective study of 51 cases of systemic blastomycosis. Eleven patients (21.5%) were found to have genitourinary involvement, with the prostate and epididymis being the most commonly affected sites. Clinically, prostate involvement presents with dysuria, nicturia, urinary retention, perineal or suprapubic pain, haematuria, and hematospermia. It can also simulate bacterial prostatitis, benign hyperplasia, or carcinoma. An abnormal urologic exam can reveal induration of the prostate gland [26,27]. There are only a few reported cases of blastomycosis of the prostate in the literature to our knowledge (less than 10) [27]: one case presented with localized prostate involvement [28], two cases involved the prostate and epididymis [26,29], two cases involved the prostate and skin [30,31], and a final case of systemic dissemination was initially diagnosed by transrectal prostate biopsy [32]. In tissue sections typical yeast-like cells are morphologically distinctive. They are spherical, hyaline, 8 to 15-microns in diameter, multinucleated, and have vacuolated cytoplasm and thick double contoured walls. The yeast-like cells reproduce by budding, and buds are attached to their parent cells by broad bases [24]. The predominant inflammatory reaction in the lesions of acute blastomycosis is suppurative, with infiltration of neutrophils and abscesses. Fungal cells are usually extracellular, numerous, and scattered in the lesions or localized to abscesses. In chronic lesions, there is a mixed suppurative and granulomatous inflammatory reaction with classic granulomas composed of compact epithelioid histiocytes, giant cells, lymphocytes, and fibroblasts, but caseation and calcification are uncommon [21]. Whenever fresh tissues are available, microbiologic culture should complement histopathologic studies [33]. Because the yeast forms of Blastomyces dermatitidis and Histoplasma capsulatum or duboissi both have thick walls and are similar in size and shape, they can be mistaken for each other in tissue sections. The latter, however, usually bud by a narrower base, whereas the diagnostic budding from Blastomyces dermatitidis is broad-based [34]. Diagnostic confirmation through molecular biology was strength of the present report. It did not require fresh tissue and was carried out from paraffin-embedded tissue. The methodology employed was based on amplifying sequences that are common among fungi and customarily used for conducting phylogenetic studies. PCR using ITS4 and ITS5 primers amplifies ribosomal sequences of a wide variety of fungi and the sequencing of the product enables species identification. This methodology is interesting because it could aid in the diagnostic confirmation of pathologies in which fungi are microscopically visualized in biopsies, as occurred in the present case. Infectious granulomatous prostatitis requires medical treatment. Surgical management of granulomatous prostatitis leads to complications such as bladder neck contracture and requires repeated resection [1]. The current treatment of choice for blastomycosis is itraconazole, except for patients with central nervous system involvement and in cases of life-threatening infection in which amphotericin B should be used [27,32]. In the present case, urinary obstruction was resolved through TURP and itraconazole was also indicated. However, long-term disease progression could not be evaluated because patient follow-up was lost after 6 months.
Fungal granulomatous prostatitis is an uncommon simulator of other prostatic pathologies. It is a rare condition and the diagnosis of prostatic blastomycosis requires a high level of clinical suspicion, which is why physicians should be aware of this entity, especially in patients living in endemic areas and with a history of chronic urinary obstruction symptoms, and those diagnosed with chronic prostatitis.
All authors certify that they do not have any direct or indirect commercial financial incentive associated with publishing the article, and there was no source of extra- institutional commercial funding. All authors do not have any conflict of interests