Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Research Article - (2015) Volume 4, Issue 2
Background: Vitiligo is a common hypopigmentary skin disease that can affect the quality of life and has an impact on the psychological health of the patient. Unfortunately these aspects are usually missed in the care process and underestimated in the assessment and management of vitiligo patients.
Aim of the Study: To determine the quality of life and assess the psychological impact of Vitiligo among Saudi patients, to understand the variables which may influence their psychological wellbeing and to assess the association between the quality of life and psychological morbidity.
Methods: Using cross sectional design, 234 adult patients were recruited from different hospitals in Saudi Arabia between October 2010 and February 2011. Quality of life and psychological health were assessed by Dermatological Quality of life Index and Hospital Anxiety and Depression scale respectively, which are well known, widely accepted questionnaires.
Results: Quality of life was more affected in females, age group (21 -30) years, low income patients and patients with generalized vitiligo. Anxiety was noticed more in females and in patients with jobs which required dealing with people on daily basis. Depression was higher in less educated and low income patients. DQLI score positively correlated with the HAD scale.
Conclusion: Vitiligo has a large impact on quality of life and mental health. Psychosocial history should be assessed and considered in any patient with Vitiligo.
Keywords: Quality of life; Depression; Anxiety; Primary health Care
Our skin influences our appearance, and plays a major role in our social interactions [1]. Disfiguring of the skin due to any reason could be a potential source of emotional distress and mental illness [2]. It is a chronic, progressive hypopigmentary skin disorder. Many theories have been proposed for causality implicating immune, genetic, and environmental factors but none of them proven [3].
Vitiligo does not result in a direct physical impairment but it can influence the patient’s quality of life and psychological wellbeing [4].
Vitiligo patients suffer from poor body images, low self-esteem and sever social impairment [5], especially if the lesion is found in exposed areas such as face, hands or feet [3]. Due to its chronic nature, unpredictable course of remissions and relapses, long term treatment, and no curable therapy, its often affects the patient’s quality of life in different aspects of social activities, work, study and marriage [5]. In addition, it has an impact on patients’ feelings including embarrassment, shame, anxiety, depression and feeling of stigmatization because of their skin condition.
Many studies have been conducted worldwide demonstrating effects of vitiligo on quality of life and psychological health [1,3,4,6,7]. Homan, et al. [8] in 2009 found that dark skin and vitiligo on exposed body parts are associated with adverse psychological impact compared to patient with fair skin and lesions in non-exposed areas. Psamponga, et al. [9] showed very strong association between quality of life and psychological problems in vitilgo patients including worries of being worse with time, feeling of anger, embarrassment and shame. Dolatshahi, et al. [10] described a significant relationship between DQLI score and marital status especially among married women. Also they found DQLI score associated with disease of extended duration. Saleh, et al. [1] found that 24% of vitiligo patients have significant suicidal thoughts.
In Saudi Arabia Robaee et al. [3], conducted a study in AlQassim in 2007 shows that vitiligo has a severe impact on quality of life specially among those who are on light therapy and with a generalized involvement.
The purpose of this study was to measure the quality of life of patients with vitiligo and the effects of the disease on their mental health and its relationship with variables such as gender, age, education, and income and skin color.
Using a cross sectional study design, the study was conducted in dermatology clinics in both governmental and private sectors. From governmental sector the following centers were engaged: King AbdulAziz Medical City, National Guard (KAMC), Security Forces Hospital Program, and King Saud Medial Complex. From private sector the National Center for Vitiligo and Psoriasis (Light Clinics) participated. Data collected between October 2010 and February 2011.
Subjects were all adult patients’ ≥18 years who had vitiligo, of any type, and on topical or light therapy. We excluded patients who were diagnosed with any psychiatric illnesses before having vitiligo, patients who had any skin disease other than vitiligo, and patients with chronic illnesses.
The sample size was calculated using open epi epidemiologic calculator. Based on the assumption of a 15% prevalence of affective disorders among primary care visitors, the calculated sample size was 255, with 95% Confidence interval and margin of error ±5%. Subjects who presented to the primary care clinics during the period between october 2011 and February 2011 and met the inclusion criteria were recruited to the study by convenience untill the required sample size was satisfied.
Research assistants were trained on the study objective and questionnaire. They distributed the questionnaires and helped the patients understand and fill the survey form properly.
The questionnaire
The questionnaire composed of 4 parts: Socio demographic data, Information about vitiligo, Dermatology Quality of Life Index (DQLI) and Hospital Anxiety and Depression Scale (HAD) [11-13].
The DQLI was first described by Finally and Khan in 1994; it is composed of 10 questions the 1st and 2nd about the sign and symptoms of the dermatological disease, 3rd and 4th about daily activities, 5th and 6th about leisure, 7th about work and school, 8th and 9th about personal relationships, and the 10th question about the treatment. It gives the range from ‘no effect’ to ‘extremely large effect’ on the patient's life with score of 0-3. We calculated the answers of all questions, so the total in minimum is 0 and the maximum is 30.
The HAD scale is composed of 14 questions, 7 to assess depression, and 7 to assess Anxiety. Each question is given a score of 0-3. The total minimum score is 0 and the maximum is 21 with a range from (0-7) normal, (8-11) patients are at risk and should be of concern to the doctors, and (12-21) patients need to be assessed by a psychiatrist.
Data analysis
Data entry, Statistical analysis and statistical tests were done using SPSS package version 20.
Data was analyzed descriptively with mean, median, modes, standard deviations, frequencies and percentages. Further analysis was carried out using chi square, t-test, ANOVA and linear regression.
P value was considered to be significant at ≤ 0.05.
Ethical Approval: Ethical approval was obtained from the Institutional review board of King Abdullah International Medical Research Center (KAIMRC).
Two hundred and thirty four Saudi patients were involved in our study. Seventy-four percent were from Riyadh and rest from Abha and Jeddah. The age range was (18–66) years (mean: 30.8 SD ±11.23). Twenty-one percent were under the age of 20 years, 39% of patients were between 21- 30 year old and only 17.5% older than 40 year. The mean age of having vitiligo found to be 21.4 years (±SD 12.98). The mean duration of vitiligo was 9.5 years (± SD 8.09), and the mean of duration of vitiligo treatment was 5.92 years (SD ± 5.99). 52% were males. Single patients were 51.6% and 48.4% were married. Above 41% were found to have a university degree and above. About 45% had income less than 5000 SR / month (Table 1).
| Characteristic | Frequency | Percentage |
|---|---|---|
| Location | ||
| Inside Riyadh | 173 | 73.9 |
| Outside Riyadh | 61 | 26.1 |
| Institution | ||
| Governmental Sector | 106 | 45.3 |
| Private Sector | 120 | 54.7 |
| Gender | ||
| Male | 123 | 52.6 |
| Female | 111 | 47.4 |
| Age Groups (years) | ||
| ≤20 | 49 | 20.9 |
| (21-30) | 91 | 38.9 |
| (31-40) | 53 | 22.6 |
| >40 | 41 | 17.5 |
| Marital Status | ||
| Single | 115 | 51.6 |
| Married | 108 | 48.4 |
| Educational Level | ||
| Elementary and Intermediate | 53 | 23 |
| High School or Diploma | 82 | 35.7 |
| University or above | 95 | 41.3 |
| Monthly Income (SAR) | ||
| ≤5000 | 106 | 45.3 |
| 5001-10.000 | 73 | 31.2 |
| >10.000 | 55 | 23.5 |
| Public job | ||
| Yes | 134 | 57.3 |
| Sometimes | 45 | 19.2 |
| No | 55 | 23.5 |
| Type of Family | ||
| Alone | 14 | 6 |
| Nuclear Family | 199 | 85 |
| Extended Family | 21 | 9 |
Table 1: Characteristics of the Study Subjects
Majority of the patients (59.8%) had a medium skin color. Positive family history of vitiligo was in 38.9%, with 72.2% first degree relatives (Table 2).
| Disease Characteristic | Frequency | Percentage |
|---|---|---|
| Skin Color | ||
| Fair | 53 | 22.6 |
| Medium | 140 | 59.8 |
| Dark | 41 | 17.5 |
| Family history of Vitiligo | ||
| Yes | 91 | 38.9 |
| No | 143 | 61.1 |
| Type of relationship of positive family history | ||
| First Degree | 65 | 27.8 |
| Second Degree | 25 | 10.7 |
Table 2: Disease related characteristics
The mean percentage of affected area was 27.66% (±SD 21.55) and 88.5% of the patients had 50% involvement of their body. Involvement of the face was in 38%, hands 62.4%, feet 56.8% and only 12% of the whole body. Among single patients, 29% reported that vitiligo is the cause of being unmarried and for 42% it was not an issue for being unmarried. 19.2% of married people admitted that vitiligo caused some marital problems. Regarding their experience with other people, 32.3% suffered from strange looks from others due to their skin condition, 35.6% would avoid marriage in families that had someone with vitiligo. 15.4% thought it was an infectious disease, 42% consider it as an inherited disease (Table 3).
| Social effect | Frequency | Percentage |
|---|---|---|
| Cause of being unmarried | ||
| Yes | 36 | 29 |
| No | 52 | 41.9 |
| I Don't Know | 36 | 29 |
| Cause of marital problems | ||
| Yes | 24 | 19.2 |
| No | 87 | 69.6 |
| I Don't Know | 14 | 11.2 |
| Strange looks | ||
| Yes | 75 | 32.3 |
| No | 103 | 44.4 |
| I Don’t Know | 54 | 23.3 |
| Avoid marriage from families with Vitiligo | ||
| Yes | 77 | 35.6 |
| No | 44 | 20.4 |
| Sometimes | 95 | 44 |
| Vitiligo is Infectious Disease | ||
| Yes | 36 | 15.4 |
| No | 130 | 55.6 |
| Some people | 68 | 29.1 |
| Vitiligo is Inherited Disease | ||
| Yes | 98 | 41.9 |
| No | 48 | 20.5 |
| Some People | 88 | 37.6 |
Table 3: Social effects of vitiligo
The mean score of DQLI for all cases was 8.72 (±SD 6.09) and 33.8% of the patients had ‘very large’ to ‘extreme’ effect on their quality of life. Physical symptoms like itching were reported in more than 60% of the patients with about 14% reporting it as severe. Near 80% admitted that they feel embarrassed because of their skin with almost half of those report the feelings as extreme. Over 17% said that their personal relationships were extremely affected. Choosing of clothes was ‘very much’ affected in almost 40% of the patients. Vitiligo treatment affected the patient's life in nearly 84% (Tables 4 and 5).
| Parameter | Extremely affected (%) | A Little (%) | Not at All/ Not relevant (%) |
|---|---|---|---|
| Symptoms | 33(14.1) | 110(47) | 91 (38.9) |
| Feelings | 90(38.5) | 96 (41) | 48 (20.5) |
| Shopping | 39(16.6) | 57 (24.4) | 138 (59) |
| Clothes | 91(38.9) | 46(19.7) | 97 (41.4) |
| Social | 38(16.2) | 50 (21.4) | 146 (62.4) |
| Sport | 37(15.8) | 42 (17.9) | 155 (66.3) |
| Working or Studying | 17 (8.5) | 72 (35.8) | 112 (55.7) |
| Relationships | 41(17.5) | 68 (29.1) | 125 (53.4) |
| Sexual | 30(12.8) | 26(11.1) | 178 (76.1) |
| Treatment | 135(57.7) | 61 (26.1) | 38 (16.3) |
Table 4: Distribution of patients related to Dermatology Quality of Life Index
| Factors | No or Small effect{No (%)} | Moderate effect{No (%)} | V. large/ extreme effect{No (%)} | Chi sq (P value) |
|---|---|---|---|---|
| Gender | ||||
| Male | 58 (64.4) | 39 (6.0) | 26 (32.9) | 18.77(0.00) |
| Female | 32 (35.6) | 26 (40) | 79 (67.1) | |
| Age group (years) | ||||
| ≤ 20 | 15 (16.7) | 12 (18.5) | 22 (27.8) | 13(0.04) |
| 21- 30 | 36 (40.0) | 28 ( 43.1) | 27 (34.2) | |
| 31-40 | 15 (16.7) | 18 (27.7) | 20 (25.3) | |
| > 40 | 24 (26.7) | 7 (10.8) | 10 (12.7 | |
| Marital status | ||||
| Single | 42(47.7) | 29(46.8) | 44(60.3) | 3.3(0.19) |
| Married | 46 (52.3) | 33(53.2) | 29 (39.7) | |
| Education | ||||
| 1ry/ 2ry school | 19(21.3) | 9 (14.1) | 25 (32.5) | 8.4(0.76) |
| High school or diploma | 30( 33.7) | 24(37.5) | 28(36.4) | |
| University | 40(44.9) | 31 (48.4) | 24(31.2) | |
| Public job | ||||
| Yes | 57(63.3) | 38(58.5) | 39(49.4) | 6.5(0.15) |
| Sometimes | 14(15.6) | 16(24.6) | 15(19) | |
| No | 19(21.1) | 11(16.9) | 25(31.6) | |
| Monthly Income (SR) | ||||
| ≤5000 | 27( 30) | 29( 44.6) | 50( 63.3) | 21(0.00) |
| 5001-10.000 | 32( 35.6) | 23(35.4) | 18(22.8) | |
| >10.000 | 31 ( 34.4) | 13(20) | 11 (13.9) | |
| Skin color | ||||
| Fair | 23 (25.6) | 11(16.9) | 19(24.1) | 3.65(0.45) |
| Medium | 55(61.1) | 42 (64.6) | 43(54.4) | |
| Dark | 12(13.3) | 12(18.5) | 17(21.5) | |
Table 5: Relationship of DQLI with variables
DQLI
DQLI was worse in female where 47.7% of them had ‘very large’ to ‘extreme’ effect while in males this effect was seen only in 21.1% (chi-sq.=18.77, p<0.001). Higher DQLI score was seen in age group (21-30 years) compared to other age groups (chi- sq.=13, p=0.043). DQLI score was higher among low income patients compared to high income patients (chi sq.=21, p<0.001).
Involvement of the neck had a significant impact on quality of life rather than other parts of the body (mean DQLI score t-test=2.21, p<.028, mean diff.=2.2).
Patients who had involvement of >50% of body surface had more effect on quality of life index (t-test=2.15, P=0.013).
The difference of DQLI among marital status, educational level, skin color or for those in public jobs dealing with people, was found to be statistically insignificant.
HAD scale
Regarding anxiety the mean score of HAD scale was 5.94 (± SD 4.51) and mean score for depression was 4.90 (±SD 4.06). Anxiety was common among females with 62.7% having ‘high’ score while only 37.3% in males had ‘high’ score (chi sq. 10.27, p<0.001). Anxiety was higher in patients dealing with people on daily basis (chi sq. 10.12, p= 0.006), in contrast to HAD scale for depression, where dealing with people had no significant effect.
Vitiligo on the face has been associated with significant anxiety than any other part of the body (mean HAD anxiety score t-test=2.31, p=0.022, mean diff.=1.382) (Table 6).
| Variable | HAD scale for Anxiety | HAD scale for Depression | |||||
|---|---|---|---|---|---|---|---|
| Normal{No (%)} | High{No (%)} | Chi sq (p) | Normal{No (%)} | High{No (%)} | Chi sq (p) | ||
| Gender | Male | 95 (59.7) | 28 (37.3) | 10.3 (0.00) |
96 (56.5) | 27(42.2) | 3.8 (0.05) |
| Female | 64 (40.3) | 47(62.7) | 74(43.5) | 37(57.8) | |||
| Age group | ≤20 | 30 (18.9) | 19(25.3) | 3.72 (0.29) |
38(22.4) | 11(17.2) | 1.8 (0.61) |
| 21- 30 | 68(42.8) | 23(30.7) | 67(73.6) | 24(37.5) | |||
| 31-40 | 33(20.8) | 20(26.7) | 35(20.6) | 18(28.1) | |||
| >40 | 28(17.6) | 13(17.3) | 30(17.6) | 11(17.2) | |||
| Marital Status | Single | 74 (48.1) | 41(59.4) | 2.4 (0.12) |
85(51.8) | 30(50.8) | 0.17 (0.89) |
| Married | 80(51.9) | 28(40.6) | 79(48.2) | 29(49.2) | |||
| Education | Primary/Secondary school | 32(20.3) | 21(29.2) | 5.26 (0.07) |
32(19.2) | 21(33.3) | 6.6 (0.037) |
| High school or diploma | 53(33.5) | 29(40.3) | 59(35.3) | 23(36.5) | |||
| University | 73(46.2) | 22(30.6) | 76(45.5) | 19(30.2) | |||
| Public job | Yes | 102(64.2) | 32(42.7) | 10.1 (0.00) |
105(61.8) | 29(45.3) | 5.4 (0.065) |
| Sometimes | 24(15.1) | 21(28.0) | 28(16.5) | 17(26.6) | |||
| No | 33(20.8) | 22(29.3) | 37(21.8) | 18((28.1) | |||
| Monthly income (SR) | ≤ 5000 | 66(41.5) | 40(53.3) | 3 (0.22) |
68(40.0) | 38(59.4) | 7.1 (0. 028) |
| 5001-10.000 | 54(34) | 19(25.3) | 59(34.7) | 14(21.9) | |||
| >10.000 | 39(24.5) | 16(21.3) | 43(25.3) | 12(18.8) | |||
| Skin color | Fair | 34(21.4) | 19(25.3) | 0.46 (0.79) |
37(21.8) | 16(25) | 0.39 (0.819) |
| Medium | 97(61) | 43(57.3) | 102(60) | 38 (59.4) | |||
| Dark | 28(17.6) | 13(17.3) | 31(18.2) | 10(15.6) | |||
Table 6: Relationship of HAD scale with variables
No difference was noted in Anxiety score between different age groups, marital status, income, educational level, skin color or extended duration of the disease.
In HAD scale for depression we found a higher score in females 57.8% compared to 42.2% in males but this difference was borderline insignificant (chi sq. 3.8, p=0.051).
Over 45.5% of ‘normal’ depression scale was seen in high educational level (university and above) while 19.2% of normal scale seen in low educational level (chi-sq. 6.6, p=0.037).
Nearly 60% of ‘higher’ depression score was seen in patients with low income while only 18.8% of ‘high’ score was noted in the high income bracket (chi-sq. 7.15, p=0.028.)
We did not find a significant association between the HAD for Depression and physical distribution of vitiligo.
Similar to HAD scale for anxiety, no effect was seen on depression scale for skin color, marital status, different age groups or extension of the disease.
There was a significant difference between ‘high’ scores in both scales (DQLI and HAD for both Anxiety and Depression) and frustration of treatment, (t-test 5.77, 7.58 and 3.827 respectively, p <0.001).
For suicidal thoughts both DQLI and HAD for Anxiety (t test 4.2 and 4.7, p<0.001 respectively) and for HAD scale for Depression
(t test=2.31, p=0.022,).
The mean score for DQLI of suicidal attempts was 21.67 (SD + 4.93) which was significantly higher from those who did not attempt suicide (t test=3.8, p<0.001), as well for HAD scale where the mean score for Anxiety was 15.33 (SD + 4.04) and for Depression was 9.67 (SD + 3.21), (p<0.001, t test=3.733 and p=0.041 t test=2.06 respectively).
A moderately positive correlation was noted between the DQLI and HAD scale for anxiety, where the patients with poorer quality of life had a higher HAD anxiety score (R2=0.35, p<0.001). The same for HAD scale for Depression (R2=0.28, p<0.001). (Figures 1 and 2).
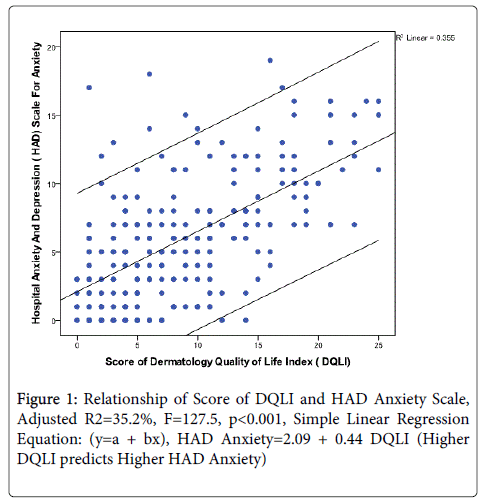
Figure 1: Relationship of Score of DQLI and HAD Anxiety Scale, Adjusted R2=35.2%, F=127.5, p< 0.001, Simple Linear Regression Equation: (y=a + bx), HAD Anxiety=2.09 + 0.44 DQLI (Higher DQLI predicts Higher HAD Anxiety)
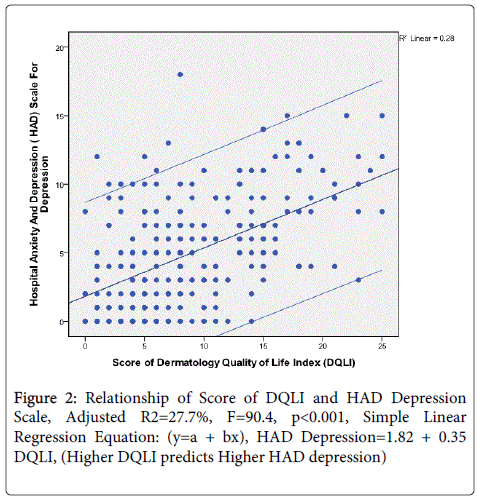
Figure 2: Relationship of Score of DQLI and HAD Depression Scale, Adjusted R2=27.7%, F=90.4, p< 0.001, Simple Linear Regression Equation: (y=a + bx), HAD Depression=1.82 + 0.35 DQLI, (Higher DQLI predicts Higher HAD depression)
Vitiligo has a very large effect on quality of life and psychological wellbeing. In most skin conditions psychiatric morbidity was strongly associated with poorer quality of life [7]. The mean DQLI in this study was 8.72(±SD 6.09) which was less than the score reported in 109 patients by AlRobaee in alQassim study, i.e. 14.72 [3], Compared to international studies we have a higher score than Kent et al. Abadie [14], where they found score of 4.82 in UK, as well in Ongenae et al. [4] study in Belgian patientswho had a mean total score of 4.95. Our findings are near the results of Finaly and Khan [15] who had a DQLI score of 7.3 in UK study, and in the same category 10.67 reported by Parased et al. [16] in India.
In our study we found females more affected than males with higher DQLI score, unlike the AlRobaee [3], Parsad et al. [16], and Kent and Abadie [14] who did not report any gender difference in score, while Ongenae et al. [4], Do Young Kim et al. [6] and Sampogna et al. [9] found that women overall had a higher score than men. We expected this finding as women are more concerned about her skin and beauty. Age also influenced DQLI where the highest effect about 34.2% was seen in age group of 21-30 years while this effect decreased to 12.7% in patients older than 40 years. This is expected as younger people are usually more concerned about their appearance.
Other factors found to have a significant effect on the quality of life was income, where 63.3% of ‘very large’ or ‘extreme’ effect was seen in low income category while 13.9% of the same effect seen in high income group. Low income patients have more life stressors beside vitiligo which can be a burden on opportunities. We found that involvement of the neck has been associated with a significant impact on quality of life more than any other part of the body. This may be due to cultural differences. In other studies like in Tunisia, they found that exposed areas have a higher impact on quality of life than non-exposed parts of the body [5].
Interestingly we found no effect of skin color on quality of life. Linborst Homan et al. In Amesrtdam reported that subjects with darker skin are more anxious about their appearance [8].
As expected we found that patients with generalized and more body surface involvement have more impact on their quality of life, the same seen in previous studies [3,4].
Although Vitiligo is considered to be idiopathic, there some theories saying that stress is one of the causes, [2,7,8]. We assessed our patients for the possibility of psychiatric illness using the HAD scale, which can differentiate between people who are normal and who need to have further evaluation and assessment.
The mean score for HAD scale for Anxiety was 5.94 (±4.51 SD), and for depression was 4.90 (±4.06 SD) where we found that 62.7% of high anxiety seen in females comparing to 37.3% in males (p<0.001) as well in depression scale a 57.8% of high reading was in female and 42.2% in male (p=0.51) even this difference was insignificant, but we think that female have a higher potential to have anxiety as well as depression more than males [2].
As in DQLI, we found that income had a psychological impact where HAD scale for Depression was high on patients with low income with a 59.4% as compared to 18.8% in patient with low income. While Anxiety scale was not affected by the income, on the other hand, it was high in patients who were dealing with people on a daily basis as job requirement.
This interaction with other people perhaps puts vitiligo patients under stress due to different reactions that are expressed towards them. Over 32.3% of people get strange looks due to their skin condition and 14.5% of people think that vitilgo is an infectious disease all of these factors may cause burden on patients and increase their level of anxiety, interestingly DQLI and Depression scale were not affected by public dealing jobs.
In contrast to both DQLI and Anxiety scale we noticed that depression scale was associated with educational level as 45.5% of those with university degree were normal on depression scale compared to only 19.2% of those who had a low educational level (p=.037), this can be explained by assuming that more educated people can understand their disease and its chronic nature which may help them in the acceptance and compliance of long treatment regimen.
HAD for anxiety as well as for depression didn’t report any significant association with age, but we noticed some pattern where high scores were reported with age group 21-30 years, as same category where DQLI showed a significant effect. This is supported by Ijaz Ahmed study were they report that psychiatric illness was predominant in patients below 30 years of age [2].
Surprisingly we found no association with marital status or skin color with either DQLI or HAD scale for both Depression and Anxiety. On the contrary, literature reported higher psychological problems seen in unmarried subjects [2]. In our study 46.2% were married and 53.8% were single, among those singles 41% thought that vitiligo is not a cause of being unmarried. Family history of vitiligo was seen in 38.9%, and only 35.6% believed that people avoid marriage from families that have vitiligo. Nearly 70% of the married patients said that vitiligo was not a cause of any marital problems and 87.2% stated it has no sexual difficulties due to their disease.
Regarding the skin color 60% had a medium skin color, most of the literature indicates that darker skin color had more stress on patients with vitiligo, however that was not noticed in our study, perhaps because only 17% reported their skin as ‘dark’ and they did not express higher impairment.
Patients with face involvement were found to be suffering from anxiety rather than depression, in the literature it was reported that patients with exposed area affected have more psychiatric disorders [2].
We found that the patients who had a large effect on ‘quality of life’ scale had an abnormal HAD score for both Depression and Anxiety. The higher the quality of life impairment, the higher will be the chance of developing psychological problems as depression or anxiety. This association was seen also in Sampogana et al. Study 2004 [7], Mechri et al. in Tunisia 2006 [17] and HananSaleh study in Egypt 2008 [1].
The DQL index assesses the effect of any dermatological disease during the last 2 weeks and might not reflect the long term implications of the disease.
This study demonstrates that vitiligo has a negative effect on quality of life and it can be a probable cause of psychological diseases. More attention should be focused on female, low income patients as they may have a more severe impairment. Patients who have a poor quality of life should be screened for depression and anxiety as there is an association between them.
Patients with vitiligo need more attention from both dermatologist as well as family physician, even its not a serious or life threatening disease but it has large effect on quality of life, its psychological and psychiatric consequences need to be evaluated and proper action should be taken, especially in low income, low educational level, and young age group.
Involving a psychiatrist or psychologist may be appropriate step in management of high risk patients. Having patient support groups may be a good forum for exchanging their experiences with other patients locally or internationally.