Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2015) Volume 4, Issue 1
Percutaneous ultrasound-guided Radiofrequencyablation (RFA) is a minimally invasive treatment that has been widely used as an alternative to surgery in the care of patients with malignant tumors of the liver, renal cell carcinoma, and other tumors. Recently, RFA is an alternative treatment modality for benign thyroid nodules instead of surgery, mainly for the cosmetic reasons, and limited cases of local recurrences or focal distant metastases of differentiated thyroid cancer in the high-risk reoperative condition or for the palliative purpose. However, RFA for the initial treatment of the DTC is rare. We report a case of RFA for the papillary thyroid microcarcinomain the high-risk surgical patient. A 49-years-old woman with congestive heart failure due to severe mitral valve regurgitation, chronic kidney disease, and type 2 diabetes was incidentally diagnosed with papillary microcarcinoma without metastasis. She underwent RFA. During 5-year follow-up, there is no recurrence of the findings.
<Keywords: Catheter ablation; Papillary; Radiofrequency; Thyroid cancer
Radiofrequency (RF) ablation is an alternative treatment modality for benign thyroid nodules instead of surgery [1-3]. Surgery is a standard treatment for recurrent thyroid cancers, followed by radioactive iodine and thyroid hormone therapy. However, RF ablation can be used in patients with high risk of surgery and in patients who refuse to repeat surgery [4-6]. Papillary thyroid cancer (PTC) is the most common type of thyroid cancer and has a good prognosis. Especially, papillary thyroid microcarcinoma (PTMC) has usually a favorable outcome. The treatment of choice of PTC is surgery. Although most of patients with PTC can be effectively treated with thyroidectomy, surgery is impossible in patients who refuse surgery or have too high risk to undergo a surgical procedure. In these cases, alternative therapy such as RF ablation or laser thermal ablation can be used [7]. Here we present a case of PTMC patient who was treated by a non-surgical ultrasound (US)-guided RF ablation due to being under high surgical risk.
A 49-years-old woman with congestive heart failure due to severe mitral valve regurgitation and type 2 diabetes mellitus admitted in Daegu Catholic Medical center in 2008. Her chief complaint was a generalized edema. Urinary analysis showed macroalbuminuria and her creatine was 1.3 mg/dL. She was incidentally diagnosed with the nodule in the left thyroid gland on carotid US. The size of thyroid nodule was 7×6×8 mm and it was a hypoechoic nodule with calcification and irregular margin (Figure 1). US-guided fine needle aspiration (FNA) was performed and was consistent with PTC. We recommended surgery for PTMC. However, the patient refused surgery because of her heart condition. Neck US and chest computed tomography did not show the presence of lymph node or lung metastasis. Free T4 was 0.952 mg/dL (0.8-1.9), thyroid-stimulating hormone (TSH) was 2.67 IU/L (0.4-4.9). Calcitonin was within normal range (1.90 pg/mL). We proposed RF ablation for left PTMC on the basis of RF ablation clinical evidence about inoperable recurrent thyroid cancer treatment. And the patient agreed with our proposal.

Figure 1: Thyroid ultrasound showed an approximately 7×6×8 mm–sized hypoechoic nodule (arrow) with a calcification and irregular margin of the left lobe in the transverse view (A), and longitudinal view (B) during the first visit
Under sterile condition and after local anesthesia with lidocaine, RF ablation was performed in the patient according to the procedure previously reported with RF electrodes. We used 5 mm RF cooled electrode (Taewoong Medical, Kimpo, Korea). RF ablation was done with an RF generator (Taewoong Medical, Kimpo, Korea). Under continuous US guidance, RF electrode was positioned within the nodule and was performed. RF ablation began with 30-50 power. The procedure was well tolerated, without serious complications. The patient felt a mild discomfort and pain of the neck during RF ablation. Pain was resolved within several minutes and she did not require an additional medication after RF ablation. Post-treatment US showed 13×13 mm-sized hypoechoic lesion without vascularity in the left thyroid gland (Figure 2). At 6 month after RF ablation, thyroid US showed 6×4×6 mm-sized hypoechoic lesion in the left thyroid gland (Figure 3). Free T4 was 0.832 mg/dL and TSH was 4.76 IU/L in the blood test. She was diagnosed with chronic renal failure and started peritoneal dialysis in 2010. At 4-year follow-up after RF ablation, US showed 4×4×6 mm-sized hypoechoic lesion with internal macrocalcification in the left thyroid gland and did not show any abnormal lymph node of the neck. We performed FNA cytology to confirm the residual cancer in the RF ablation site. FNA cytology result showed no residual cancer. At 5 years after RF ablation, US showed 3×3×6 mm-sized hypoechoic lesion with internal macrocalcification (Figure 4). On follow-up, free T4 was 0.934 mg/dL and TSH was 4.22 IU/L. The nodule decreased in size compared to the previous. In the present, the general conditions of the patient are worsening due to chronic renal failure and congestive heart failure.
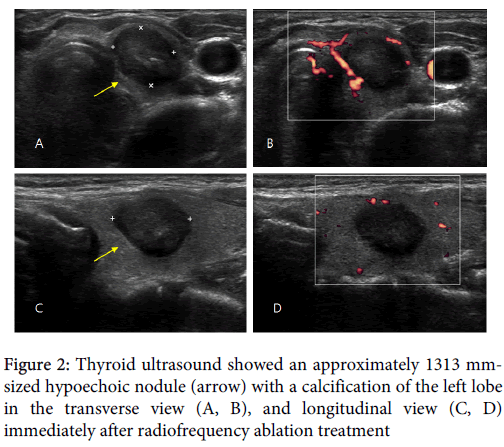
Figure 2: Thyroid ultrasound showed an approximately 1313 mmsized hypoechoic nodule (arrow) with a calcification of the left lobe in the transverse view (A, B), and longitudinal view (C, D) immediately after radiofrequency ablation treatment
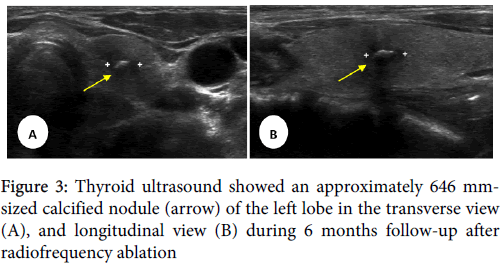
Figure 3: Thyroid ultrasound showed an approximately 646 mmsized calcified nodule (arrow) of the left lobe in the transverse view (A), and longitudinal view (B) during 6 months follow-up after radiofrequency ablation
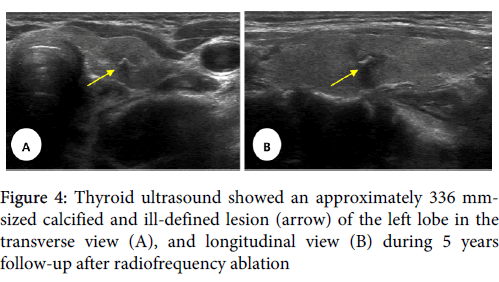
Figure 4: Thyroid ultrasound showed an approximately 336 mmsized calcified and ill-defined lesion (arrow) of the left lobe in the transverse view (A), and longitudinal view (B) during 5 years follow-up after radiofrequency ablation
The widespread use of cervical US in health screening has resulted in increasing number of incidentally discovered thyroid nodule and PTMCs in Korea. Most of cases of PTMCs show a good prognosis. Ito et al. reported they just observed in PTMCs patients who did not show unfavorable features without surgery and suggested PTMCs that are not associated with unfavorable features can be a candidates for observation without surgery [8]. Thyroidectomy is a safe method, nevertheless has some adverse effects such as decreased quality of life and weight gain in postoperative patients [9,10]. Some thyroidectomy patients complained fatigue, general weakness, depression, and anxiety. Total thyroidectomy patients had to take thyroid hormone replacement therapy during whole lifetime. US-guided laser ablation showed to be a potential therapeutic approach in incidental discovered PTMC patients with high-risk surgical patients in previous report [7]. Papini et al. reported they performed US-guided laser ablation on the elderly PTMC patients with high risk and found no locoregional recurrence or distant metastasis during 2-year follow-up period.
Following RFA, several investigators have reported a mean volume reduction of 56-93%, complete disappearance of 42-58.2% of tumors, therapeutic success rates of 75-91.6% [4-6,11,12]. The procedurerelated complications is neck discomfort, skin burn, and changes in voice. Serious complications, such as injury to the esophagus, trachea, or other nerves have not been reported following the treatment of recurrent thyroid cancers, which can be located near these structures [4-6,11,12]. In the present case, RF ablation of PTMC in high-risk surgical patient was performed rapidly and without any side effects and complications. If patient had received total thyroidectomy, patient could have been exposed to surgery and postsurgical acute complication. The left PTMC was completely ablated on the basis of post-treatment cytological and ultrasound findings. During 5-year follow-up, patient’s general condition was worsening due to the progression of renal function decreased. After RF ablation, patient was evaluated by annually clinical and US examinations, and no the evidence of the recurrence of thyroid cancer was apparent during 5- year follow-up. Ablation therapy of incidental PTMCs that appear unifocal and are confined to the thyroid gland on US may be used to reduce the risk of a local growth or extraglandular spread in high-risk surgical patients. Percutaneous ethanol injection (PEI) and thermal ablation have been proposed for the treatment of inoperable cervical lymph node metastasis [11]. PEI is reported as effective especially on the cystic nature nodule, and ethanol is randomly distributed and the size and shape of the coagulative necrosis area cannot be predicted [13,14]. In addition, PEI has a risk of ethanol leakage. Ethanol can be spread into the surrounding cervical tissues when injected to the metastatic cervical lymph node and cause a neck pain and posttreatment fibrosis [14]. Because of the limitation of PEI, laser or RF ablation seems to be more effective and safe for reducing the volume of solid thyroid lesions close to vital structures in the neck by welldefined necrosis area [15,16]. Shin et al. compared the effects of RF ablation and ethanol ablation on the treatment of recurrent thyroid cancer and summarized the efficacy seems to be higher in RFA, however the complications of procedure seem to be lower in ethanol ablation [11].
Recently, Ito et al. reported subclinical low-risk PTMC can be followed without immediate surgical intervention, with older patients potentially the candidates for observation approach [17]. Although PTMC in young patients (<40 years) may be more aggressive than that in older patients, they suggest it might not be too late to perform surgery after subclinical PTMC has progressed to clinical disease regardless of patient age. However, observation treatment is still inconclusive. The young PTMC patients may need an immediate treatment rather than observation. Therefore, RFA or laser ablation as the alternative treatment may be considered in the young low-risk PTMC patients who stubbornly refuse surgery.
In this case, RF ablation was a safe and prompt procedure for the ablation of PTMC without the evidence of extra thyroidal extension and lymph node metastasis. RF ablation can be safely performed as either outpatient or a day-hospital procedure for patients with significant comorbidities [18]. RF or laser ablation may be considered as the alternative treatment modalities in PTMC patients with high risk who decline to undergo surgery. However, clinical and radiological examinations for the extra thyroidal spread and lymph node metastasis in these patients should be completely evaluated before RF or laser ablation. Although the patients are high risk for surgery, RF or laser ablation is not recommended in them with suspected multifocal PTMC.