Advanced Techniques in Biology & Medicine
Open Access
ISSN: 2379-1764
ISSN: 2379-1764
Review Article - (2015) Volume 3, Issue 3
To measure the stiffness of the aorta, femoral artery and tibial artery noninvasively, cardio-ankle vascular index (CAVI) which was independent of blood pressure had been developed in cooperation of the Tohoku University and Fukuda denshi Co. The reproducibility had been studied, and the Independence from blood pressure has been studied till now. The results suggested that CAVI could reflect arteriosclerosis of the aorta, femoral artery and tibial artery. Furthermore we can evaluate the baroreflex sensitivity of an artery by the use of arterial tone. International cooperation study is ongoing now. So various scientific reports are easily found in pubmed. Medical device maker is now gathering these international papers for the presentation to the every doctor in the world for the achievements of better medical care. If the evaluation by this methodology in not so good, all doctors have a chance to use another devices. So, it is not necessary to use this method when the scientific papers showed another device had been good. Every doctor in all over the world must check recent progress in medical device in the scientific fields. By the use of the scientific, physical, quantitative methodology, evaluation of the atherosclerosis will be embodied in near future based on the normal value of every people in every country.
Keywords: Cardio ankle vascular index, Baroreflex, Pulse wave velocity, International cooperation
In order to diagnose arteriosclerosis in any part of the body, pulse wave velocity (PWV) measurement is a useful approach [1-3]. However, it is considered that the technique of PWV measurement should be simplified. A new method for measuring PWV has therefore been proposed in Japan. The PWV of the brachial artery and the ankle was measured by applying air pressure with the aid of a volume plethysmograph [3-5]. Comparisons between the baPWV measurement method and the conventional method are currently being performed. Since satisfactory results have been obtained to date, baPWV has gained popularity throughout Japan.
Since this method measures PWV in the arm and foot, it may be said that aortic PWV is not reflected though a large amount of past PWV measurements. BaPWV is influenced by blood pressure. With the baPWV technique, blood pressure compensation is not carried out. Furthermore, the pulse pressure is measured by air pressure; therefore any stimulus that exerts pressure on an artery may influence these results. Due to these reasons, a cardio-ankle vascular index (CAVI) has been proposed in which the pressure wave form indicating the closing of the aortic valve appears in the form of an arterial pressure wave after a fixed delay time [6-9].
Formula for measuring this index is:
CAVI=a{(2rho/DeltaP) x ln(Ps/Pd)PWV(2)} + b where, Ps and Pd are systolic and diastolic blood pressures respectively, PWV is pulse wave velocity between the heart and ankle, DeltaP is Ps-Pd, rho is blood density, and a and b are constants. This equation was derived from Bramwell-Hill's equation, and stiffness parameter.
Measurements of stiffness parameter of the Aorta and arteries are of course important in developed countries, because progression of the atherosclerosis causes a chronic artery disease that develops over many years without clinical symptoms.
Furthermore, it is an important point that the progression of atherosclerosis may be decelerated by intensive treatment of the main cardiovascular risk factors. Various kinds of medical studies have been carried out in all over the world. Soska V et al. [10,11] always have noted the importance of obesity in the prevention of the stiffness parameter progression, and a lot of researchers in many countries including Japan, USA, China, have showed the data concerning the obesity and CAVI in pubmed base.
In the world, the Russian data was the most interesting thing. Because the worst obese population in EU has been observed in Russia and Malta. In Smolensk, a lot of patients had been evaluated in the Smolensk State Medical Academy. 1733 peoples had been measured and evaluated. For example, 390 healthy subjects without heart attack, stroke, hypertension, HCM, DM and smoking had been compared with Aging (Figure 1).
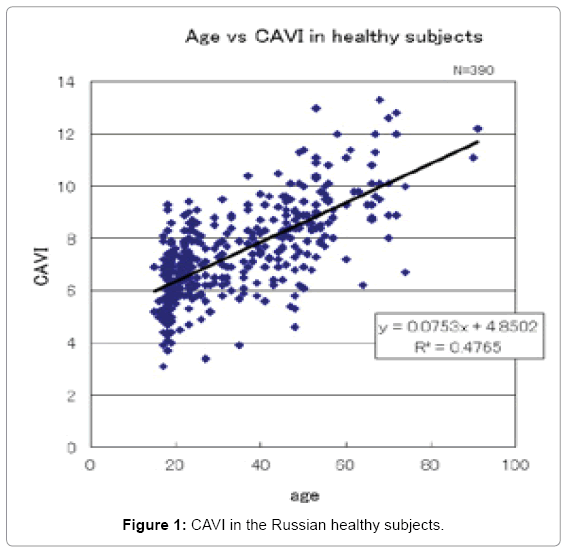
Figure 1: CAVI in the Russian healthy subjects.
Everybody knows that DM has been the worst risk factor in metabolic disorder. Of course, the Russian data had supported the existence of this phenomenon (Figure 2).
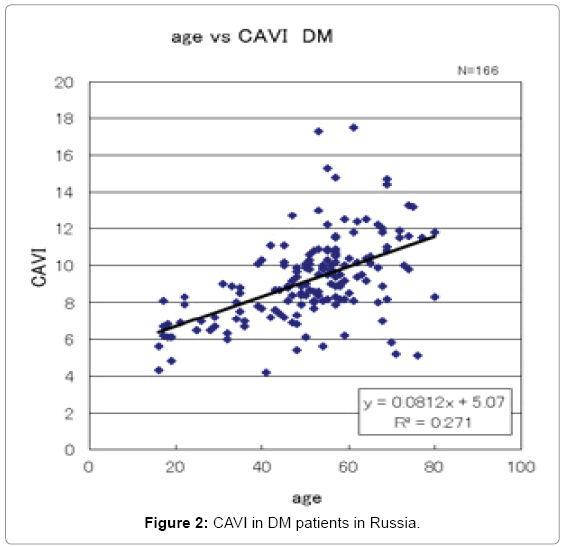
Figure 2: CAVI in DM patients in Russia.
Baroreflex system is one of the most important regulatory systems to maintain the homeostasis of the circulation. When blood pressure (BP) was increased, baroreceptor sensed this increase. Neural information concerning the BP change was evaluated in the central control system. Heart rate (HR) was reduced and resistance vessels were dilated by the autonomic control system. BP was returned to the normal range by the reduction of the pump output and vascular resistance. Sensitivity of the baroreflex system was evaluated by the various methodologies. Quantitative evaluation by the slope of the regression line between BP change and HR change was one of the typical methods to evaluate the baroreflex sensitivity of the heart. However, we could not evaluate the baroreflex sensitivity of the vascular system by this method.
Autonomic nervous system control of the each internal organ was different. So, we must evaluate the sensitivity of the baroreflex system of an artery. However, it is very difficult to evaluate the tonus of the artery in the human body during awaking condition. Recently, brachial ankle pulse wave velocity (baPWV) and cardio ankle vascular index (CAVI) were invented and commercialized. These methodologies measured the pulse wave velocity of the human body and calculate the tonus of the artery. So, if we use these methodologies to measure the tonus of the artery, we can measure the characteristics of the baroreflex system of an artery.
New diagnosis tool to evaluate the baroreflex sensitivity of an artery was invented.
In order to evaluate the baroreflex sensitivity of an artery, we used the information of the pulse wave velocity of the human body. Time series data of the ECG, pulse wave of the radial artery, and fingertip pulse wave were recorded in the data recorder and analyzed in the personal computer system. Pulse wave velocity was calculated from the time lag between the R wave and pulse wave. Changes of the pulse wave transmission time were plotted against the changes of the blood pressure. Slopes of the regression line showed the baroreflex sensitivity of the peripheral resistance artery.
Quantitative evaluation of the baroreflex sensitivity may be useful when we consider the ideal treatment of the patients with hypertension [12,13].
New methodology of pulse diagnosis had enabled us the noninvasive measure of the Cardiology. Carotid-femoral pulse wave velocity (PWV), the brachio-ankle PWV, and cardio-ankle vascular index (CAVI) based on the thesis of stiffness parameter beta had been developed and used in the hospitals in all over the world. By the use of baPWV and CAVI, measurement time had been short and individual physician's alteration had been so small. And price is relatively low, so it may be used in developing countries (Table 1).
| baPWV | CAVI | Stiffness p | |
|---|---|---|---|
| Objective Segment | Mainly lower limb arteries | Heart to Ankle | Local point |
| Measurement time | 3-4 min | 4-5 min | 20-30 min |
| Blood-pressure affection | Very weak | Very weak | none |
| Individual Comparison | Impracticable | Practicable | Practicable |
| Price | medium | medium | Expensive |
Table 1: Comparison of the various methods to measure the atherosclerosis.
Further international cooperative studies are undergoing now. So various scientific reports are easily found in pubmed. Medical device maker is now gathering these international papers for the presentation to the every doctors in the world for the achievements of better medical care. If the evaluation by this methodology in not so good, all doctors have a chance to use another devices. So, it is not necessary to use this method when the scientific papers showed another device had been good. Every doctor in all over the world must check recent progress in medical device in the scientific fields.
For example, Schillaci et al. had reported the usefulness of CAVI compared with cf PWV in LV mass detection [14]. We need the further examination in future, but comparison of the various methodologies is always important.
Otsuka K et al. [15] reported the changes in CAVI after management of atherosclerotic risk factors and the impact of these changes on future CVD outcomes. CAVI improved in 50% patients after 6 months, but remained high in 50% patients. CVD outcomes were worse in patients with persistently impaired CAVI than in those with improved CAVI (P<0.001). His study was the first to demonstrate that persistent impairment of arterial stiffness was an independent risk factor of future CVD events.
Long time follow up is the most important issue. We must continue this kind of studies. Of course, the obesity in one of the most important factors in metabolic syndrome when we consider the healthy population in every country. Sato asahara et al. reported the incidence of cardiovascular events in obese patients. And their study demonstrates for the first time that CAVI is an effective predictor of CVD events in obese patients [16].
More and more studies [17-21] are carried out now in all over the world. There may be a possibility that another new diagnosis method will be invented. We must continue our study for the more good treatment of the patients
Part of the results of this paper is based on “Agreement of Academic Exchange between Tohoku University and Smolensk State Medical Academy”, “Japan-Russia joint research on arteriosclerosis and aging using CAVI” supported by Fukuda Kinen Iryo-Technology Promotion Foundation, “Bio-nanotechnology-based medical engineering” (Tohoku University 21st century COE) and “Nano medical engineering hubs in the growing global source of the new century”.