Pediatrics & Therapeutics
Open Access
ISSN: 2161-0665
ISSN: 2161-0665
Review Article - (2014) Volume 4, Issue 1
Bladder Bowel dysfunction (BBD) represents a broad term used to describe a multitude of conditions associated with incontinence or Urinary Tract Infections (UTI) that commonly is seen in primary Family and/or Pediatrics care. The BBD spectrum includes lower urinary tract conditions such as overactive bladder and urge incontinence, voiding postponement, underactive bladder, and voiding dysfunction, and, importantly, also includes bowel issues, as constipation and encopresis. BBD is often not recognised by family or child or even the referring professional, but it is the secondary symptoms of wetting or UTI, that prompts the child to be evaluated by a consultant. The goal of this review is to provide a practical guideline for diagnosis and management of BBD in children, common problem in daily pediatric practice. Most importantly, considering that most of these issues are functional, is that the majority of these children are best evaluated and treatment instituted by the primary provider, with referral to a specialist, only in exceptional cases.
Keywords: Bladder bowel dysfunction, Lower urinary tract symptoms, Dysfunctional elimination syndrome, Urinary tract infection
Bladder Bowel dysfunction (BBD) is a broad term used to describe children who present a constellation of Lower Urinary Tract Symptoms (LUTS) associated with constipation and/or encopresis. The functional interaction between bowel and bladder is well described in medical literature [1-9]. In this clinical condition, bladder symptoms such as urgency, frequency and incontinence are caused by problems in emptying and/or storage [1]. Overall, the rectum loaded with stools compresses the bladder and decreases the bladder capacity, ultimately leading to urgency and frequency. Furthermore, the increased fecal mass located in the rectum may cause chronic pelvic spasms which will likely result in incomplete bladder emptying and significant post void residual volumes [2]. Additionally, children who voluntary hold urine for longer periods will gradually present decreased sensation/ urge to evacuate establishing the BBD cycle pattern [6,10]. BBD is thus a more representative term for a spectrum of disorders, commonly referred to previously, as dysfunctional voiding and/or Dysfunctional Elimination Syndrome (DES). Often unrecognised, as a diverse spectrum by family, child, or even the referring professional, it is the bothersome secondary symptoms of wetting, constipation or Urinary Tract Infection (UTI), that prompts further evaluation or referral to a specialist. These patients represent a common component of virtually every primary care practice, but a substantial number of these children also are referred to pediatric urologists and nephrologists, and if bowel symptoms predominate, referral may be to gastroenterologists or pediatric surgeons. In fact, BBD represents approximately 40% of patients presenting to the pediatric urologist [2]. It is a field replete of semantic confusion. As a result, the literature in this area is often divergent and, there is a lack of randomized, controlled prospective trials that could provide the baseline for standardised diagnosis and treatment of BBD.
In this review, we use the term BBD to describe the multitude of conditions leading to incontinence or urinary tract infections, commonly seen in primary care practice. The goal of this review is to provide a practical guideline for diagnosis and management of BBD in children, targeting mostly primary care practitioners, who very commonly have to deal with these patients in daily practice. More importantly, most of these children likely can be evaluated and treatment instituted without early referral to a specialist. Clearly, however since BBD represent a spectrum, the most severe and recalcitrant cases may require more specialized involvement. The following synopsis is not intended to be a systematic literature review, but rather a discussion of relevant research studies in the field, and discussion based on our own experience and recommendations in these children.
The genitourinary tract and gastrointestinal tracts share the same embryological origins, pelvic location, aspects of innervation and passage through the levator ani. Commonly, stool retention with or without fecal incontinence coexists with dysfunctional voiding as a result of non relaxation of the pelvic muscle floor [2]. In this context, urinary incontinence and recurrent UTIs are often present [2-5,11]. The close anatomical proximity of the bladder and urethra to the rectum makes it likely that abnormalities within one system will affect the other [4]. For normal voiding and defecation the pelvic floor muscles and striated sphincters are needed to relax appropriately. The coexistence of bladder and bowel disorders might be explained by few proposed theories in the medical literature [4,5,10,11]. Chase et al. [10] and Burgers et al. [6] have proposed that in the presence of constipation, rectal distension directly pushes the posterior bladder wall anteriorly causing bladder overactivity. This increased pressure can also result in mechanical compression of the bladder, what potentially leads to trigonal irritation or even bladder neck and obstruction of the urethra [9,10]. The effect of rectal distension on bladder function has been evaluated with urodynamic studies [6]. Such studies suggest that rectal distension significantly affects bladder capacity and contractility, in some but not all, children with Lower Urinary Tract Symptoms (LUTS). O’Regan and Yazbeck [7] theorized that when the external anal sphincter contracts for prolonged periods in the context of large fecal load, this long term contraction results in abnormal pelvic floor contraction and ultimately non-relaxation of the urethral sphincter-the so called detrusor-sphincter dyssynergia [4]. Potential consequences of this dyscoordination are bladder overactivity, urinary incontinence, recurrent UTIs or Vesicoureteral Reflux (VUR) [4,7,8]. Treatment of constipation in children with BBD frequently results in results in improvement of urinary incontinence and less urinary tract infections [4,9,12].
In an effort to facilitate clinical diagnosis and treatment, we describe below some of the most commonly recognized conditions defined as part of BBD spectrum, proposed by the International Children’s Continence Society (ICCS) [3,9]. We have arbitrarily divided the clinical conditions into 2 subgroups: I) Those common conditions that may be diagnosed, initially treated and even potentially followed by the primary care practitioner (therefore referral to the subspecialist may be indicated only if failure to initial treatment occurs); and II) Conditions that may require earlier consultation and management with the specialist.
Conditions potentially managed by the primary care practitioner
Overactive Bladder and urge incontinence (OAB): Previously known as “bladder instability”- the most common form of BBD, with reported incidence of approximately 60% among children presenting incontinence [13]-is best characterized by frequent episodes of an urgent need to void, countered by contraction of the pelvic floor muscles and holding maneuvers such as squatting with the heel pressed into the perineum, and standing on tiptoes, crossing of the legs – the Vincent Curtsy’s sign (Figure 1A). As mentioned in the ICCS standardisation of LUTS terminology document (J Urol 2006): “The hallmark of OAB is urgency and, thus, children with this symptom can be said to have an OAB.” Patients with OAB usually have incontinence secondary to detrusor overactivity, and can be inferred by the symptoms above. Oftentimes these symptoms occur only during the daytime, although the situation can be more challenging when there is nocturnal enuresis, and/or bowel issues. The goal of therapy is to assure that any constipation is dealt with first, while the children are instructed in a timed voiding program. In recalcitrant cases, after bowel status has been optimized, anticholinergics may be considered.

Figure 1A: Holding maneuvers in girls: Vincent Curtsy’s sign.
Voiding postponement: Many children between 3-5 years old tend to delay urination because of intense concentration on playing or watching television or using electronic toys. Therefore daytime incontinence and holding maneuvers are habitually noticed by parents (Figure 1B). As a result they occasionally have damp or soaked clothing. If the voiding pattern is otherwise normal, this pattern of voiding dysfunction usually subsides with increase effort toward scheduled voiding. One study of an initial trial of timed voiding reported that 45% of patients had a significant improvement in the frequency of wetting [14]. These children usually present with low voiding frequency and urgency due to a full bladder. They commonly will have constipation as an associated problem, due to the fact that the mechanism to delay defecation is similar [2,15]. This entity has been observed more frequently, in children who have experienced psychological and behavioural disturbances [13]. Again the goal of treatment is to have an empty bladder and rectum. Hence constipation is treated while a timed voiding regimen is instituted.

Figure 1B: Holding maneuvers in girls: Squatting.
Extraordinary daytime urinary frequency: Unlike virtually all other categories of voiding dysfunction where females predominate over males by a 5:1 ratio, children with extreme daytime frequency are predominantly male [16,17]. Children presenting daytime frequency typically present very small voided volumes, often less than 50% of the Expected Bladder Capacity (EBC)* and micturition occurs at least once every hour [3]. Importantly, this diagnosis is heralded by lack of associated incontinence and nocturnal enuresis. The best treatment, therefore, is reassurance. Again, these youngsters are dry with no urge to urinate or void after bedtime. Invariably this occurs in young boys and is self-limited. (*EBC in ml: children >1 year of age=age in years +2×30; <1 year=7×weight in Kg) [13,16].
Dysfunctional voiding: The appropriate use for the term Dysfunctional Voiding (DV) according to the ICCS standardisation document (J Urol 2006) is applied to “children who contracts the urethral sphincter during voiding.” The idea is to keep it simple: “Dysfunctional voiding means purely dysfunction during voiding”. Thus, applying the term to other conditions may lead to confusion. DV is commonly associated with constipation and/or encopresis. Confirmation of true DV can only be obtained with repeat uroflow curves showing staccato pattern or during invasive urodynamics test [3]. However, given the majority of children who present LUTS will likely respond to conservative therapy with constipation management and bladder retraining [2,4,10,12], we strongly believe that these patients may be initially treated by the primary care doctor, as discussed below in the section “Diagnostic approach of BBD”. Nevertheless, failure to treatment with absence of improvement or worsening symptoms of incontinence, and recurrent episodes of UTI despite BBD treatment might prompt referral for urological assessment. In the most extreme situations, the contracted sphincter provides a “physiological obstruction”, with the potential for significant morbidity at the bladder and kidney levels. Such children are labeled as “Hinman- Allen” syndrome which is discussed later in this manuscript. Because of the dyscoordination and pelvic floor contraction causing pseudo-obstruction, therapy is centered on bowel and bladder emptying.
Conditions that may require specialist evaluation
Underactive bladder: The new term underactive bladder, previously known as “lazy bladder, is used to identify children who void very infrequently, typically 2-4 times daily. Not rarely they need to strain, increasing intra-abdominal pressure, in attempt to start or complete voiding [3]. They likely represent a more extreme variant of the voiding postponement group addressed earlier. These children often do not void on awakening, either at public restrooms or at school (commonly the first void in the day occurs at home after school) and typically present symptomatic UTI or asymptomatic bacteriuria, dribbling, enuresis and/or constipation/encopresis. If available, these children classically present an interrupted pattern on uroflow with a large post void residual. Since they represent spectrum of voiding postponement, urotherapy is the first step in treatment, with an intensive bowel program. Occasionally more invasive modalities need to be instituted in order to assure emptying.
Hinman-allen syndrome: Hinman Syndrome (HS), or Hinman- Allen syndrome is the most severe form of dysfunctional voiding. It is an important example of “functional” obstruction of the urinary tract which consists of a spectrum of presentations. Thus, although the problem is physiological, not anatomical, the secondary obstructive sequelae may resemble those associated with anatomical diagnosis that must be considered, such as: posterior urethral valves or urethral stricture. Likewise, an occult neurogenic issue must be excluded by a thorough history and physical exam.
It is characterized by functional bladder outlet obstruction in the absence of neurologic deficits. The prevalence is not known. The syndrome typically occurs at some point after toilet training in early to late childhood after a period of normality but even infant and adult cases have been observed [18]. Patients may present with a myriad of symptoms: enuresis, urgent voiding with incontinence, infrequent voiding, intermittency, straining, urinary tract infections and diffuse abdominal pain. HS is probably caused by acquired behavioural and psychological disorders manifested by bladder dysfunction mimicking neurologic disease [19,20]. The dysfunction is frequently associated with abnormal family dynamics in 50% of cases. Individuals under psychosocial pressure (divorce, sexual abuse) try to inhibit enuresis by voluntarily contracting the external sphincter. These voluntary contractions lead to an obstruction of the urinary tract, characterized by an intermittent stream, increased residual urine and increased intravesical pressure. The resultant destruction of the urinary tract simulates true neurogenic bladder.
HS can be differentiated from neurogenic bladder by five criteria: a) intact perineal sensation and anal tone, b) normal anatomy and function of the lower extremities, c) absence of skin lesions overlying the sacrum, d) normal lumbosacral spine at plain radiography, and e) normal spinal cord on imaging (magnetic resonance imaging or ultrasound if younger).
In summary HS diagnosis is based on the presence of the clinical and radiographic manifestations of neurogenic bladder in the absence of an underlying neurogenic abnormality or an obstructive lesion.
HS can result in a trabeculated bladder, ureterovesical obstruction, dilation of the upper tracts, and vesicoureteral reflux. Even chronic kidney disease and end stage renal disease can occur in the most extreme cases. Given the potential burdens for the urinary tract and renal function when HS is suspected prompt referral to a pediatric urologist is highly recommended. Briefly, treatment for HS focuses on helping the child void and defecates normally through alleviating psychosocial pressures which are likely to be causing the problem with voiding through suggestion therapy including hypnosis, bladder retraining and timed voiding. More invasive and even surgical interventions indicated in extreme cases where behavioural and medical modalities have failed and the bladder and kidneys are affected.
For the scope of this review we include common clinical conditions in which LUTS are present, frequently seen in the primary care practice, thus important for the differential diagnosis of BBD:
Vaginal reflux
This event is explained by the occurrence of vaginal entrapment of urine during micturition. Vaginal reflux of urine from voiding in a knees-closed position can cause dampness when the child assumes an upright posture after voiding or post void dribbling. These girls are diagnosed with vaginal reflux if no other underlying mechanism is identified [3]. Labial adhesions, a common finding in young girls, are rarely severe enough to be the instigating issue for vaginal reflux. They are thus more commonly a benign associate, rather than causative, finding. As a result, caution should be exercised when suggesting treatment of labial adhesions for cure of vaginal voiding. Treatment is centered on positioning and spreading the legs properly when these girls are toileting, so that reflux is eliminated. This can be aided by assuring that panties are pulled down below the knees. Even sitting on the toilet backwards or in short children’s, having them relax their legs on a stool, is helpful.
Giggle incontinence
Occurrence of involuntary complete bladder evacuation induced by laughter and typically appears in children aged 5-7 years. Giggle incontinence can persist throughout the school years but usually improves or disappears with age. The voiding pattern is otherwise normal. Episodes of incontinence may occur with giggling in some children; in others, they are induced by only vigorous laughter. The etiology is unknown. Giggle incontinence is not a form of stress incontinence, nor is it due to weakness of the sphincter. The authors of one study found a high incidence of daytime voiding symptoms in patients in whom they diagnosed giggle incontinence [21]. The authors concluded that laughter induced unstable detrusor contractions in children susceptible to detrusor instability. When bothersome, methylphenidate (Ritalin) has been shown to be useful as a therapeutic option [22].
Female epispadias and male proximal epispadias
Epispadias, consisting of the defect of the dorsal wall of the urethra, occurs more commonly in males than in females, with a prevalence of 1 case in 10,000-50,000 people [23]. The male-to-female ratio is 2.3:1.
Isolated female epispadias without bladder exstrophy is an extremely rare congenital anomaly occurring in 1 in 480.000 females [24,25]. The usual complaint is abnormality of the external genitalia which may or may not be associated with urinary incontinence or, in older women, sexual dysfunction. The diagnosis can only be made after a detailed local examination by separating the labia. In most instances the vagina and internal genitalia are found to be normal. The anomaly can be corrected by surgical reconstruction of bladder neck, urethra and external genitalia.
In males the defect resultant of failure of the urethral plate to tubularize on the dorsum ranges from a glandular to a penopubic location. In addition, male patients demonstrate a dorsal chordee whereas female patients exhibit a bifid clitoris [26]. Proximal epispadias does not involve the body of the bladder or the hindgut but does affect the urethra and can affect the bladder neck. As a consequence, it presents with a spectrum of severity that can affect urinary continence if the epispadias anomaly is proximal enough to affect the urinary sphincter mechanism.
The burden of lower urinary tract dysfunction
Although BBD should be considered to be associated with a psychosocial burden, for children and families, if left untreated, secondary comorbidities may occur. LUTS cause distress with the potential to adversely impact renal and bladder function. For instance, in the presence of lower urinary tract symptoms, particularly those with documented associated urological abnormalities, such as vesicoureteral Reflux (VUR), children may have an increased risk for urinary tract infection, renal scarring, and consequent long term development of renal damage, compared to those without BBD [2]. Delayed resolution of VUR has been documented in children with BBD [27,28]. It has been shown that the child with OAB symptoms is much more likely to have continued problems with OAB in adulthood. Pelvic floor contractions and holding maneuvers associated with OAB and dysfunctional voiding may result in inappropriate postponement of defecation.
It has been shown that constipation associated with Lower Urinary Tract Dysfunction (LUTD) constitutes the so called Dysfunctional Elimination Syndrome (DES) or now referred to as BBD (J Urol 2010) [1,28]. It is not infrequent that parents of a child with wetting issues may be unaware that their child also has coincidental bowel dysfunction [29]. In the presence of constipation, both LUTD and the gastrointestinal tract must be addressed and treated properly, or voiding symptoms are unlikely to improve. Dohil et al. [30] have shown that in a group of children presenting with increased post-void residual urine and constipation, 66% had improvement in bladder emptying after treatment of constipation alone [31]. In another study treatment of constipation resulted in 89% resolution of daytime wetting, 63% resolution of nocturnal enuresis and prevention of urinary tract infection [29].
On the other hand, patients with severe voiding postponement, underactive bladder, presenting with infrequent voiding, often have an overdistended bladder that may decompensate over time, resulting in decreased or absent detrusor contractions. At this point, they may require abdominal pressure with Valsalva or Crede maneuvers to be able to void (Figure 2). Ultimately, if untreated, Clean Intermittent Catheterizations (CIC) may be required for the management of this condition, as bladder function deteriorates. A different condition of note occurs in patients who void at high pressures secondary to overactive or dyssynergic pelvic floor contractions, resulting in increased outlet resistance. Initially, hypertrophy of detrusor occurs. Later, this can also lead to bladder deterioration, ultimately requiring clean intermittent catheterizations. Children with LUTD of this nature are diagnosed with the severest form of non-neurogenic bladder dysfunction called Hinman syndrome, previously discussed in this review [32].

Figure 2: Crede maneuver: patients with underactive bladder may progress to decreased or absent detrusor contractions. At this point they may need increased abdominal pressure to be able to void.
The pediatric urinary incontinence ABC’s
In the context of urinary incontinence in children it is important to have in mind possible causes as Anatomic, Behavioral, CNS/ neurological, Developmental, Endocrine, renal, Functional, Genetic, Habitual or Infectious/irritation (Table 6). For the purposes of this review, we will limit the discussion to the most common and clinically relevant anatomic causes that might have prompt specialist assessment. Much of the behavioural issues were discussed above and may be initially managed by the primary care physician.
The initial diagnostic approach should explore both voiding and bowel components of BBD. In regards to the voiding dysfunction, LUTD of all types may be functionally classified to either failure to store or failure to empty [13,33]. It is important to have in mind which phase most likely the lower urinary tract dysfunction occurs: storage or empty phase, in order to identify which factor(s) has (have) resulted in BBD. Concomitantly, bowel issues, especially constipation must be addressed. It is important to suspect for bowel dysfunction in children with LUTS and in the opposite scenario, to look for LUTS in children with bowel dysfunction. The definition of constipation varied for many years among physicians, patients and parents. For instance, normal stool frequency can vary from 3 stools per week to 3 stools per day, from three years old on [9]. The ICCS recommends the use of the Rome III criteria for diagnosing functional defecation disorders in children (Table 3). Because the Rome III criteria were established by pediatric gastroenterologists specialized in functional gastrointestinal disorders, in theory they might not be entirely applicable for children with primarily urinary tract symptomatology. In the presence of constipation the Bristol Stool Form Scale (BSFS) represents a practical and widespread tool extremely helpful for diagnosis and evaluation of therapy response (Figure 3).

Figure 3: The Bristol Stool Form Scale: A helpful tool on diagnosis and management of constipation.
History: A good clinical history is the key for BBD diagnosis. Regarding LUTS, important points should include history of recurrent febrile UTIs (details of these should be pursued in depth, as presence of documented fever, urine culture, how urine specimen was obtained), any known urinary tract malformations. A voiding history, with symptoms as frequency, urgency, dysuria, or incontinence and characterization of these, if present. Urgency and frequency often result in daytime accidents and are frequently associated with nocturnal enuresis [9]. Dysuria is often associated with UTI but in the absence of infection it may be caused by pelvic fecal mass compressing the urethra against the pubic bone. It is crucial to not label dysuria and other urinary symptoms as “UTI”, if no appropriate laboratory confirmation has been obtained. Similarly boys may complain of penile or scrotal pain as result of referred pain from a fecal mass. Abdominal pain and cramps, often severe, may be associated with urinary postponement and/or severe constipation. Infrequent voiding may be a manifestation of the underactive bladder with incomplete emptying and elevated post void residuals related to constipation. Patients with other symptoms such as enuresis, voiding postponement, extraordinary daytime frequency or terminal hematuria should be screened for constipation given that treatment for these conditions is often unsuccessful in the presence of underlying constipation [31]. It is important to identify the presence of other symptoms, such as nausea, vomiting, weight loss or failure to thrive, inappetence, muscle weakness/atrophy and psychological or behavioral problems. Bowel habits should be detailed in the history - frequency of bowel movements, stools consistency, shape, caliber and size, presence of fecal incontinence, straining, etc. It is necessary asking if the child experiences pain during defecation, the presence of episodes and timing of fecal incontinence, and stool withholding behavior. Importantly, talking to the child often reveals information that parents cannot provide. Questions about retentive posturing behavior in younger children are frequently denied because they are overlooked or misinterpreted for attempts to strain for defecation [9]. The BSFS (Figure 3) can help patients and physicians to classify their stool form using different images and descriptions in everyday language. The original BSFS was adapted for the use in children. The final scale consists of 7 stool form descriptors accompanied by drawings. The accuracy of the defecation history in children as provided by the child and/or parents can be improved with use of a bowel diary. Typical symptoms of constipation in children are listed on Table 1. The primary care practitioner must be able to clarify the impact of BBD in the child’s and family/caregivers quality of life. Knowledge of the time of the first bowel movement is essential to discriminate functional constipation from Hirschsprung’s disease. Dietary history and the history of previous treatment strategies for constipation should be investigated. Finally, it is important to ask for life events, such as death in the family, birth of a sibling, school problems and sexual abuse which might contribute to the development of retentive behavior.
| Functional constipation | ≥ 2 of the following in a child ≥ 4 years old not |
| fitting IBS criteria: | |
| ≤ 2 defecations per week | |
| ≥ 1 episode of fecal incontinence per week | |
| History of painful or hard bowel movements | |
| Presence of a large fecal mass in the rectum | |
| History of large diameter stools that obstruct the toilet | |
| History of retentive posturing or excessive volitional stool retention | |
| FNRFI (Nonretentive fecal incontinence) | Allof the following in a child ≥ 4 years: |
| Defecation into places inappropriate to the social context at least once per month | |
| No evidence of an inflammatory, anatomic, metabolic, or neoplastic process | |
| No evidence of fecal retention | |
Table 1: The Rome III pediatric criteria for functional constipation and functional nonretentive fecal incontinence (FNRFI).
Physical examination: Physical examination must include careful inspection of the genitalia to rule out anatomical causes of lower urinary tract dysfunction. Rashes in the perineum or genital areas may indicate fungal infections that result from chronic wetness. In girls, the genitalia should be examined to evaluate for sexual abuse, as one study reported that 6% of patients evaluated for voiding dysfunction had a history of sexual abuse (89% of that group was female) [20]. Occasionally an ectopic ureter or female epispadias will be recognized early by a detailed exam, rather than delaying the proper diagnosis. The rectal examination may help rule out most organic causes of constipation (i.e. Hirschprung’s disease, anorectal malformations, etc). Neurologic examination and careful inspection of the spine and limbs should be performed to rule out an abnormality of the lumbosacral area that suggests occult spinal dysraphism, which includes a sacral dimple or tuft of hair, dermal vascular malformations, a small lipomeningocele, absence of the gluteal cleft with flattened buttocks, or hyperextension of the toes (possible lesion of S1-S2). The neurologic examination should include assessment of motor strength, deep tendon reflexes, perineal sensation, gait, and coordination. In the presence of any neurologic deficits, significant cutaneous lesions in the lumbosacral region, or bony abnormalities of the spine in children with BBD, further radiological evaluation and neurological consultation should be requested.
Voiding and bowel diary: History and physical examination must be supplemented with bladder and bowel diary (Table 4). The diary should include all voids over a period of 7-14 days, with documentation of the volumes, the presence or absence of incontinence, fluid intake volume and timing of intake, frequency and characteristics of bowel movements, as well as presence of encopresis. Scientifically validated diaries recommend 7-14 days of recording for reliability of information [34-36]. Voiding symptom scores have been proposed and validated by Farhat et al. [37] (Table 2). These scores serve as a useful adjunct to history and noninvasive studies in the diagnosis of BBD. In addition to helping in the evaluation of patients, they are valuable at the time of diagnosis as a baseline for monitoring treatment efficacy, as they provide qualitative and quantitative assessment of symptoms. Scoring systems should include questions related to the storage and emptying phase of micturition, and also include questions related to bowel habits, given the close association between constipation and lower urinary tract dysfunction. Despite no validation, shorter term diaries of 3-5 days have been useful in our practice.
| During the last month | Almost never | < 50% of the time | ± 50% of the time | Almost every time |
|---|---|---|---|---|
| 1. I have had wet my underwear during the day | 0 | 1 | 2 | 3 |
| 2. My underwear is soaked when I wet myself | 0 | 1 | 2 | 3 |
| 3. I don’t have a bowel movement every day | 0 | 1 | 2 | 3 |
| 4. I have to push for my bowel movements to come out | 0 | 1 | 2 | 3 |
| 5. I only go to the bathroom to pee 1 or 2 x/day | 0 | 1 | 2 | 3 |
| 6. I can hold my pee crossing my legs, squatting, or doing the pee dance | 0 | 1 | 2 | 3 |
| 7. When I have to pee I can’t wait | 0 | 1 | 2 | 3 |
| 8. I have to push to pee | 0 | 1 | 2 | 3 |
| 9. When I pee it hurts | 0 | 1 | 2 | 3 |
| 10. Parents to answer: Have your child experienced any stressful situation as the examples below* | No (0) | Yes (3) |
*School difficulties, sexual or physical abuse, family problems(divorce/death), new baby at home, new school, new home
Table 2: An example of validated voiding score system: The Dysfunctional Voiding Scoring System (Adapted from Farhat et al. [37]).
| ITEMS TO BE CHECKED | ACTIONS TO BE TAKEN |
|---|---|
| Background data | Actions if answer is yes |
| Age <6 years? | Only general advice given, no alarm ordesmopressin therapy indicated |
| Is there enuresis every night? | Prognostically unfavorable. Consider sending patient to enuresis specialist |
| Is the child not bothered by the enuresis? | Risk for therapy-resistance. Consider postponing treatment until child is motivated |
| Complicating factors, comorbidity | Actions if present |
| Daytime incontinence (now or after 3,5 years of age), urgency, holding maneuvers, suspected voiding <4 or >7 times per day? UTIs after 3,5 years of age | Suspect non monosymptomatic enuresis. Make the family complete a frequency volume chart before proceeding. |
| Encopresis, hard stools, infrequent bowel movements? | Suspect, and treat for, constipation |
| Significant problems with peer relations and behavior? | Risk for therapy-resistance and/or psychiatric comorbidity. Consider parallel psychological evaluation. |
| Warning signs | Actions if present |
| Straining, weak stream, continuous incontinence, micturition in >1 phase? | Suspect neurogenic bladder or anatomic abnormalities. Send to secondary center. |
| Glucosuria? | Consider diabetes. Send to pediatric clinic without delay |
| Proteinuria (++ or more on urine test) | Consider kidney disease. Consult pediatrician without delay |
| Leucocyturia or nitrite test positive? | Take urine culture. Consider antibiotic treatment if culture is positive |
| Excessive thirst, need for night-time drinking? | Consider polydipsia or kidney disease. Measure fluid intake |
| Nausea, weight loss, fatigue? | Consider kidney disease. Consult pediatrician |
Table 3: Minimal primary evaluation protocol: Recommended minimal primary evaluation of children with voiding and/or bowel symptoms (adapted from ICCS). Prerequisites: voiding history and a urine sample tested for glucose, protein, leukocytes and nitrite.
| Name = ……………………………………………………………………… | |||||||
|---|---|---|---|---|---|---|---|
| Age1 ………….. years | Weight! …………………... kg | ||||||
| Day 1 | Day 2 | ||||||
| Date → | |||||||
| Every time you drink or pie the drink or pee volume (how many milliliters) is filed in here → In the column marked with # we want you to Mark these things: An “L” if the under- pants become wet with urine. A “W” if more than the underpants become wet with urine. An "U” if you feel a Sudden and intense desire to pee. |
Time | Urine volume | Fluid intake | # | Urine volume | Fluid intake | # |
| 6:00 AM | |||||||
| 7 | |||||||
| 8 | |||||||
| 9 | |||||||
| 10 | |||||||
| 11 | |||||||
| 12 | |||||||
| 1:00 PM | |||||||
| 2 | |||||||
| 3 | |||||||
| 4 | |||||||
| 5 | |||||||
| 6 | |||||||
| 7 | |||||||
| 8 | |||||||
| 9 | |||||||
| 10 | |||||||
| 11 | |||||||
| night | |||||||
| Marx here if the following night is wet or dry → | Dry night □ Wet night □ |
Dry night □ Wet night □ |
|||||
Table 4: Example of seven day frequency-volume chart.
Complementary exams: The first exam that should be done in the context of lower urinary tract dysfunction is the urinalysis and if indicated, quantitative urine culture should be performed for evaluate for UTI. On urinalysis, the specific gravity (concentration) of the urine is noted as well as any evidence of underlying voiding problems based on the presence of hematuria, proteinuria, or glucosuria. A simple urinalysis can assist in discriminating dysuria from a UTI or, if no pyuria or bacteriuria, BBD (i.e. OAB, dysfunctional voiding, etc) may be more likely. The documentation of febrile UTIs with appropriate collected urinalysis and urine culture is of major relevance and must be obtained whenever the child presents fever and lower urinary tract symptoms. However, It is important to avoid collecting random urine specimens when the child is asymptomatic (looking for asymptomatic bacteriuria), given that meaningless positive results in this context may lead to erroneously overdiagnosing UTI, with consequent excessive and unnecessary antibiotic use, onerous and even invasive, complementary investigations (i.e. VCUG, nuclear renal scans).
Renal and Bladder Ultrasounds (RBUS) are not a routine in most of the simpler diagnoses discussed previously. In reality, they are most often ordered to alleviate parental anxiety, not for clinical indication. Clearly, in the more extreme cases, there might be clinical indications for ordering RBUS.
The measurement of Postvoid Residual (PVR) using a bladder scanner or transabdominal Ultrasound (US), can bring invaluable information in the context of OAB suspicion. Although minimal detrusor overactivity or dyssynergia cannot be excluded, the patient can be commenced with the standard protocol for OAB with less risks of developing a UTI [38]. In children presenting with warning LUT/ bowel symptoms as straining, weak stream, continuous incontinence or micturition in more than 1 phase, transabdominal US may give invaluable information regarding the status of the upper urinary tract [3]. Moreover, the US can show an impression of the rectum behind the urinary bladder and is considered to be a simple and reliable technique to demonstrate fecal loading in children. With this non-invasive technique, the transverse rectal diameter can be measured. This is used by pediatric surgeons, pediatric urologists and in some countries by pediatricians and allied health professionals and should be used only as an adjunct, when simple less expensive investigation has failed. Patients with lower urinary tract dysfunction and constipation were found to have a significant larger diameter of the rectum than those presenting regular bowel pattern, however, there is insufficient evidence that the transverse diameter can be used alone as predictor of constipation and fecal impaction [6]. Klijn et al. proposed: In both non-constipated and constipated children a diameter above 30 mm correlated with a positive finding of rectal impaction on a digital rectal examination, implying that US can give information regarding rectal impaction as one of the six Rome III criteria [27]. Additionaly, in our experience, the kidneys, ureters, and bladder X-ray (KUB), may be of great help to confirm the presence of fecal loading, convince parents and children of the need for constipation therapy, monitor the success of therapy and rule out gross boney abnormalities.
More sophisticated investigations
Non-invasive studies as uroflowmetry associated with bladder ultrasound may provide valuable information in cases of LUTD. This is not readily available in a primary care office; however it is an important diagnostic tool for the pediatric urologist. In the primary care setting, focus of this review, often just watching and listening while the child voids can be very helpful – the “poor man’s uroflow”. A strong stream compared to an intermittent stream can often be assessed in this manner. If any abnormality is noticed in the stream, these patients should be promptly referred to the specialist (Figure 4). The volume voided in conjunction with a good voiding diary may provide information for the establishment of the functional bladder capacity. This could be very different from the anatomic capacity, secondary to diminished compliance, detrusor overactivity or high post void residuals.

Figure 4: The wet child investigation in the primary care setting.
More invasive studies, such as urodynamics or videourodynamics should not be performed on a routine basis to diagnose BBD, and rarely are even ordered after referral to a pediatric urologist. Although formal urodynamic testing provides the greatest amount of information regarding the components of bladder storage, i.e. capacity, compliance and contractility, it remains an invasive study and should not be construed as the urological equivalent of an electrocardiogram.
VCUG may have an important role in the presence of confirmed recurrent febrile urinary tract infections, mainly in the context of renal parenchymal abnormalities, as scarring, cortical thinning, increased echogenicity, reduced corticomedullary differentiation, poor renal growth and/or dilatation of renal pelvis, calyces and ureters on ultrasound. VCUG is the gold standard test for the diagnosis of Vesicoureteral Reflux (VUR), bladder abnormalities (trabeculation, thickening, ureteroceles) and posterior urethral valves. If VUR is diagnosed, accompanied by recurrent UTIs or any of the ultrasound findings discussed above, prompt referral to the specialist is recommended. However, BBD should be addressed and managed concomitantly and treatment should be initiated by the primary care doctor while the referral is expedited.
Therapy may be directed more appropriately at the cause of the dysfunction. Although primary care practitioners have at their disposal a wide range of treatment modalities for the management of patients with BBD, it is not recommended to initiate any therapy without clearly diagnosing the etiology of the child’s symptoms. In the absence of anatomic or neurologic abnormalities, the functional classification of LUTD (bladder storage vs. emptying phase symptoms) may be applied to indicate the most appropriate therapy for the presenting condition. Other factors that may influence the selection of therapy are: child’s age, duration of symptoms, impact on quality of life, and comorbidities. Impact on quality of life to the child and the impact on the caregivers’ quality of life may be very different and will play an important role in the level of compliance to treatment. Children with evidence of upper tract deterioration evidenced in the US by progressive dilatation of the urinary collecting system and evidence of parenchymal damage (i.e. increased echogenicity, cortical thinning and decreased corticomedullary differentiation) require prompt, aggressive management, while those with no comorbidities can be treated conservatively. Patient or physician preferences have also to be taken into consideration in selecting a specific form of therapy.
Urotherapy is a non standardized term referring to nonsurgical and non pharmacological treatment of lower urinary tract dysfunction [3,39]. Our mantra has been: “A happy bladder is an empty bladder. An even happier bladder is an empty one associated with an empty rectum!” Once anatomical abnormalities are excluded, for patients with inadequate emptying, behavioral therapy is generally considered as the first-line treatment. Usually this is based on positive reinforcement, with no negative consequences. Patients may present with a combination of abnormalities that impact bladder emptying but that are not purely pelvic floor dysfunction. Thus it can also benefit from urotherapy. It comprises:
Education of the child/family
Do not assume child and parents understand LUTD. Many families feel their child is unique and are frustrated and angry, may demand a quick fix. Thus, successful management requires ongoing support, instruction, and education, and most important, patience. Children should be taught to understand that normal urination is the result of relaxing the sphincters and permitting the bladder muscle to expel the urine, not a matter of forced voiding using the abdominal muscles. Understanding of bladder structure and function, and etiology of the child’s BBD, lead to better compliance to treatment and more promising response to therapy. The appropriate posture and position for voiding and stooling might be clarified with parents and patients. Children should have a footstool or other solid surface placed in front of the commode so that their feet are on a solid surface. The child should remove his or her underpants or lower them to the ankles to permit relaxed separation of the thighs. During voiding, the child should be comfortable and relaxed and not rushed to void (e.g., during a television commercial). Boys should be instructed to free their penis before voiding. The zipper or buttons should be completely opened. If the underwear constricts the penis, this should be corrected. Boys should be relaxed and take sufficient time to completely empty the bladder.
Routine hydration
The goal is to achieve the recommended daily Total Fluid Intake (TFI) for child’s age or weight. Taking 1 cup of fluids after all voids is a good way to keep adequate hydration and facilitates the timed voiding. Whether it works or not, another of our clinical mantras is: “Dilution is is the solution to pollution!” Again this is based on the praise that more fluids may dilute any bladder bacteria, but more frequent urination and emptying will occur when hydration is optimized.
Regular optimal voiding regimens
A timed voiding schedule should be used when the child is awake, even in those with urinary frequency. Children should be encouraged to void before a sense of urgency is present in order to develop a regular voiding pattern. Time voiding is instituted with bladder evacuation every 2-3 hours “by the clock” when the child is awake. This is an essential component of bladder retraining. Writing letters to a school nurse, teacher, or principal to carry out this program is necessary and of value. In a survey of school nurses, 47% of respondents reported being involved in setting voiding schedules for children, and the majority allowed free access with a physician’s note [40]. Double or triple void is useful practice in trying to improve bladder emptiness. Voiding and bowel diaries should be used to determine treatment response. The latter is important even in the child with no history of constipation. The document standardized by ICCS for lower urinary tract function terminology states that, initial success to treatment is considered full response if 100% decrease or less than 1 symptom occurrence monthly; response is defined as a 90% or greater decrease, partial response 50% to 89% decrease, and non response is defined as a 0% to 49% decrease. In regards to long term success, relapse is defined as more than 1 symptom recurrence monthly; continued success is defined as no relapse in 6 months after the interruption of treatment and complete success is defined as no relapse in 2 years after the interruption of treatment [3].
Bowel programs
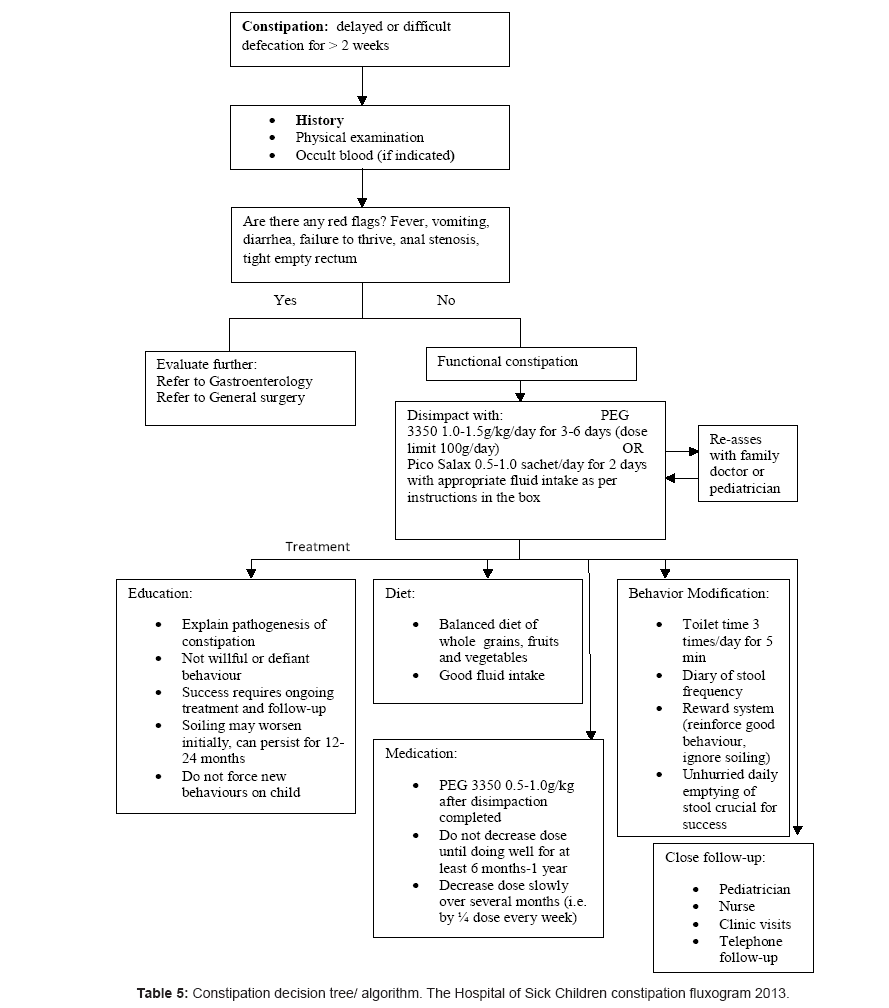
Virtually all of our patients are treated as if they are constipated, regardless of history. We thus reinforce initially set times for the child to have use of the toilet. We also institute a high content fiber diet and stool softeners, if needed. Depending on the degree of constipation (i.e. soiling, severe straining and blood during defecation) a more aggressive clean out regimen might be necessary. Available oral laxatives consist of osmotic and stimulant laxatives. Although oral laxatives are widely used in the pediatric population, to date, only 2 randomized controlled trials have compared the effectiveness of oral laxatives versus the use of a placebo [41,42]. Both studies concluded that PEG was more effective than placebo in increasing frequency of bowel movements, reduction of hard stools, pain and straining during defecation. Several RCT’s have compared the effectiveness of PEG and lactulose; however, it is difficult to draw firm conclusions, due to different inclusion criteria, outcome measures, dosages and study designs. A recent Cochrane review concluded that the use of PEG is superior to lactulose for the outcomes of stool frequency per week, form of stool, relief of abdominal pain and the need for additional products [43]. It is clear however that more studies are necessary to determine and understand the role of different laxative treatments in childhood constipation. Frequently used oral laxative agents for maintenance therapy are listed in Table 5. Our recommended dose for clean out with PEG is 1 g/kg po BID for 7 days; maintenance 1 g/kg, po, daily for minimum 6 months to 1 year. If no response is obtained, the child may need hospital admission for disimpaction with high dose PEG 3350 through Nasogastric tube and/ or fleet enemas.
| Anatomic: ectopic ureter, female epispadias, congenital megaprepuce, labial adhesions |
| Behavioral: voiding postponement, vaginal reflux |
| CNS, neurogenic bladder |
| Developmental |
| Endocrine, renal |
| Functional (Hinman syndrome) |
| Genetic (neuromuscular disorders) |
| Habitual |
Table 6: Pediatric Urinary Incontinence. Differential diagnosis. The “ABC’s.
Pelvic floor muscle awareness and relaxation
Toilet posture and relaxed voiding techniques should be addressed with the child and parents as well as Kegel exercises. Biofeedback therapy has demonstrated clinical use in helping children with pelvic floor retraining as an adjunct to behavioral modification [44-47]. Patients with inability to store urine, as OAB patients, are also placed on behavioral therapy. This may be supplemented with pelvic floor retraining to help with bladder outlet incompetence. However, medical therapy with anticholinergics is the mainstay of treatment for patients with storage problems related to LUTD [48]. Neuromodulation may be applicable in the same context as biofeedback.
Pharmacological therapy
The use of prophylactic antibiotics should be considered in the management of children with BBD and recurrent UTIs. The most recent American Urological Association Vesicoureteral reflux guidelines (Peters, J Urol 2010) recommends that prophylaxis be instituted when BBD co-exists with VUR, especially if there are renal cortical abnormalities [1]. Still the role of antibiotics is controversial with or without reflux. In this section, we will not discuss medications indicated for LUTD refractory to initial treatment with urotherapy and biofeedback, given that these cases should be referred to the specialist for appropriate investigation and management. We don’t recommend instituting anticholinergics, to relax the bladder, or alpha blockers, to potentially loosen the outlet, until all non-pharmacologic retraining has been assured. Thus, discussion of the pros and cons of pharmacotherapy are beyond the scope of this review.
BBD is a common condition seen in primary care practice. To manage patients appropriately, primary doctors must elucidate whether this has resulted in failure to store or failure to empty the bladder. Detailed history, physical examination and direct observation of the urinary stream may give crucial information towards more accurate diagnosis. Constipation should be addressed and managed concomitantly. Most of the patients with BBD will respond to urotherapy and will not need medications or further surgical procedures. Therefore, they likely can be evaluated and treatment instituted without early referral to a specialist. Clearly, however since BBD is a spectrum, most severe and recalcitrant cases may require more specialized involvement and it is equally important to recognize these red flags in these children.