Journal of Sleep Disorders & Therapy
Open Access
ISSN: 2167-0277
ISSN: 2167-0277
Perspective - (2016) Volume 5, Issue 5
Study Objectives: In patients with severe obstructive sleep apnea syndrome (OSAS), continuous positive airway pressure (CPAP) is first-line therapy. Compliance to CPAP is sometimes a problem, and mandibular advancement device (MAD) is then an alternative. However, this alternative is often not effective. It was hypothesized that patients suffering from OSAS would have a freer airway, resulting in a decreased apnea-hypopnea index (AHI), through use of a cervical collar (CC) to extend the neck. To study the effect of this new therapy, a randomized crossover study was conducted to compare MAD monotherapy with CC/MAD combination therapy.
Methods: Eight patients with severe OSAS (AHI>30) who had ceased to use CPAP were enrolled in the randomized crossover study. Four patients started with MAD and four with CC/MAD for one week followed by a wash-out period and then cross-over. Polygraphic sleep recordings were performed at baseline and after each therapy.
Results: The baseline AHI was 51.5 ± 22.5. AHI was reduced to 30.4 ± 23.2 through MAD monotherapy, and to 14.9 ± 10.2 through CC/MAD combination therapy. The effect of the combination therapy was statistically significantly (p=0.018) better than that of the monotherapy. Four patients were achieved an AHI<10/h through use of the combination therapy.
Concusions: The study showed a significant reduction in AHI scores in patients with severe OSAS through use of the CC/MAD combination therapy as compared to the MAD monotherapy. This first report indicates a new possibility for treating severe OSAS in non-compliant CPAP users.
Keywords: Cervical collar, CC/MAD combination therapy, Noncompliant CPAP users, Obstructive sleep apnea
AHI: Apnea-Hypopnea Index; CC: Cervical Collar; CPAP: Continuous Positive Airway Pressure; CMSC: Cervico Mandibular Support Collar; MAD: Mandibular Advancement Device; ODI: Oxygen Desaturation Index; OSAS: Obstructive Sleep Apnea Syndrome; ΔAHI: The difference in AHI
Obstructive sleep apnea syndrome (OSAS) is a common disease in the adult population [1]. OSAS is also associated with increased risk for occupational and road accidents as a result of fatigue and daytime sleepiness [2,3]. Furthermore, patients with untreated moderate and severe OSAS run an increased risk of cardiovascular morbidity [4-6]. CPAP is the most effective treatment for patients with severe OSAS; however, 29%-83% of patients use CPAP for less than 4 hours a night due to the practical difficulties of using the CPAP device [7]. Wolkove et al. found significant problems with CPAP compliance in long-term treatment. Among 80 patients who participated in their study, 15% had abandoned CPAP after 10 months, and 31% never commenced therapy after the initial diagnosis [8]. Oral therapy such as use of a mandibular advancement device (MAD) has been shown to be an effective treatment for mild to moderate OSAS [9-11]. The main function of MAD is to protrude the mandible forward, causing the airway to remain open during sleep [9]. MAD therapy is also an alternative when patients reject CPAP or when CPAP is not tolerated for various reasons [12]; however, the effect is less powerful than that achieved with CPAP [13].
There are different causes of OSAS, and being overweight and sleeping in the supine position play significant roles. Obese patients show an increase in pharyngeal tissue, which constitutes an anatomical basis for respiratory obstruction during sleep [14]. The supine sleeping position generates mandibular retraction and tongue collapse, which have the same result [15]. Skinner et al. [16] compared the effectiveness of a cervicomandibular support collar (CMSC) with standard CPAP. The CMSC’s function was to prevent downward displacement of the mandible as well as to maintain the head in slight extension during sleep. Their study could not demonstrate that the CMSC used as a single therapy was an effective treatment [16].
Finding a treatment to prevent collapse of the airway during sleep is an interest resulting from knowledge of conditions in the upper respiratory airway that is associated with OSAS. An important aspect is that extending the neck and pulling out the mandible reduce mechanical barriers in the upper airways. Our hypothesis was that patients suffering from severe OSAS would have a freer airway through use of a cervical collar (CC) to extend the neck. The knowledge that the function of MAD is to protrude the mandible forward, causing the airway to remain open during sleep, has led to the hypothesis that CC and MAD would have a synergistic effect. To study this effect with the CC, a pilot randomized crossover study was conducted to compare MAD monotherapy with CC/MAD combination therapy in patients with severe OSAS.
Ethics statement
This study was approved by the Stockholm Ethics Committee (2012/1084-31/4). The patients agreed to participate and gave their written informed consent. The patients received detailed information and were instructed to discontinue the treatment in the event of discomfort or other complications. They were informed they could cease participation whenever they wished.
Eight patients with severe OSAS were included in the study. They had all been prescribed CPAP therapy at the ENT clinic at the County Central Hospital (Malarsjukhuset) in Eskilstuna, Sweden but had ceased CPAP-treatment due to intolerance. The inclusion criteria were: severe OSAS (AHI>30/h), BMI less than 35, non-pregnant, and no medical history of whiplash, rheumatic disease, or osteoporosis. Patients with fibromyalgia, psychiatric and neurological disorders, and with alcohol and drug abuse problems as well as patients being treated with different kinds of sedative were also excluded. To identify the study population, a total of 166 patients who had failed follow-up during the last two years were contacted by telephone. Of these 166 patients, 131 still used their CPAP, 8 patients could not be reached, and 27 patients had ceased CPAP treatment due to discomfort (e.g., dry mouth or nose, runny nose, headache). Of these 27 patients, 16 agreed to be included in the study, and 12 (10 men and 2 women) met the inclusion criteria. Four patients dropped out at the onset of the study. Eight patients completed the study; all of them were men aged 56.1 ± 10.2 (mean ± SD).
Patients underwent a physical examination that included measurements of blood pressure, cardiac, nose-throat and thyroid status prior to the study. They were recorded using polygraphy to obtain baseline values for sleep-disordered breathing and to ensure that they still had an AHI of >30/h. Patients were then randomized into two groups: starting with MAD monotherapy or with combination CC/MAD therapy. Patients had to choose between two envelopes containing letter A or B. Thedevices (MAD or CC/MAD) were used for a period of one week until the patients felt comfortable with the treatment. Theneach patient underwent full-night polygraphy. Patients could choose any sleep position they wished. Aftersleep registration, the patients slept without any treatment for at least one week (washout period). Thena crossover to the other treatment condition was made.
Mandibular advancement device (MAD)
Each patient received a MAD from a dental specialist at Malarsjukhuset in Eskilstuna. The MAD was individually adapted according to construction bites. The device was adjusted after a 1- month habituation period in patients with side effects.
Cervical collar (CC)
In our study, a neck collar (Vista CC) that already existed on the market was used, Figure 1. It is intended for indications of various diseases such as traumatic cervical injury, cervical disc herniation and other neck problems. The main reason we chose the Vista CC was its design, which allows adjustment of the elevation level to achieve sufficient effect, i.e., extending the neck. The CC has six height settings to choose from, and adjustment between them is easy. All patients were instructed to select the highest level for the CC during polygraphy.
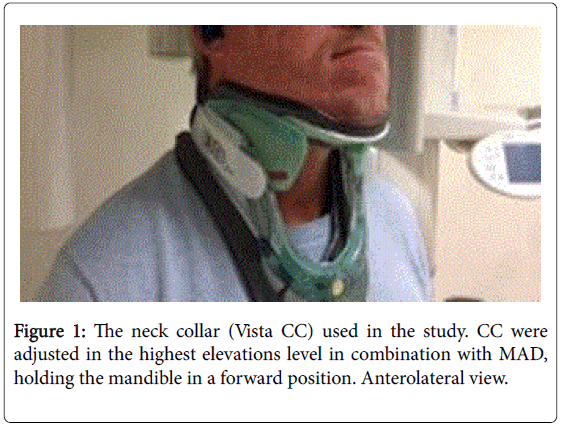
Figure 1: The neck collar (Vista CC) used in the study. CC were adjusted in the highest elevations level in combination with MAD, holding the mandible in a forward position. Anterolateral view.
Polygraphy
Polygraphy was performed in patients' homes with Embletta PDS recorder equipment (Medcare, Reykjavik, Iceland). RemLogic 3.2 analysis software (Embla Systems LLC, Thornston, CO) was used. All sleep recordings were evaluated and scored manually by the same experienced sleep technician. The patients filled in standardized questionnaires about sleep time (time of sleep onset and awakenings) and sleep quality. Sleep time was defined when the recording showed a continuous curve of smooth breathing in combination with non-bodymovements or the presence of apnea/hypopnea. Apneas, hypopneas and desaturations were scored according to the criteria of the American Academy of Sleep Medicine [17]. Obstructive apnea was defined as a decrease in respiratory airflow of more than 90% for more than 10 seconds with preserved respiratory movement in the thoracic or abdominal wall. Hypopnea was defined as a reduction in nasal pressure signal of 50% or more from baseline for >10 sec in combination with an oxygen desaturation (OD) of >3% (4B Rule). OD was defined as a reduction in saturation of at least 3% from baseline.
AHI was defined as the total sum of apneas and hypopneas divided by registration/sleep time.
Differences in baseline measurements between treatment groups were analyzed using t-tests. In the primary analysis, paired t-tests were used to test mean differences between MAD monotherapy and CC/MA combination therapy. To test for violation of the normal distribution assumption we used the Shapiro-Wilks test, with a p-value of 0.08 (MAD) and 0.10 (CC/MAD) respectively, indicating they both follow a normal distribution.
However, considering the small sample the Wilcoxon signed rank test was also used to test the difference between treatment periods. As is common, we set the significance level (α) generally at 0.05. That together with the small sample size (n=8), causes the power of the test to be fairly low.
The power of the t- test and the Wilcoxon signed rank test of no difference in AHI between MAD and MAD/CC was 0.23 and 0.20 respectively. The existence of a carryover effect was examined by conducting a t-test on the difference between treatment groups using measures from both treatment periods.
Four patients started with MAD (Group A), and four started with CC/MAD (Group B). The characteristics of both groups were comparable. The demographic data are shown in Table 1. The mean of baseline AHI for both groups was more than 51; for four patients among them, AHI ranged from 57-96.
| Variables | Group | p-value | |
|---|---|---|---|
| A | B | ||
| Age | 55.5 ± 2.9 (54-60) | 56.7 ± 19.8 (38-72) | 0.88 |
| BMI | 28.7± 3.7 (26.8-34.3) | 28.8 ± 3.2 (24.4-32.1) | 0.97 |
| AHI | 45.3 ± 16.4 (30.8-57.4) | 57.5 ± 28.5 (36.1-96.7) | 0.49 |
| Data are presented as mean ± SD (range) | |||
Table 1: Demographic data and baseline values for AHI from the two randomized.
All eight patients completed both treatments. No severe adverse event was reported during the study. The outcome data for each patient are shown in Table 2.
| Patient No |
Random Type |
Baseline | MAD | CC/MAD | |
|---|---|---|---|---|---|
| AHI | AHI | AHI | ΔAHI | ||
| 1 | A | 30.8 | 21.3 | 12.3 | -9.0 (-18.5) |
| 2 | B | 96.7 | 45.8 | 27.4 | -18.4 (-69.3) |
| 3 | B | 36 .1 | 7.7 | 8.2 | 0.5 (-27.9) |
| 4 | A | 31.6 | 9.7 | 5.9 | -3.8 (-25.7) |
| 5 | A | 57.4 | 61.6 | 29.7 | -31.9 (-27.7) |
| 6 | B | 61.2 | 63.7 | 22.6 | -41.1 (-38.6) |
| 7 | B | 36.3 | 10.8 | 4.6 | - 6.2 (-31.7) |
| 8 | A | 61.6 | 22.8 | 8.1 | -14.7 (-53.5) |
| Mean ± SD | 51.5 ± 22.5 | 30.4 ± 23.2 | 14.9 ± 10.1 79.8) |
-15.5 ± 36.1 (-36.5 ± | |
Table 2: AHI scores for each patient.
There was a clear reduction in mean AHI with CC/MAD combination therapy compared to MAD monotherapy (-15.5 ± 36.0) (p=0.018) and compared to baseline (-36.5 ± 79.8) (Figure 2). In two patients, AHI decreased to < 10/h with MAD monotherapy, and four patients achieved an AHI< 10/h with the CC/MAD combination.
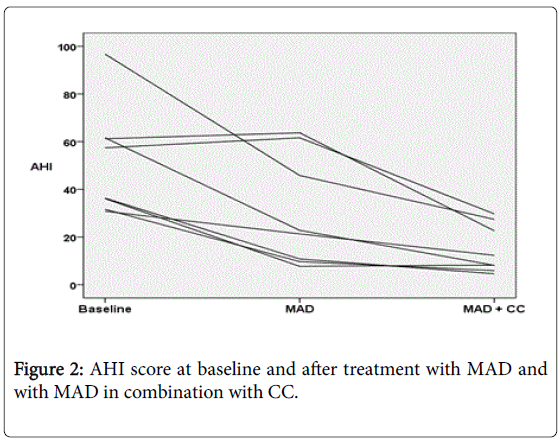
Figure 2: AHI score at baseline and after treatment with MAD and with MAD in combination with CC.
One patient’s AHI was somewhat higher with CC/MAD than with MAD, but both values were < 10/h. The greatest reduction in AHI (-69.3 index points) was shown in a patient with baseline AHI 96.7.
In case of violation of the normality assumption the t-test was complemented with the Wilcoxon signed ranks test for the difference in AHI between MAD and CC/MAD, which resulted in a p-value of 0.016.
The baseline oxygen desaturation index (ODI) was 50.3. Table 3 shows that the mean ODI decreased significantly from 31.2 with MAD to 16.5 with CC/MAD (p=0.027).
| Polygraphy data | Baseline | MAD | CC/MAD | p-Value |
|---|---|---|---|---|
| Apnea + Hypopnea/h (AHI) | 51.5 ± 22.5 (30.8-96.7) | 30.4 ± 23.2 (7.7-63.7) | 14.9 ± 10.1 (4.6-29.7) | 0.018 |
| Body mass index | 28.5 ± 3.2 (24.4-34.3) | 29.2 ± 4.8 (24.4-35.9) | 29.3 ± 3.4 (25.0-35.9) | 0.391 |
| Oxygen Desaturation Index (ODI) | 50.3 ± 22.6 (29.4-98.3 | 31.2 ± 21.6 (9.7-57.6) | 16.5 ± 12.9 (4.9-41.3) | 0.027 |
| Average Oxygen Saturation | 89.6 ± 3.6 (82.6-94.7) | 90.3 ± 2.5 (85.9-94.6) | 90.8± 2.5 (87.8-94.9) | 0.957 |
| Total sleep time (min) | 377 ± 38.5 (313-422) | 427 ± 67.7 (332-504) | 349 ± 43.8 (282-422) | 0.006 |
| Supine sleep time (%) | 69.6 ± 35.8 (7.2-100) | 62.8 ± 33.3 (14.7-94.5) | 71.8 ± 28.9 (32.8-100) | 0.005 |
| AHI supine position | 59.3 ± 18.3 (32.1-91.9) | 46.6 ± 29.4 (7.5-82.9) | 18.2 ± 11.2 (5.6-36.9) | 0.009 |
| AHI non-supine position | 34.4 ± 36.0 (0.0 -102) | 20.3 ± 18.8 (6.6-61.8) | 2.9 ± 2.0 (0-5.5) | 0.04 |
Table 3: The relevant values for recorded polygraphic data.
The reduction patterns for ODI and AHI show approximately the same numerical trend. There was a clear reduction in AHI in both the supine and non-supine positions. Baseline AHI in the non-supine position was 34.4.
Supine sleep time was longer with CC/MAD compared to MAD and baseline (p=0.005). BMI did not change significantly between recordings. Average oxygen saturation showed small improvements with CC/MAD (p=0.957).
The present study showed a significant reduction in AHI scores in adults with severe OSAS using CC/MAD combination therapy compared to using MAD monotherapy.
The difference was even greater compared to baseline AHI and ODI. Four patients were achieved an AHI< 10/h using CC/MAD combination therapy. All patients were achieved an AHI< 5/h when they sleep in a non-supine position in combination with CC/MAD. To confirm this hypothesis, further studies using polysomnography must be conducted to delineate sleep stages. Our study also showed that AHI was reduced significantly in patients with CC/MAD combination therapy, despite the fact that they spent more time in the supine position.
CPAP is the most effective treatment for patients with severe OSAS; however, treatment effectiveness is limited by compliance with longterm treatment [7,8,18]. Maintaining this compliance requires intensive education, motivational enhancement and support [19,20]. Patients with severe OSAS need to use CPAP to prevent the risks associated with the disease. MAD is an alternative to CPAP but unfortunately does not have the same effect in patients with severe OSAS [13]. MAD has the best effect in patients with mild to moderate OSAS [9-11]. Pharyngeal surgery is another option for treatment; however, long-term studies have shown suboptimal results. The surgery is also associated with some risk of side effects [21,22]. There is therefore a need for alternative forms of treatment for patients with severe OSAS who cannot use CPAP.
As far as we know, our study is the first to investigate the effect of neck extension in combination with MAD. We found that the treatment was effective in reducing AHI and ODI in patients with severe OSAS. The strength of this study includes its randomized crossover design, which offers more data than a study performed with a limited number of patients. However, there are a number of limitations to this pilot study that should be considered. Most importantly, all recordings were performed with polygraphy, and sleeping time could therefore only be estimated by the manual evaluation of sleep by sleep technicians and standardized questionnaires. In addition, hypopneas were defined according to the AASM scoring rules 2007 that have later been updated. However, identical scoring rules were used before and after each treatment period. CC/MAD may cause discomfort, which could reduce sleep time and thus the AHI. However, the AHI for polygraphy in this study was based on recording times obtained while patients slept. Another limitation of the study is the small number patients, although we did perform extensive data analysis for each patient. Given that the present investigation is based on eight patients, it should be considered a pilot study. A larger, randomized, and placebo-controlled multicenter study is therefore warranted. Gender is also an issue, as the present study included only male participants. This is related to the way we identified our patients. There were no women who met our inclusion criteria.
Our results showed a significant reduction in AHI scores in adults with severe OSAS after using CC/MAD combination therapy for one week. To confirm the patients’ compliance with long-term treatment using this concept, follow-ups will be carried out. The Vista CC was not made specifically for treating patients with OSAS, and construction could therefore be optimized.
Skinner et al. [16] compared the effectiveness of a cervicomandibular support collar (CMSC) with standard CPAP. Their study did not demonstrate that CMSC was an effective treatment. We believe that the Vista collar that was used in the present study provides higher elevation of the head than the CMSC does, thus enabling freer airways. Another possibility is that a cervical collar is only effective in the combination with MAD.
We have not found any similar previous studies, though many have tested different positioning methods. Head extension using a CC provides more space in the upper airway. The MAD moves the mandible forward, and the CC provides an additional effect by closing the mouth and thus increasing the degree of protrusion. This increases the airway space between the tongue and the posterior pharyngeal wall.
In conclusion, the present randomized crossover pilot study showed a significant reduction in AHI in patients with severe OSAS through the use of CC/MAD combination therapy as compared to MAD monotherapy. Although the study has several limitations, this first promising report may lead to new therapy using a CC for this group of patients-patients with severe OSAS who are difficult to treat owing to non-compliance with CPAP therapy. Further studies are needed to confirm the benefits of this new CC/MAD combination therapy and also CC treatment as monotherapy for OSAS cases of varying severity.
The authors declare no financial support or other benefit that could
be interpreted as a conflict of interest.
This study was supported by the Research and Development Center, Sormland County Council, Sweden. We are thankful to Fredrik Granstrom for his contribution to the statistical analysis and to Ronnie Jonsson for his work as sleep technician at the Department of Clinical Physiology MSE, including his scoring of the sleep recordings.