Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2012) Volume 1, Issue 1
We present a patient with respiratory insufficiency due to progressive lung metastases of thyroid cancer. Low dose i.v. vinblastin, oral cyclophosphamide and s.c. enoxaparin produced dramatic clinical improvement, a drop in thyroglobulin and prolonged disease stabilisation. This new way of giving classical chemotherapy is called metronomic chemotherapy. Its anti-angiogenic basis of activity is corroborated by the more recent drugs in thyroid cancer which share this mechanism.
<Until recently, there was no effective chemotherapy for iodine refractory thyroid cancer. The use of lower dose chemotherapy (called “metronomic chemotherapy”) like in other endocrine responsive tumors was never evaluated in this tumor type. The clinical benefit, as well as the prolonged disease stabilisation by metronomic chemotherapy in a palliative patient with massive lung metastases, illustrates empirically the anti-angiogenic effect of this type of chemotherapy. It predated the recent avalanche of specific angiogenesis inhibitors in this disease.
Our patient first presented at the age of 55 with a large mediastinal mass in 2000. After resection this proved to be a follicular thyroid adenocarcinoma weighing 270 grams. Postoperatively, he received a first dose of radioactive iodine (I*) at a dosage of 100 mCi. In 2003 two doses of 100 mCi each were given for an asymptomatic rise in thyroglobulin. In 2004 a local lymph node recurrence was detected and resected. That time lung metastases were documented on imaging. These were treated with one dose of 150 mCi of I*. A rise in thyroglobulin and increase in size of lung metastasis were treated with two doses of 150 mCi I* in 2005.
In 2008 there was an increase of the lung metastases on PETscan and chest x-ray. Although most lung metastases didn’t show any further iodine uptake, indicating iodine resistance, a final dose of 150 mCi was nevertheless administered. The re-evaluation three months later showed further progression of the lung metastasis and a further increase of serum thyroglobulin to 90.500 ng/ml on 10/11/2008. The patient, then 63 years, was therefore referred to a tertiary cancer centre to participate in a phase II trial with a new tyrosine kinase inhibitor. Unfortunately this protocol was closed and the patient was treated with sandostatin injections. Under this treatment the patient showed progressive shortness of breath and dyspnoea requiring an urgent admission in our hospital. At admission the patient was extremely hypoxic with a peripheral saturation of 80% on pulse oximetry. Chest x-ray showed innumerable lung metastases and bedside sonography showed neither arguments for deep venous thrombosis nor other causes of respiratory failure. Biochemistry showed a significant increase in thyroglobulin level (202.000 ng/ml) under the previous treatment with sandostatin. With oxygen and bed rest, the patient had slightly recovered on the following day, allowing a first dose of oral cyclophosphomide (50 mg), i.v. vinblastin (3 mg) and subcutaneous enoxaparin (40 mg). After one week of oral cyclophosphomide + sc enoxaparin, the patient had sufficiently recovered allowing a second dose of i.v. vinblastin (3 mg). The patient was then discharged home. During the following eighteen months, the patient was treated with this regimen on an outpatient basis without major haematological or other complications. After an initial drop in thyroglobulin the values essentially stabilised for more than fourteen months (Chart 1). Subsequent CT scans of the chest all showed persistent disease stabilisation of the numerous lung metastases (Figure 1a,1b and Figure 2a,2b). In October 2011, after 24 months of treatment, progression was documented by a rising thyroglobulin over 200 000 ng/ml and a slight increase in lung lesions (Figure 3). The patient was therefore referred to a tertiary cancer center to start sorafenib in a compassionate use programme.
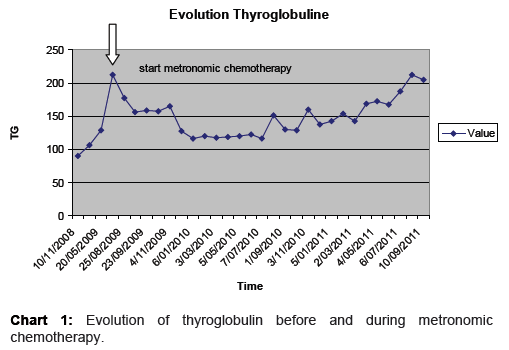
Chart 1: Evolution of thyroglobulin before and during metronomic chemotherapy.
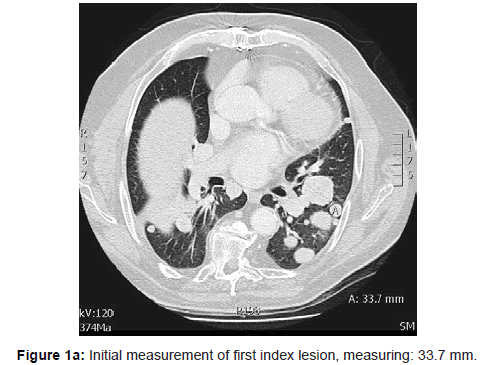
Figure 1a: Initial measurement of first index lesion, measuring: 33.7 mm.
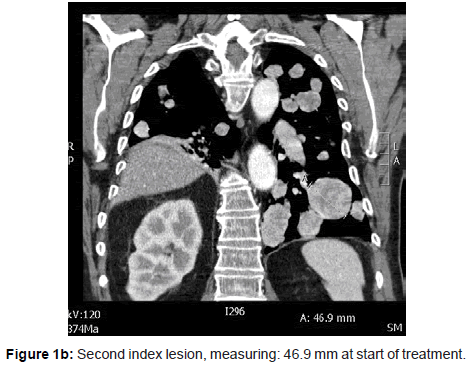
Figure 1b: Second index lesion, measuring: 46.9 mm at start of treatment.
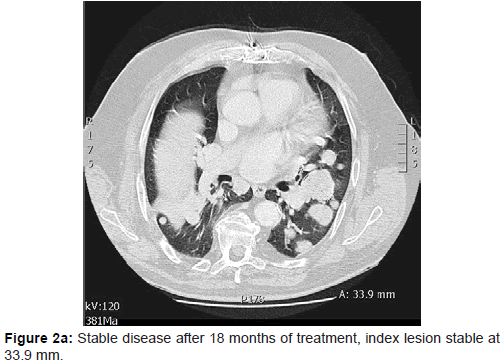
Figure 2a: Stable disease after 18 months of treatment, index lesion stable at 33.9 mm.
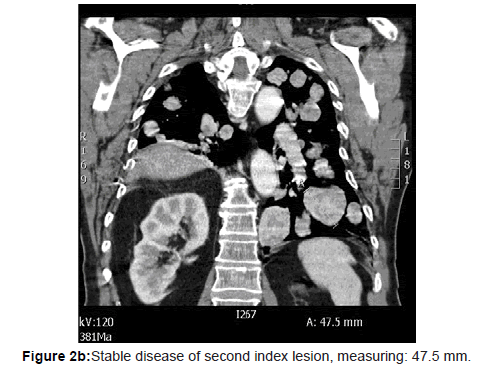
Figure 2b: Stable disease of second index lesion, measuring: 47.5 mm.
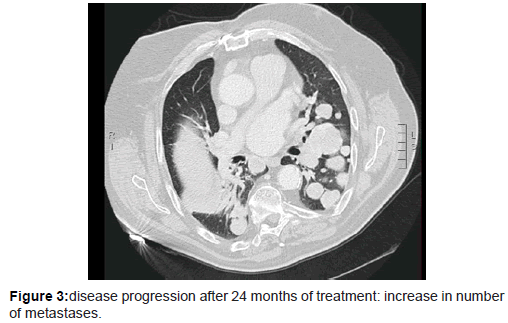
Figure 3: disease progression after 24 months of treatment: increase in number of metastases.
Thyroid carcinoma is the most common malignancy of the endocrine system, and the vast majority of these carcinomas are of the papillary or follicular subgroups. The majority of these welldifferentiated thyroid carcinomas (DTCs) are highly treatable by surgery, followed in most patients by I131 and TSH-suppressive doses of levothyroxine [1]. Indeed, the overall 10-yr survival rate is 93% for patients with papillary thyroid carcinoma (PTC) and 85% for patients with follicular thyroid carcinoma (FTC). However, about 2% of patients with PTC and 6% of those with FTC or Hurthle cell carcinoma have distant metastasis at the time of diagnosis [2], and an additional group of patients develop identifiable distant metastases during longterm follow-up [3,4]. The long-term disease-specific survival of patients with either DTC with distant metastases is less than 50% at 5 yr [2,4,5]. Furthermore, a subgroup of these patients with distant metastases, including those with metastases that concentrate 131I poorly, have brain, bone, or large lung metastases or bulky fluoro deoxyglucose-avid metastases [6-8] that typically do not respond to 131I therapy.
Alternative systemic treatments for widely metastatic DTC using cytotoxic chemotherapy have been of limited utility. Until recently, chemotherapy for metastatic radio-iodine refractory thyroid cancer was limited to anthracyclines and some case reports [9]. This has recently changed with the advent of efficient targeted therapies [10] initially in medullary thyroid cancer and subsequently also in papillary and follicular cancer. These targeted treatments essentially block intracellular pathways or have anti-angiogenic properties.
Comprehensive studies of mutation pathways in DTC and MTC have been undertaken in the past two decades [11,12]. The knowledge gained from these analyses made DTC and MTC amenable to designer therapeutics. The most important findings centre on the discovery of oncogenic kinases, as well as the elucidation of various signalling pathway adaptations occurring in malignant cells. Of the oncogenic kinases, BRAF V600E mutation and RET/PTC mutations are being targeted as potential pathways for therapeutic intervention. Both of these mutations have the potential to activate the mitogen-activated protein kinase (MAPK) pathway downstream [10].
The BRAF inhibitor studied most in thyroid cancer is sorafenib. Sorafenib is an oral tyrosine kinase inhibitor. A number of phase II trials of sorafenib involved advanced or metastatic DTC. These patients’ tumors demonstrated partial responses in 15–27% of participants, and stable disease in a little over 34–61% [13-15].
Sunitinib is a tyrosine kinase inhibitor affecting VEGFR 1/2/3, RET, RET/PTC1. Of DTC and MTC patients enrolled in a phase II trial of sunitinib receiving 50 mg/day, partial response was observed in 13% of patients with DTC, while stable disease was the best response in 68% of patients with DTC [16,17].
Other important signalling cascades being investigated for the possible development of therapeutic kinase inhibitors are the VEGF and PDGF pathways. VEGF is a pro-angiogenic factor that binds to two receptor tyrosine kinases (VEGFR-1 and VEGFR-2), of which VEGFR-2 is widely recognized to be the primary mediator of angiogenesis. PDGF-B is required for the maturation of microvasculature, while tumor-derived PDGF-A recruits angiogenic stroma to the tissue. VEGFR and PDGFR mutually support the increased activity of each other [18]. Increased VEGF expression appears to be related to worse prognosis, increased risk of recurrence, and the presence of metastasis [19].
Pazopanib is a second-generation oral small molecule kinase inhibitor that targets VEGFR-1, 2, and 3, as well as alpha and beta PDGFR [20]. A phase II study completed in early 2009 of thyroid cancer patients led by the Mayo Clinic demonstrated a confirmed partial response rate by RECIST criteria in 49% of enrolled subjects (18 patients).
Motesanib is an oral tyrosine-kinase inhibitor. It demonstrates both direct antitumor and anti-angiogenic properties [21]. Phase 1 trials were encouraging with 3 DTC patients registering a partial response [22]. A subsequent phase II trial administering 125 mg/day to patients with DTC demonstrated a partial response in 14% of patients, while 35% of patients had stable disease after 48 weeks [23].
All these newer drugs underline the importance of angiogenesis in thyroid cancer and its inhibition by blocking the VEGF-R. It is therefore logical that classical chemotherapy, with the mainly cytotoxic activity, showed little effect.
A more recent way of giving chemotherapy, called “metronomic chemotherapy”, has also important anti-angiogenic properties by blocking endothelial proliferation [24]. It has proven efficacy in endocrine sensitive tumors like prostate cancer and breast cancer. Partial responses and disease stabilisations were obtained with prolonged administration of cyclophosphomide [25-27]. Thyroid cancer was never before treated with this way of prolonged chemotherapy. Angiogenic inhibition by chemotherapy has therefore not been explored in these rare tumors. The success in our patient on symptom control and decrease in thyroglobulin rests on the unique method of activity of this particular administration of chemotherapy. By using low dose cyclophosphomide orally and weekly vinblastin, we applied a regimen with maximal anti-angiogenic properties as demonstrated in several prior publications [28,29]. We also applied the antitumoral effect of enoxaparin in this regimen, which works by inhibition of tumor cell adhesion [30]. This led to an initial decrease in thyroglobulin and prolonged disease stabilisation exceeding 18 months, as can be seen in the most promising of all recent anti-VEGF-R inhibitors.
This is the first case report on the clinical benefit of metronomic chemotherapy in diffuse lung metastases of thyroid cancer. This type of chemotherapy works by an antiangiogenic mechanism and thus, this case report confirms the common pathway with the more recent drugs developed for thyroid cancer.