Medical & Surgical Urology
Open Access
ISSN: 2168-9857
ISSN: 2168-9857
Research Article - (2018) Volume 7, Issue 3
Keywords: Renal replacement lipomatosis; Psoas abscess; Xanthogranulomatous pyelonephritis
Renal replacement lipomatosis is chronic disease process which is usually unilateral and follows calculus disease characterized by vicious cycle of atrophy or destruction of renal parenchyma due to chronic inflammation triggering proliferation of fatty tissue. Fatty tissue proliferation begins within the renal sinus and gradually occupies hilum and perinephric/periureteric space and contributes to pressureinduced thinning and loss of renal parenchymal bulk. Patients usually present with complaints of recurrent flank pain, fever, weight loss and mass per abdomen. Role of various imaging modalities has been described but computed tomography (CT) and magnetic resonance imaging (MRI) are considered superior among all of them for characterization of pathology and to differentiate it from other similar appearance fatty masses of retroperitoneum, most importantly xanthogranulomatous pyelonephritis which has similar etiological factors and presentation.
A 60-year male presented with chronic dull pain in the right flank, low-grade fever, and long term history of renal stones to our institute. On clinical examination, there was vague slightly tender mass with the fullness of right flank. Routine blood investigation showed raised values of inflammatory markers (CRP, ESR, WBC). Abdominal radiograph showed staghorn opacity in right lumbar region. Ultrasound examination of abdomen revealed predominantly hyperechoic mass in right lumbar region with staghorn calculus and renal parenchymal atrophy. After urological consultation patient underwent CT examination with clinical suspicion of xanthogranulomatous pyelonephritis. On 64 slice CT scanner plain and contrast study was performed which showed large fat-attenuation reniform mass lesion occupying right renal fossa with a large hyperdense calculus, thinned out renal parenchyma and poorly functioning kidney. In addition, a large multiloculated collection was seen in right psoas muscle. On these imaging findings, the radiological diagnosis of renal replacement lipomatosis with psoas abscess was made. The patient underwent right nephrectomy in view of poorly functioning kidney with drainage of psoas abscess. Intra-operatively large amount of fat was seen in right hilar and perirenal location. Renal artery and vein was clipped. No perirenal adhesions or was identified. Post-operative period went uneventful.
Specimen measured 11 x 6 x 5 cm with intact Gerota’s fascia, irregular nodular external surface and fibro-fatty tissue attached on the kidney. Cut surface appeared yellowish with lot of fatty tissue deposition. There was complete loss of renal architecture with significant atrophy. Microscopic examination revealed complete loss of renal architecture with extensive fatty tissue infiltration without normal glomeruli and there was thyroidisation of tubules. Interstitium revealed mononuclear infiltration and fibrosis. No evidence of malignancy was seen.Histopathology of tissue confirmed the diagnosis of renal replacement lipomatosis (Figures 1-3).
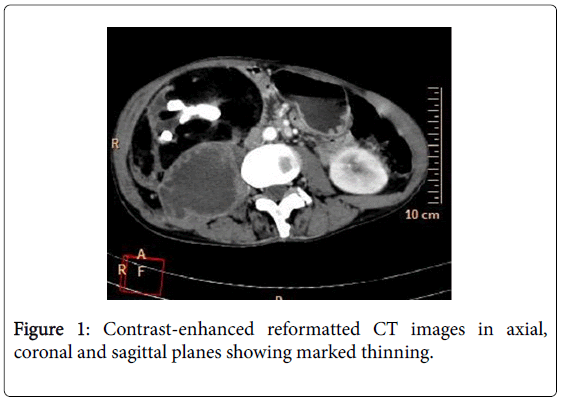
Figure 1: Contrast-enhanced reformatted CT images in axial, coronal and sagittal planes showing marked thinning.
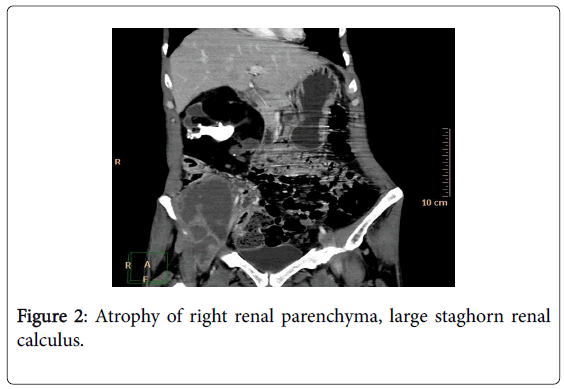
Figure 2: Atrophy of right renal parenchyma, large staghorn renal calculus.
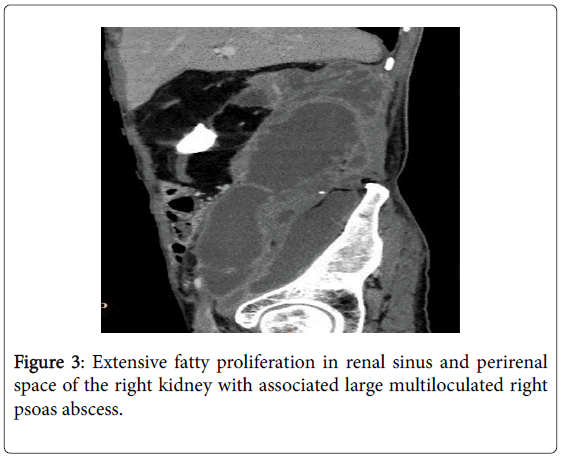
Figure 3: Extensive fatty proliferation in renal sinus and perirenal space of the right kidney with associated large multiloculated right psoas abscess.
Renal replacement lipomatosis (RRL) also known as fibrolipomatosis is an uncommon condition, which occurs secondary to atrophy or destruction of renal parenchyma by chronic inflammation. RRL is most commonly seen in association with calculus disease (in >70% patients), however it can be associated with other chronic inflammatory pathologies such as chronic pyelonephritis, renal tuberculosis and transplant patients [1,2].
Fat proliferation begins from the renal sinus also called as renal sinus lipomatosis and eventually replaces the entire renal and perirenal tissue by lipomatous mass in more severe form called as total replacement lipomatosis [1]. The disease process is presumed to contribute to atrophy of renal parenchyma by increasing pressure over pelvi-calyceal system or direct parenchymal invasion which helps to distinguish this from other medical conditions causing increase in retroperitoneal fat volume like obesity, Cushing's disease or long-term exogenous steroid exposure [3].
Renal replacement lipomatosis (RRL) is prevalent in old age males during 5-6th decades with the long-term history of renal stones. Incidence of RRL increases with increasing age and obesity. Unilateral involvement is more common in the majority of patient with the longterm history of renal stone particularly stag horn however case reports have been published describing renal replacement lipomatosis in the absence of renal calculus disease. The patient usually presents with non specific complaints of flank pain, fever, weight loss and mass per abdomen.
Various conventional imaging modalities like plain radiograph, Xray intravenous pyelogrpahy and sonography can be used for evaluation of such patients however CT or MRI with MR urography are required for making accurate diagnosis of renal lipomatosis. They also help in distinguishing RRL from other mimickers mainly xanthogranulomatous pyelonephritis, other fat-containing neoplasm of kidney like angiomyolipomas, liposarcomas, lipomas and transitional carcinoma of the renal sinus [4].Cross sectional imaging also tell about the extent and distribution of fat proliferation, parenchymal changes as atrophy or destrucion, associated conditions like pyonephrois/ hydronephrosis or calculus disease and thereby help in presurgical planning. CT scan demonstrates parenchymal destruction with fatty proliferation as negative attenuation same as that of normal adipose tissue. Kidney is usually poorly or non functioning in patients with RRL. CT scan is an accurate method for diagnosing renal replacement lipomatosis and obviates the need for pre-operative invasive diagnostic procedure or diagnostic surgery [5].
Renal replacement lipomatosis and xanthogranulomatous pyelonephritis may mimic each other as well as can coexist in same patient and are difficult to differentiate at times due to common etiological factors like chronic inflammation and renal calculus. Renal replacement lipomatosis shows increased adipose tissue content in renal sinus and perirenal tissues with formation of reniform lipomatous mass lesion while xanthogranulomatous pyelonephritis is characterized by infiltration of lipid-loaded inflammatory foam cells in the renal parenchyma [6]. On CT imaging xanthogranulomatous pyelonephritis shows presence of multiple hypodense lesions in renal parenchyma suggesting abscesses with renal stones, infected hydronephrosis and involvement of surrounding soft tissue or abdominal wall without much evidence of proliferated fat in and around the kidney [7].
Another important diagnostic differential is retroperitoneal liposarcoma which is seen at periphery of kidney, occupying space between kidney and renal capsule without any breach in renal cortex. Similarly RRL can be differentiated from renal angiomyolipoma or lipoma by its association with parenchymal atrophy, calculus and at times perinephric abscess. Fat containing neoplasms are usually located intrarenally or extrarenally outside the renal sinus. Angiomyolipoma also contains varying amount of fat with enhancing soft tissue areas [4].
Recently MRI with MR urography is coming up as diagnostic modality for evaluation of RRL it does not require intravenous contrast administration in patients with poorly or non functioning kidney and can evaluate entire urinary tract even without much dilatation.
The purpose of this article is to described importance of CT imaging in making accurate diagnosis of renal replacement lipomatosis, rule out similar appearing fatty masses of retroperitoneum, differentiate this condition from xanthogranulomatous pyelonephritis, evaluate associated complications as seen in this case and road map to surgery since this condition is still quite uncommon among practicing urosurgeons and radiology people.