Journal of Cancer Research and Immuno-Oncology
Open Access
ISSN: 2684-1266
ISSN: 2684-1266
Research Article - (2017) Volume 3, Issue 1
Objective: To examine the relationship between anogenital abnormalities and the development of anal dysplasia among Human Immunodeficiency Virus (HIV)-negative women.
Methods: This retrospective matched case-control study used administrative data from the 2009-2014 Clinformatics Data Mart. Cases were selected according to the International Classification of Diseases, Ninth Revision, using Clinical Modification codes for carcinoma in situ of the anal canal or anus unspecified, anal intraepithelial neoplasia 1 and 2, abnormal glandular Papanicolaou (Pap) smear of the anus, or Pap smears of the anus with atypical squamous cells, squamous intraepithelial lesions, or cytological evidence of malignancy. Conditional logistic regression analysis was used to calculate odds ratios (ORs) and 95% confidence intervals for the risk of anal dysplasia.
Results: The study included 3,384 HIV-negative women (846 cases and 2,538 controls), mean age 50.1 ± 11.9 years. The odds of being a smoker, having cervical intraepithelial neoplasia (CIN), or anogenital warts were higher for HIV-negative women with anal dysplasia than for those without anal dysplasia (OR =2.5-16.3).
Conclusions: HIV-negative women with anal dysplasia are more likely to have concomitant human papillomavirus (HPV)-related CIN and anogenital warts than women without anal dysplasia. The presence of HPV-associated lesions might have implications for future screening recommendations. HIV-negative women with a history of CIN and anogenital warts could benefit from anal dysplasia/anal cancer screening. Gaining a better understanding of the natural history of anal HPV infections will provide tools to better treat and counsel patients with anal dysplasia.
Keywords: Anal dysplasia; Anal intraepithelial neoplasia; Cervical cytology; Anogenital warts; Cervical intraepithelial neoplasia; HPV; Anal cancer
HPV infection is the most commonly diagnosed sexually transmitted disease in the United States (US) and is associated with the development of anal cancer [1-4]. Anal cancer and its precursor lesions are biologically similar to cervical cancer and caused by persistent HPV infection [2,3,5]. A high proportion of anal cancers are associated with HPV types 16 and 18. Each year, there are 1.8 anal cancer cases per 100,000 persons, with a higher incidence among women [6]. The anal cancer incidence has been increasing at a rate of 2.2% per year over the last decade, with death rates rising an average of 1.7% per year [6]. In 2017, there will be 8,200 new anal cancer cases (5,250 in women and 2,950 in men) and 1,100 deaths (650 in women and 450 in men) [7].
Numerous histological types of malignant tumors develop within the anus, but squamous cell cancers are the most common [7]. Anal intraepithelial neoplasia (AIN) is considered a potential precursor of anal cancer [2]. Although HPV infection can be transmitted through anal intercourse, that is not required for the development of anal HPV infection [8,9]. Risk factors for increased anal HPV incidence and AIN include immunosuppression or organ transplant, men who have sex with men (MSM), HIV seropositivity, women with a history of lower genital tract neoplasia (i.e., cervical or vulvar dysplasia), men having more than 10 female partners, history of anogenital warts or prior history of Sexually Transmitted Diseases (STDs), chronic local inflammation, smoking, race and gender, and radiation therapy [1-5,8,10-12]. A high prevalence of anal cancer has been observed in HIV-positive men and women [1,10-13]. In HIV-negative women with HPV-related pathologies of the vulva, vagina, and cervix, the prevalence of anal high-risk HPV varied from 23%-86% compared to 5%-22% in women with no known HPV-related pathology [13].
Currently, there are no definitive screening guidelines or a welldefined standard of care for people with high-grade anal cytology or AIN, regardless of HIV seropositivity [14-16]. Routine screening is not supported by the Centers for Disease Control and Prevention (CDC), United States Preventive Services Task Force (USPSTF), American Cancer Society (ACS), or the Infectious Diseases Society of America (IDSA) [17]. Although not proven in formal randomized control trials as done for cervical cancer, anal cancer may be preventable through anal-rectal cytology screening and treatment before progression to invasive squamous cell carcinoma occurs [2,5,15-22]. According to the ACS, “People at increased risk for anal intraepithelial neoplasia and cancer may benefit from screening …including women who have had cervical cancer or vulvar cancer” [2]. Several studies have found that high-risk cervical HPV is associated with high-risk anal HPV and abnormal anal cytology [16,21]. Anal cancer precursors are detectable by anal cytology, anal HPV testing, High-Resolution Anoscopy (HRA), and anal histology [2,3]. The Anal Cancer HSIL Outcomes Research Study (ANCHOR) is one study that is seeking to determine if treating anal high-grade squamous intraepithelial lesions (HSIL) in HIVinfected individuals can prevent the development of anal cancer [22].
Studies on anal dysplasia in HIV-negative women are extremely limited [2,9,15]. Most studies focus on women known to be at increased risk of anal cancer, including those with HIV infection or other forms of immunosuppression [2,10,11,13,22,23]. Our objective in the current study is to examine the relationship between anogenital abnormalities and the development of anal dysplasia among HIV-negative women enrolled in one of the largest commercial insurance programs in the US.
Study design and data source
This retrospective, matched case-control (1:3) study used 2009-2014 medical claims from the Clinformatics Data Mart (CDM) Database (OptumInsight, Eden Prairie, Minnesota, USA). This database contains member files including enrollment and demographic information, insurance claims for medical services, and prescriptions for over 56 million enrollees in the US. According to CDM, the database primarily consists of enrollees from the South (44%) and Midwest (26%), with the remaining population from the Northeast (11%) and West (19%). Since this study was a secondary data analysis using de-identified data, it was determined to be exempt by the Institutional Review Board at the University of Texas Medical Branch at Galveston. Figure 1 provides a detailed flowchart of the selection of cases and controls.
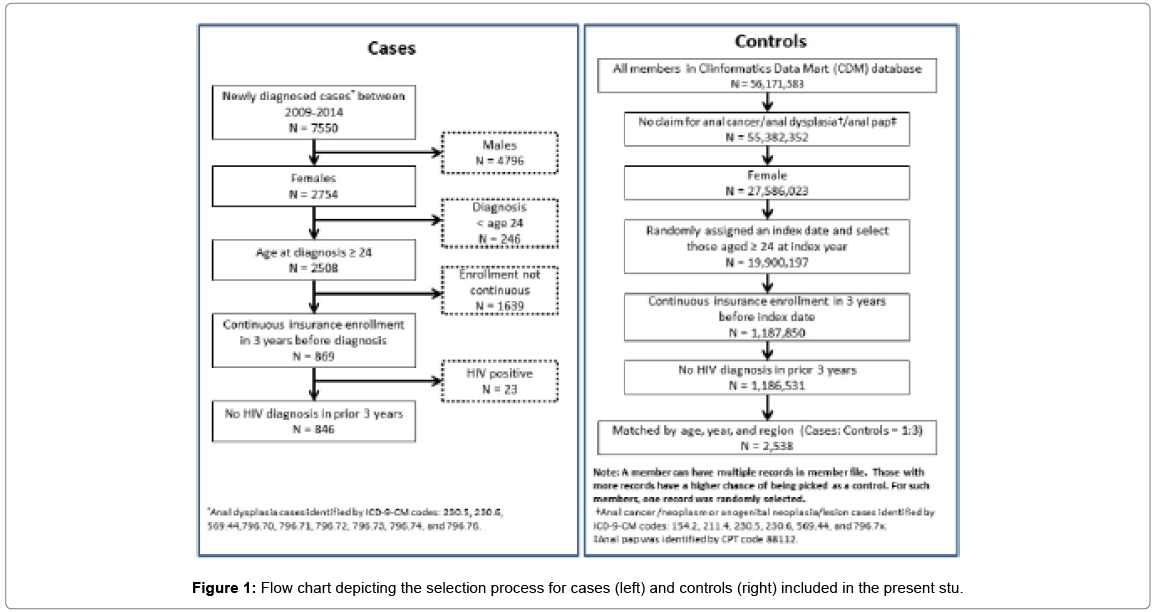
Figure 1: Flow chart depicting the selection process for cases (left) and controls (right) included in the present stu.
Cases
A total of 2,754 females were newly diagnosed with anogenital abnormalities or anal dysplasia between January 1, 2009, and December 31, 2014. Cases were selected according to the International Classification of Diseases, Ninth Revision, using Clinical Modification (ICD-9-CM) codes for carcinoma in situ of the anal canal or anus unspecified (230.5, 230.6), AIN 1 and 2 (569.44), abnormal glandular Papanicolaou (Pap) smear of anus (796.70), or Pap smears of the anus with atypical squamous cells (796.71, 796.72), squamous intraepithelial lesions (796.73, 796.74), or with cytological evidence of malignancy (796.76). Women had to be at least 24 years old at diagnosis (n=2,508). We selected those with continuous enrollment including the prior 3 years (n=869) and excluded those with HIV diagnoses in the prior 3 years, resulting in 864 cases. The initial diagnosis date served as the event date.
Matched controls
To identify matched controls, we excluded enrollees who had claims for anal neoplasms (ICD-9-CM codes: malignant neoplasm of the anal canal, 154.2; malignant neoplasm of the anus, unspecified site, 154.3; benign neoplasm of the rectum and anal canal, 211.4; and carcinoma in situ of the anal canal or anus unspecified, 230.5 and 230.6), anal neoplasia/lesions (ICD-9-CM codes: AIN1 and AIN2, 569.44), abnormal Pap smear of the anus (ICD-9-CM: 796.7x), or anal Pap smear (Current Procedural Terminology (CPT) code, 88112). For each of the controls, we randomly assigned an index month and year based on the year and month distribution of the event date among cases. We assigned the 15th of the month as the index date. We included females who were at least 24 years old, had continuous insurance enrollment over the prior 3 years, and had no documented HIV diagnosis in the prior 3 years. We identified 1,186,531 possible controls. Of these, we randomly selected 2,538 to match the cases based on age, event/index year, and region.
Measures
Age, gender, and region were obtained from the member files. Using claims for medical services in the 3 years before the event/index date, we identified whether cases and controls had HPV vaccinations (CPT codes: 90649, 90650), a history of smoking (ICD-9-CM codes: V15.82, 305.1), cervical cytopathology (by Pap test) (ICD-9-CM code: 91.46; CPT codes: 88141-88143, 84147-88148, 88150-88155, 88164- 88167, 88174-88175; Healthcare Common Procedure Coding System (HCPCS) codes: G0123-G0124, G0141-G0148, P3000-P3001, Q0091), or anogenital warts (ICD-9-CM: 078.11). Receipt of Pap smear was used as a proxy for preventive health services behavior. Research has shown that preventive health services significantly reduce morbidity and mortality [24]. Cervical histopathology was classified as cervical intraepithelial neoplasia (CIN1, CIN2, or CIN3) and was determined using the claim closest to the event/index date. When more than one diagnosis code was present on the same date, the code for the more severe condition was assigned.
Data analysis
All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC). We computed the number and proportion of patients with each of the aforementioned characteristics. To examine which characteristics were associated with anal dysplasia, we performed a multivariate conditional logistic regression to estimate odds ratios (ORs) and 95% confidence intervals for all studied characteristics. All analyses used an α level for statistical significance of 0.05 (2-tailed). Group differences were analyzed using Student t test, or the x2 test where appropriate.
A total of 3,384 privately insured HIV-negative women (846 cases and 2,538 controls) were included in this study. Table 1 shows the characteristics of the cases and controls. The mean age for both cases and controls was 50.1 ± 11.9 years (Interquartile Range [IQR]: 42-59 years). A higher proportion of the cases had a Pap test in the prior 3 years than did controls (79.9% versus 62.9%, respectively). Both groups had a low percentage of receiving the HPV vaccine in the prior 3 years. Compared to controls, a higher percentage of cases were smokers or had anogenital warts in the prior 3 years. More than half of the anal dysplasia cases (n=442, 52.2%) were diagnosed through anal histology (AIN1, AIN2, and AIN3). The rest of the cases were diagnosed through an abnormal cytological smear of the anus. About 14% of the cases (118/846) had cervical dysplasia (CIN1, CIN2, CIN3, and unspecified cervical dysplasia).
| Characteristics | Cases (n=846) | Controls (n=2,538) |
|---|---|---|
| N(%) | N(%) | |
| Age, years | ||
| Mean age ±SD (interquartile range) 50.1±11.9 (42.0-59.0) | ||
| 24-34 | 106 (12.5) | 318 (12.5) |
| 35-44 | 148 (17.5) | 444 (17.5) |
| 45-54 | 260 (30.7) | 780 (30.7) |
| 55-64 | 257 (30.4) | 771 (30.4) |
| ≥ 65 | 75 (8.9) | 225 (8.9) |
| Region | ||
| Midwest | 214 (25.3) | 642 (25.3) |
| Northeast | 91 (10.8) | 273 (10.8) |
| South | 391 (46.2) | 1173 (46.2) |
| West | 150 (17.7) | 450 (17.7) |
| Anal dysplasia* | ||
| AIN1/AIN2 | 213 (25.2) | - |
| AIN3 | 229 (27.1) | - |
| Abnormal cytologic smear of anus | 404 (47.7) | - |
| Year of anal dysplasia diagnosis | ||
| 2009 | 134 (15.8) | - |
| 2010 | 138 (16.3) | - |
| 2011 | 161 (19.0) | - |
| 2012 | 145 (17.1) | - |
| 2013 | 141 (16.7) | - |
| 2014 | 127 (15.0) | - |
| Health history prior three years | ||
| Received HPV vaccine | 11 (1.3) | 17 (0.7) |
| Smoking | 140 (16.5) | 183 (7.2) |
| Had pap test | 676 (79.9) | 1596 (62.9) |
| Had anogenital warts | 78 (9.2) | 13 (0.5) |
| Cervical dysplasia† | ||
| CIN1 | 59 (7.0) | 23 (0.9) |
| CIN2 | 10 (1.2) | 11 (0.4) |
| CIN3 | 20 (2.4) | 4 (0.2) |
| Unspecified cervical dysplasia | 29 (3.4) | 14 (0.6) |
| None | 728 (86.1) | 2486 (98.0) |
Note: Cases and controls were matched on age, event/index year, and region. AIN=Anal intraepithelial neoplasia; CIN=Cervical intraepithelial neoplasia; SD=Standard deviation. *When more than one diagnosis code was present on the same date, the more severe condition was assigned. When both histopathlogy and cytology codes were present, the former was assigned. †Determined by claim closest to the index date. When more than one diagnosis code was present on the same date, the more severe condition was assigned.
Table 1: Characteristics of cases with anal dysplasia and matched controls (n=3,384), 2009-2014 Clinformatics Data Mart Database.
Table 2 provides the results of the conditional logistic regression for the odds ratios for anal dysplasia diagnosis among privately insured HIV-negative women. The odds ratios for anal dysplasia increased for those who smoked, had a Pap test (regardless of outcome), or had a diagnosis of anogenital warts or cervical dysplasia in the past 3 years. The odds of being a smoker in the prior 3 years for HIV-negative women with anal dysplasia were 150% higher than for women without anal dysplasia. The odds of having cervical dysplasia were higher for HIV-negative women with anal dysplasia than for those without anal dysplasia, with odds ratios ranging from 2.6 to 11.8. HIV-negative women with anal dysplasia had higher odds of having HPV-related anogenital warts than did those without anal dysplasia (OR=16.3, 95% CI=8.7-30.7).
| Patient Characteristics | Adjusted Odds Ratio (95%CI) |
|---|---|
| HPV vaccine in prior three years | 1.73 (0.68, 4.43) |
| Smoking in prior three years | 2.54 (1.96, 3.30) |
| Had Pap test in prior three years | 2.25 (1.83, 2.78) |
| Had anogenital warts in prior three years | 16.32 (8.67, 30.73) |
| CIN 2 | 2.63 (1.05, 6.59) |
| CIN 1 | 6.37 (3.76, 10.78) |
| Unspecified cervical dysplasia | 6.17 (3.17, 12.03) |
| None | Reference |
Note: Cases and controls were matched on age, event/index year, and region. CI=Confidence interval; CIN=Cervical intraepithelial neoplasia.
Table 2: Odds ratios and 95% confidence intervals of anal dysplasia diagnosis among privately insured HIV-negative women.
To our knowledge, this is one of the few studies to explore risk factors associated with anal dysplasia among HIV-negative women. Specifically, we assessed the history of other HPV-related cancers (i.e., cervical, vulvar, and vaginal cancer), preventive health service behavior (i.e., HPV vaccine, Pap smear), and smoking status in the prior 3 years. Our study shows that HIV-negative women diagnosed with anal dysplasia are more likely to have HPV-related anogenital tract abnormalities-particularly anogenital warts or cervical dysplasia (CIN1, CIN2, or CIN3)-and a history of smoking. More than half of the cases were diagnosed using anal cytology, and 14% had cervical dysplasia in the prior 3 years.
This study complements previous studies that have shown a link between cervical cancer, anal cancer, and high-risk HPV [9,13,15,16,21,25,26]. However, only a few studies have addressed the role of screening for women with high-risk cervical and anal abnormalities, particularly those without a history of HIV [13,15,21]. The prevalence of anal high-risk HPV is higher in HIV-negative women with HPV-related pathologies than in those without HPV-related pathologies [13]. Robison et al. [15] found that HIV-negative women with a history of neoplasia in the lower genital tract are more likely to have positive anal cytology, anal high-risk HPV, and AIN. High-risk HPV in the anal canal was detected in 20.8% of the high-risk group compared to 1.2% of the low-risk group [15]. In a prospective study of HIV-negative women by Lammé et al. [21], high-risk cervical HPV was associated with high-risk anal HPV (OR=3.6, 95% CI=1.2-10.8) and abnormal anal cytology (OR=6.5, 95% CI=2.7-15.6).
Our study had a number of limitations. First, it may not be representative of the general population. The study included commercially insured women. Such women may be healthier, have a higher income, and have better healthcare access. More than half of the study population lived in the Southern United States. Therefore, these results must be interpreted accordingly.
Second, we were limited to what is collected in the CDM database to address our research questions. The data contain claims that are collected for payment purposes, not research. Information related to other risk factors, such as race/ethnicity, sexual activity/history, and socio-economic status were not available for study [8]. Research has shown that certain types of sexual behavior increase the risk of genital HPV infection and anal cancer, such as having sex at an early age, having multiple sexual partners, sexual orientation, and participating in receptive anal intercourse [8,27].
Last, claims included in this study were identified by ICD-9- CM, CPT, and HCPCS codes. Studies using administration data are prone to coding error. HIV status was determined by the presence of a HIV-positive claim, not cluster of differentiation 4 (CD4) count or lab confirmation of HIV status. As a result, we may have cases of undiagnosed HIV in women since anal HPV-associated conditions are more common in HIV-positive populations. The procedure used to identify anal dysplasia is not specific. While anal cytology is approximately as sensitive as cervical cytology, high-resolution anoscopy provides a more specific means of identifying AIN. However, this was not studied.
Despite these limitations, this study uses a large set of administrative data to provide unique insights into the possible risk factors for anal dysplasia for HIV-negative women, an understudied population in this regard. Our study is novel because it is one of the largest to date and includes women with a history of cervical, vulvar, and vaginal dysplasia and cancer. The results of this study indicate that HIV-negative women are at risk of developing anal dysplasia if they smoke and have HPVrelated cervical dysplasia and anogenital warts. As mentioned above, this is consistent with other studies on lower genital tract infections. However, many questions remain unanswered.
Future prospective studies are needed to evaluate the association between anal dysplasia and anal cancer among HIV-negative women who present with anogenital warts or cervical dysplasia. AIN is a precursor to anal cancer. It is possible that some of the AIN may progress into anal cancer. Gaining a better understanding of the natural history of anal HPV infection, precancerous lesions, risk factors, diagnostic tools, and therapeutic methods will provide us with better tools with which to adequately prevent, screen, evaluate, treat, and counsel patients on anal dysplasia [4].
The incidence of anal cancer is increasing. Careful consideration should be given to whether screening for anal dysplasia should be recommended for HIV-negative women who present with anogenital warts or CIN. Although routine anal cancer screening with anal cytology is not now recommended or endorsed [17], these women are at higher risk of developing anal cancer. Hence, more effective screening is needed. Although a prospective clinical trial studying the efficacy of anal dysplasia screening among HIV-negative women with HPV-related disease of the anogenital tract would provide the best evidence of whether we need to screen for anal dysplasia, no such trials are currently available [28]. The Anal Cancer HSIL (Highgrade Squamous Intraepithelial Lesion) Outcomes Research Study (ANCHOR) [22] is the only study that has assessed whether treatment for anal HSIL is effective in reducing the development of anal cancer in HIV-infected men and women compared to active monitoring. This type of study has not been replicated for the HIV-negative population. Observational studies using administrative data are the only current source of information for studying anal dysplasia among HIV-negative women. Future research should be planned with the goal of improving health outcomes for these women.
We thank Dr. David Konkel and Goldie Tabor for editing the manuscript. The research reported in this publication was supported by the Institute for Translational Sciences at the University of Texas Medical Branch. AMR is supported in part by a Clinical and Translational Science Award (Grant No. UL1TR001439) from the National Center for Advancing Translational Sciences, National Institutes of Health. The funding organization had no role in the design or conduct of the study; in the collection, analysis, or interpretation of data; or in the preparation, review, or approval of the article. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
The research reported in this publication was supported by the Institute for Translational Sciences at the University of Texas Medical Branch. AMR is supported in part by a Clinical and Translational Science Award (Grant No. UL1TR001439) from the National Center for Advancing Translational Sciences, National Institutes of Health. The funding organization had no role in the design or conduct of the study; in the collection, analysis, or interpretation of data; or in the preparation, review, or approval of the article. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.