Journal of Cell Science & Therapy
Open Access
ISSN: 2157-7013
ISSN: 2157-7013
Review Article - (2018) Volume 9, Issue 2
Nerve trauma is a common cause of quality of life decline, especially in young people. Causing a high impact in personal, psychological and economic issues. The peripheral nerve injury (PNI) with a several grade of axonotmesis and neurotmesis represents a real challenge for neurosurgeons. However, the basic science has greatly contribute to axonal degeneration and regeneration knowledge, making possible to implement in new protocols with molecular and cellular techniques for improve nerve re-growth and to restore motor and sensitive function. The Schwann cell transplantation from different stem cells origins is one of the potential tools for new therapies. In this briefly review is included the recent results of animal and human neurosurgery protocols of Schwann cells transplantation for nerve recovery after a PNI.
Keywords: Schwann cells; Neurotrauma; Peripheral nerve injury; Cell therapy
With an annual incidence of approximating 13 to 23 per 100,000 persons per year [1] the Peripheral Nerve Injuries (PNI), have a great impact in the people’s quality of life. The expected recovery from this injuries depends on critical factors as the type of injury, the patient`s age and the delay before intervention [2]. However, it`s well known that after a PNI the peripheral nervous system (PNS) has an innate capacity to regenerate but is often insufficient and functional recovery is incomplete [3].
In 1943, Seddon introduced a classification system to describe nerve injury [4] that included neurapraxia, axonotmesis, and neurotmesis [5]. A few years later, Sunderland expanded the axonotmesis grade into three different levels, for a total of five grades [6]. In general, the several axonotmesis injuries and neurotmesis requires complicated microsurgery techniques to restore nerve continuity and functional recovery.
Nerve transfer and nerve grafting are some of most helpful techniques for PNI repair. This procedure have been enhanced with cellular and molecular protocols. The combination of neurosurgery interventions and transplanted Schwann cells improves an auspicious support for peripheral nerve repair and has been investigated in preclinical and clinical studies as a strategy to circumvent the limitations of surgical repair [7].
In this briefly review is included the recent results of animal and human neurosurgery protocols of Schwann cells transplantation for nerve recovery after a PNI.
Sources of Schwann cells
Schwann cells are embryologically derived from the neural crest [8]. The capacity of Schwann cells for proliferation, growth factor secretion, immune modulation, remyelination and migration make them potential targets in neural repair [9]. Some of the sources of Schwann cells are a population of neural crest pluripotent and stem cells (NCSCs) in sciatic nerve and dorsal root ganglia (DRG), the NCSCs placed in a specified differentiation medium and the most favorable nanofiber matrix [10] are influenced to convert into a Schwann cell lineage.
Mesenchymal stromal cells (MSCs) or bone marrow stromal cells are multipotent somatic stem cells, from a non-hematopoietic precursor found in the bone marrow capable to differentiate into neural cell types including Schwann-like cells [11]. In vitro using an indirect co-culture system, the DRG cells extend their neurites significantly higher when they are expose to differentiate MSCs (dMSCs) compared to undifferentiated MSCs (uMSCs) [12] and in animal models the transplantation of this Schwann-like cells derived from MCSs were able to differentiate into myelinating cells, capable of supporting nerve fibre re-growth and functional recovery after nerve injury [13].
Besides bone marrow stromal cells and NCSCs, skin, adipose, and olfactory tissues provide other potential cell sources [14]. The skin precursor cells SKPCs that can differentiate into neural crest cell types that display similar features to Schwann cells and peripheral neurons [15]. After peripheral and spinal cord injury the SKPCs provided a bridge across the lesion site, increased the size of the spared tissue rim, myelinated spared axons within the tissue rim, reduced reactive gliosis, and an environment that was highly conducive to axonal growth making possible to enhance the locomotor activity [16].
The differentiated adipose-derived Schwann cells expressed a range of intrinsic neurotrophic factors [17]. The addition of this cells to the site of repair promote a neuroprotective effect evidenced by the expression of anti-apoptotic m-RNA of Bcl-2 in the dorsal root ganglia.
Other studies showed that adipose-derived Schwann cells enhanced regeneration distance in a similar manner to differentiated bone marrow mesenchymal stem cells without limitations of the donor-site morbidity associated with isolation of Schwann cells [18].
Finally, the induced pluripotent stem cells (iPSCs) since their discovery in 2006 [19] have been propose as a new tool for cell replacement therapy in nerve injury. NCSCs derived from iPSCs can be immune compatible with a potential expansion of this cells, making them a better source for the regeneration of peripheral nerve [20]. However, aberrant differentiation into unwanted lineages, might complicate their therapeutic utility.
In summary the three-principal mechanism of action in stem cell transplantation is represented in Figure 1. Their potential depends basically in differentiate into Schwann-like cells, increase neurotrophic production and myelin formation [21].
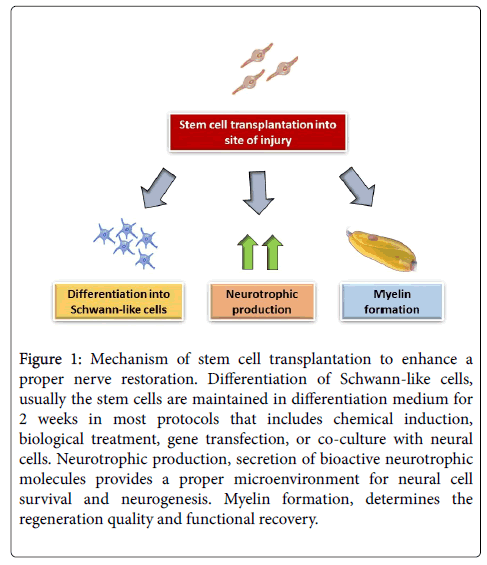
Figure 1: Mechanism of stem cell transplantation to enhance a proper nerve restoration. Differentiation of Schwann-like cells, usually the stem cells are maintained in differentiation medium for 2 weeks in most protocols that includes chemical induction, biological treatment, gene transfection, or co-culture with neural cells. Neurotrophic production, secretion of bioactive neurotrophic molecules provides a proper microenvironment for neural cell survival and neurogenesis. Myelin formation, determines the regeneration quality and functional recovery.
Schwann cells transplantation after PNI in humans
The mechanisms of traumatic nerve degeneration depend on the underlying trauma, but eventually with severe enough injuries Wallerian degeneration ensues [22]. Schwann cells provide bioactive substrates on which axons migrate and have been shown to release factors that regulate axonal outgrowth [23]. Recently, clinical protocols of neurosurgery interventions with Schwann cells transplantation have been applied.
The steps to produce a safety protocol to apply in humans combined a large list of researches that include: the isolation of the SCs from adult, human nerve tissue [24], the ability to induce division and growth of the cells once isolated with the use of particular mitogens (heregulin b1/forskolin), and confirming the safety of these cells and making sure that they did not produce tumorous growths in vivo [25].
In 2017, the first human experience of Schwann cells transplantation for sciatic nerve restore [26]. The study evidence that autologous Schwann cells may be a viable option for long-gap nerve defect repairs. Both patients respond correctly with an improvement in their motor and sensitive function. This preliminary results shows the potential use of the cell therapy for improve patient’s quality of life after neurotrauma. In Figure 2 is represented the schematic protocol for future neurosurgery interventions with microsurgery combined with Schwann cell transplantation.
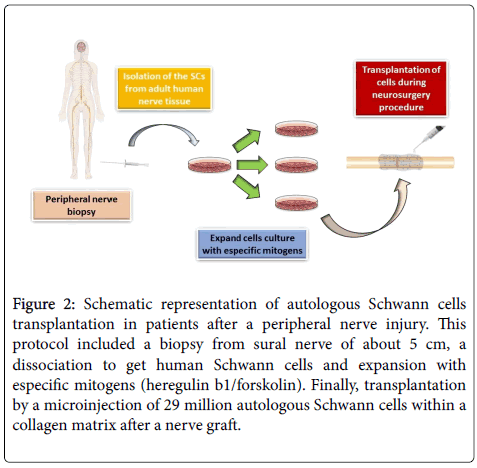
Figure 2: Schematic representation of autologous Schwann cells transplantation in patients after a peripheral nerve injury. This protocol included a biopsy from sural nerve of about 5 cm, a dissociation to get human Schwann cells and expansion with especific mitogens (heregulin b1/forskolin). Finally, transplantation by a microinjection of 29 million autologous Schwann cells within a collagen matrix after a nerve graft.
Future trends and challenges
One of the main challenges in this topic is to minimize the nonfunctional and erroneous connections [27]. A combination of slow axonal regeneration, structural changes in muscle targets, and an increasingly less supportive stromal environment for regeneration all contribute to incomplete functional recovery [28]. So, we need to take some considerations in future protocols for treat patients with acute, severe and long length peripheral nerve injuries. The autologous transplantation of SC is the gold standard, they enhance the regeneration process through their secretion of neurotrophic and tropic cues however, in the clinical practice with certain patients it may not result very convenient for the several weeks that takes to culture a reasonable amount of SC. In the other hand, the allogenic SC transplantation could be culture very fast but this protocol should include immunosuppression treatments. Carrying to possibility to infections and side effects. Moreover, there etAhical commitments on this topic haven´t been totally discussed.
Another dimension on this topic is in the engineering process, nerve conduits need to be a perfect scaffolds with enough permeability to provide sufficient diffusion of oxygen and metabolites for supporting Schwann cells proliferation but should also prevent fibroblast infiltration [29]. In this context, the main considerations for approach new protocols should consider, an early and appropriate diagnose of nerve injury, including a mechanism of injury and length of nerve defect. If a patient is candidate to a SC transplant, then we should consider which kind of transplant will bring better outcomes, the autologous or the allogenic with the pros and cons mentioned. Furthermore, in future clinical trials are also needed to standardize rehabilitation strategies in order to restore nerve function after injury [30].
The implementation of cell therapy protocols like the Schwann cells or Schwann-like cells transplantation represents a potential tool to improve the quality of life of patients with peripheral nerve injuries after a neurotrauma. However, there`s still a need for more clinical trials with different origins of Schwann-like cells and neurosurgery techniques to identify the proper protocols for distinct kinds of nerve injuries and patients.