Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Case Report - (2016) Volume 6, Issue 4
Congenital diaphragmatic hernia (CDH), which usually induces pulmonary symptoms, is more diagnosed in infant than in adult. Right-side hernia is rarer because the right pleuroperitoneal canal closes earlier and the liver buttresses the right diaphragm. We report an unusual case of a right-sided congenital diaphragmatic hernia complicating with secondary common bile duct stones in a 43-year-old man.
<Keywords: Gallbladder; Jaundice; Colon; Pancreas
A 43-year-old man admitted into our hospital in July 11 2010 presented with a 2-day history of right upper quadrant intense pain associated with nausea, vomiting and followed by 5-day yellow coloration of skin. The patient was diagnosed with gallstones a few years ago, but he denied a history of chest or right upper abdomen trauma. His examination was nothing besides yellow coloration of skin and sclera. The results of laboratory analysis shown that GGT 204 IU/L (reference range: 0-50 IU/L), Total bilirubin (TBiL) 251.4 umol/L (reference range: 2-22 umol/L), Direct bilirubin (DBiL) 226.7 umol/L (reference range: 0-7 umol/L). At first, he was diagnosed just as obstructive jaundice. However, other problems were found during the typical preoperative preparation. The chest X-ray revealed the right-side diaphragm was elevated markedly (Figure 1). The initial and contrast-enhanced CT image revealed calculus of common bile duct and the right-lobe of liver, gallbladder and colon herniated into the thorax cavity (Figures 2A and 2B), the latter was confirmed by barium enema (Figure 3). According to the clinical manifestation and auxiliary examinations as above, the patient was diagnosed with choledocholithiasis, congenital right side diaphragmatic hernia.
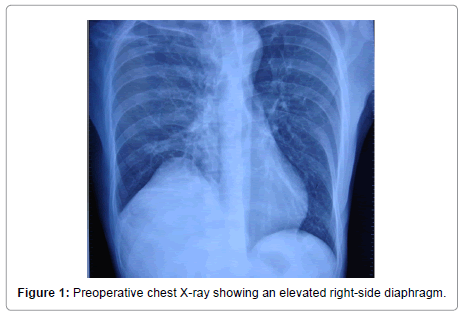
Figure 1: Preoperative chest X-ray showing an elevated right-side diaphragm.
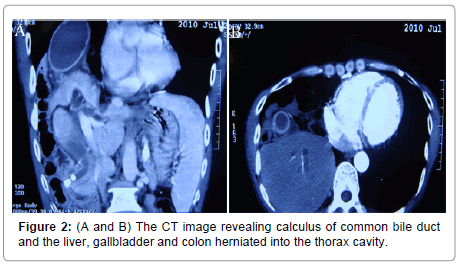
Figure 2: (A and B) The CT image revealing calculus of common bile duct and the liver, gallbladder and colon herniated into the thorax cavity.
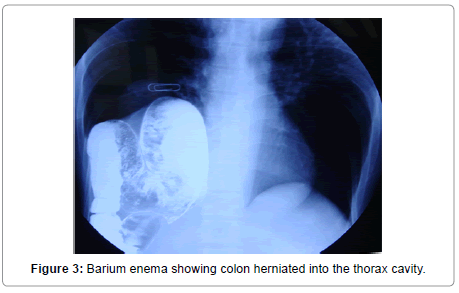
Figure 3: Barium enema showing colon herniated into the thorax cavity.
The patient underwent an elective thoracoabdominal operation. During the operation, that the right-lobe of liver associated with gallbladder and colon herniated into the right thoracic cavity through a 12*8 cm defect at the central tendinous part of the diaphragm was confirmed (Figure 4). The herniated portion of the liver and colon was moved back to the abdominal cavity and a non-absorbable patch was sutured under the diaphragm to repair the defect. The gallbladder with thick-wall and dilated cystic duct was excised and the common bile duct calculus was removed. The bile duct mucous membrane was adhered by floccule which was caused by the infection of pseudomonas aeruginosa through bacterial culture of bile after operation.
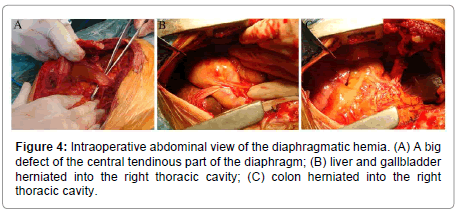
Figure 4: Intraoperative abdominal view of the diaphragmatic hemia. (A) A big defect of the central tendinous part of the diaphragm; (B) liver and gallbladder herniated into the right thoracic cavity; (C) colon herniated into the right thoracic cavity.
The patient remained stable during the intraoperative phase. Postoperative recovery was uneventful except jaundice descended slowly. Finally, the patient was discharged 12 days after the surgical procedure with total bilirubin 149.8 umol/L, direct bilirubin 111.3 umol/L. Postoperative CT scan showed the liver of the patient had been moved back into the abdominal cavity (Figure 5A). Cholangiography found no calculus in bile ducts (Figure 5B). At follow-up, he had no symptoms and his TBiL and DBiL were down to normal level in 2 months.
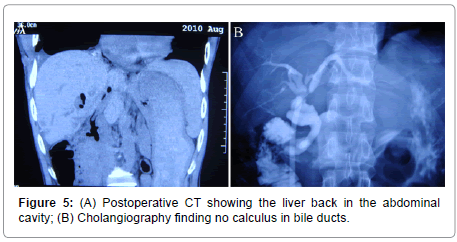
Figure 5: (A) Postoperative CT showing the liver back in the abdominal cavity; (B) Cholangiography finding no calculus in bile ducts.
Congenital diaphragmatic hernia is believed to be caused by the failure diaphragmatic closure at the 9 to 12 week of pregnancy. It has an incidence of 1:3000–1:5000 per live births [1]. Most CDH can be diagnosed in children for which almost presented as acute pulmonary symptoms [2]. Different from infants with these hernias may have acute presentation, most adults present with more chronic symptoms, such as chronic dyspnea, chest pain and pleural effusion. Recurrent abdominal pain, postprandial fullness and vomiting are the most common abdominal symptoms in adults [3].
Clinically, the left-sided congenital diaphragmatic hernia is more common than right-sided. The population-based data from ongoing studies in the California Birth Defects Monitoring Program (CBDMP), Anne M. Slavotinek compared 146 CDH cases, 38 with R-CDH (26%) and 108 with L-CDH (74%) [4]. In addition, the majority of herniated organs at left are the omentum, bowel, spleen, stomach, kidney, and pancreas. Because of the right side of the pleuroperitoneal canal closing earlier, liver as the herniated organs is extremely rare [5].
Chest X-ray and CT are essential for definitive diagnosis of CDH, especially for an adult patient with vague and nonspecific clinical symptoms. The diagnosis in our patient was ascertained by a combination of chest X-ray and CT. Chest roentgenograms may show the defective diaphragm as a sharp line in the thorax and the enema with contrast fluid may reveal a stop at the entrapped part of the intestine [2]. Only colonic contrasting may lead to the correct diagnosis as in our patient. It has been reported that the multi detector row CT scan with coronal, sagittal and 3-dimensional reconstructions raises the CT’s sensitivity to CDH [6]. The multi detector row CT scan in our case revealed huge right-sided hernia of large gut, the right-lobe of liver and gallbladder in pleural cavity.
Hernia repair is typically performed through either trans abdominal or transthoracic, or both [7]. However, laparoscopic surgery, thoracoscopy, or artificial patches have become very popular in recent years. Right-sided defects are traditionally dealt with by a thoracic or thoracoabdominal approach because of the presence of the liver. Small diaphragmatic defects are usually repaired by primary repair with nonabsorbable sutures [8]. For large defects, prosthetic patches or tissueengineered grafts are typically used to avoid causing excessive tension after repair [1]. In our patient the size of the defect in the diaphragm was 12*8 cm wide, and sutured with non-absorbable patch.
Prolapse of the gallbladder into the thoracic cavity in posttraumatic diaphragmatic hernia was reported in few articles [9-13]. An inflamed gall bladder (with stones) in the thoracic cavity was rare [14]. Malrotation of hepatic right lobe in our patient, which was confirmed by operation, may impair bile flow of microscopic bile duct and induce cholestasis, resulting in calculi formation in gallbladder for a long term. The gallbladder contracts to discharge stone into the common bile duct. In summary, high attention should pay to some atypical thoracic or abdominal symptoms in clinics, appropriate auxiliary examinations contribute to accurate diagnosis.