Family Medicine & Medical Science Research
Open Access
ISSN: 2327-4972
![]() +44-77-2385-9429
+44-77-2385-9429
ISSN: 2327-4972
![]() +44-77-2385-9429
+44-77-2385-9429
Research Article - (2013) Volume 2, Issue 3
Background: Sensitive skin, a phenomenon claimed by the majority of female consumers across the industrialized world, is not well understood. Multiple studies investigating the biology of reported discomfort have been unable to establish reliable diagnostic criteria. The influence of geographical and cultural influences, including health and beauty product advertising, on perceptions of sensitive skin are increasingly being recognized.
Objective: To evaluate southern American women for the perception of sensitive skin and compare to results of previous surveys in other regions of the US.
Patients/Materials/Methods: A written questionnaire for self-reported perception of facial, genital, and body skin sensitivity was administered to 86 females in Mississippi (MS). Statistical analysis was performed on the data and compared with previous results.
Results: Women in Mississippi reported any skin sensitivity at significantly higher rater than those in Ohio although they reported very or moderately sensitive skin at rates lower than other regions of the US.
Conclusions: This study confirms previous studies that have shown that women across the industrialized world report some degree of skin sensitivity at fairly high levels and that environmental factors such as weather can contribute to the perception of sensitive skin. It is increasingly recognized that psychosocial influences as well as biological factors can contribute to skin sensitivity. Cultural contributions to the perception of skin sensitivity, particularly in women, are often ignored but should be considered as a likely component of sensitive skin perceptions.
<Despite thorough premarket testing of health and beauty products specifically designed to ensure that marketed products do not irritate the skin, individual response is difficult to predict. In routine postmarket surveillance, a small number of consumers consistently report unanticipated adverse reactions to extensively tested products, typically itching or pain described variously as burning, stinging, or prickling [1]. Cleaning products as well as many environmental irritants (e.g., weather conditions) are also reported to cause similar reactions. This unusual sensitivity to common products or exposures has been termed “sensitive skin.”
Research efforts to uncover the biological source of this reported hypersensitivity to common products continue. Confounding significant progress are the prodigious number of different signs and symptoms that patients report as well the multitude of triggers described. In addition, subjects who claim sensitive skin, in irritant testing, often produce no visible irritation, while subjects who deny sensitivity sometimes react strongly [2]. Furthermore, subjects who react strongly to a known irritant may lack sensitivity to another. Individual response, in fact, can differ substantially at different anatomical sites [3], and even at the same anatomical site on symmetric limbs [4]. Efforts to establish reliable diagnostic criteria and testing methods continue; however, epidemiological surveys which collect self-reported consumer perceptions of skin sensitivity remain a primary source of data.
Though consistent evidence for either a certain etiology or a dependable symptomatology for sensitive skin is lacking, epidemiological surveys reveal surprising agreement in one aspect of the sensitive skin phenomenon: although initially believed to be an unusual reaction to common products experienced by only a small subset of consumers, epidemiological surveys consistently find a surprisingly high prevalence of self-perceived sensitive skin across the industrialized world. Early epidemiological studies in Europe (Germany) [5], England [6], France [7], and the US [8] observed unanimously that a majority of women, when surveyed as to whether they or not they experienced sensitivity to common consumer products (despite premarket testing that found no irritant potential), reported unpleasant reactions to common consumer products. Men in early studies were less likely to report sensitive skin: 38.2% of men sensitive versus 51.4% in women in England [6], 41% versus 55% in Germany [5], 36% versus 51% in the US [8], and 44% versus 59% in France, respectively [9].
Not surprisingly, some researchers dismiss the high prevalence of sensitivity identified by epidemiological surveys, calling sensitive skin a “princess and the pea effect,” i.e., a largely psychosocial phenomenon in which sensitive skin has become culturally desirable [10].
Efforts to establish a physiological basis of sensitive skin perception have focused largely on the contribution of various intrinsic components of skin: gender [11], age [12], anatomical site [13-15], ethnicity [8,16,17], skin type [6,18], and concomitant dermatological diseases [19,20]. Lesser attention, however, has been paid to the wide variety of potential extrinsic components, including environmental exposures, lifestyle factors, and cultural influences.
Self-reported perceptions of sensitive skin have now been gathered from populations in four continents (Figure 1), with particular attention to population differences in Europe (Figure 2). The results of earlier epidemiological surveys have been repeatedly confirmed; the large majority of female consumers in the developed world believe themselves to have sensitive skin.
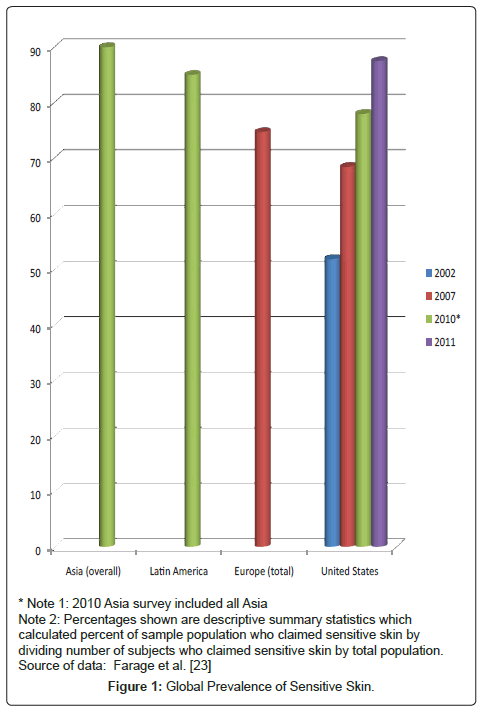
Figure 1: Global Prevalence of Sensitive Skin.
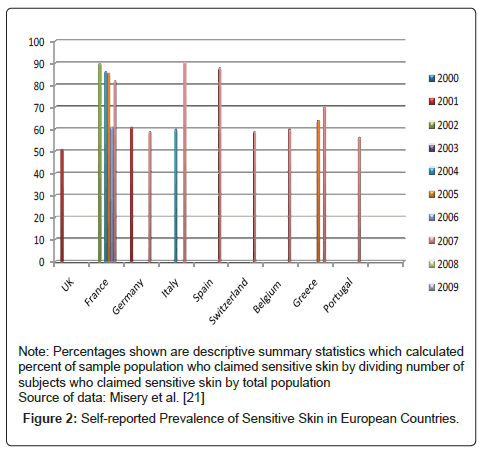
Figure 2: Self-reported Prevalence of Sensitive Skin in European Countries.
The availability of worldwide data allows comparison of subjects living in disparate geographies with different cultures and different exposures. Intriguingly, geographically specific differences in sensitive skin prevalence are observed. A comparison of self-reported skin sensitivity in eight European countries found dramatic differences between national populations that are biologically similar (Portugal, Italy, and Spain, for example, reporting 80% to 90% of their population as experiencing at least some sensitivity; while Germany, Belgium, and Switzerland reported just a little more than half (Figure 2)), an unexpected finding given that the area surveyed shares genetic similarity as well as geographic proximity [21]. A Chinese community-based study surveyed residents of Beijing, Shanghai, and Guangzhou in 9154 women and men aged 15 years or older and found a mean prevalence that varied dramatically between cities. The number of Chinese that claimed sensitive skin (very or moderately) was 17.12% in Beijing but barely more than half that (9.10% ) in Shanghai, yet substantially more (22.39%) in Guangzhou [22].
The observation that substantial differences in both the prevalence of skin sensitivity and its specific characteristics can sometimes occur in seemingly similar populations (or even in a single population), in conjunction with the ongoing lack of a solid biological explanation or reliable diagnostic criteria for sensitive skin, emphasizes the multifactorial nature of this complaint. Extrinsic factors like environmental or cultural influences are increasingly being explored.
The variety of possible irritants inherent in changing weather conditions is the most studied environmental cause of skin sensitivity. A French study which surveyed two populations of approximately a thousand people found that the self-reported prevalence of sensitive skin was significantly higher in July than in March (59.4% versus 52.1%, p=0.08), an indication that environmental exposures do impact sensitive-skin perceptions [18]. Extreme cold was reported as the most common culprit in skin sensitivity in a US study [16]; and when sensitive skin was evaluated in Beijing, Shanghai, and Guangzhou, the significant differences observed between three urban areas (P<0.001) were putatively attributed to different climactic conditions.
Separate investigations by the same author found that weather conditions accounted for 33% of sensitive skin reports in China; [23] and 35% of self-reported sensitive skin in the US [16]. In addition, sensitivity, to weather was climate-dependent: cold and hot weather caused skin irritation in 83.9% and 58.7%, respectively, of sensitive skin sufferers in the US [16], while in China hot weather caused more irritation (31.2%) than cold (19.2%) [23].
Differences in sensitive skin prevalence may also be related to lifestyle decisions that dramatically influence exposures to irritants. It is known, for example, that feminine hygiene and fertility products like perfumes, medications, antifungal medication, and contraceptives are the most common cause of vulvar irritation [24]. Older women, predictably, are more likely to report irritation due to incontinence products than younger women, who were more likely to report irritation due to tampons [12], a finding clearly based on the fact that women need different forms of protection at different stages of life. Asians reported being more sensitive than Caucasians to spicy food, also likely related to different levels of exposure [8]. Differences in sensitive skin prevalence, therefore, may have their origin more in culturally driven levels of exposure than on actual physiological differences.
The steady rise in self-reported skin sensitivity over the last decade, particularly the rapid rise among men, has prompted discussion regarding the role that other cultural influences may play in the perception of sensitive skin. Early studies (1998-2002) found that women were substantially more likely to claim sensitive skin than men. Since then, however, hundreds of sensitive skin products have been specifically targeted toward men; it has been suggested that these products, and the aggressive advertising associated with them, may have made it more culturally acceptable for men to claim sensitive skin [13]. A survey of American men performed in 2009, in fact, observed the perception of sensitive skin in men and women to be virtually equal [13]. A comparison of self-reported skin sensitivity in Europe, in which Spain was revealed to have almost double the self-reported prevalence of Portugal (despite being adjoining countries with very similar climates and biologically identical populations) attributed the observed differences in the prevalence of sensitive skin in Europe to differing levels of advertising [21]. A recent survey of sensitive skin in Chinese women (residents of a developing country with comparatively less aggressive advertising of products targeted for sensitive skin), would seem to support at least some cultural component. Overall, 41% of Chinese women claimed sensitive skin, far less than the 76% to 88% typically claimed in North America and Europe (with comparatively higher levels of health and beauty-product advertising) [23]; while percentages of Chinese-American women who claimed sensitive skin were not different than their Euro-American, African-American, or Hispanic neighbors [8].
Other potential cultural contributions exist as well. For example, cultures tolerate expressions of pain differently; some prize stoicism [25] while others encourage free expression of pain and emotion [26].
Although multiple laboratory studies have failed to document consistent ethnic differences in pain thresholds, pain studies do document a significant influence of culture on pain expression. African-American cancer patients reported more pain and as well as more pain-related dysfunction than white patients [27]; Asians were observed to be more stoic than whites [28]. The influence of cultural conventions regarding pain expression and their influence on sensitive skin perception is virtually unknown.
To our knowledge, no epidemiological surveys have comprehensively analyzed regional differences in sensitive skin in the United States. This article will compare previously collected information on the perception of sensitive skin among women in Cincinnati, OH with perceptions of sensitive skin among women in the states further south. These data will then be compared to that collected in other regions of the US in order to provide a full analysis of sensitive skin in the United States, particularly with regard to regional differences.
The survey utilized in this study to gather perceptions of sensitive skin among women in the southern United States was exactly the same questionnaire used in 2006 to evaluate sensitive skin prevalence and characteristics in subjects in the area of Cincinnati, OH, USA. The survey consisted of a written questionnaire which, in the Mississippi study, was administered in person to female staff of two schools (n=36), three medical practices (n=21), and members of one large church (n=32) in DeSoto County, Mississippi. In this study, all participants had been raised in the southern US states of Mississippi, Alabama, Arkansas, Louisiana, and Tennessee.
The survey collected demographic information as well as extensive information with regard to subject perceptions of their own skin sensitivity, including the degree of sensitivity (subjects were asked to rate their skin as “very,” “moderately,” “slightly,” or “not sensitive,”) the location of skin sensitivity (face, skin and/or body), the duration of perceived sensitivity, the course of skin sensitivity since its onset (skin much more sensitive now, somewhat more sensitive, about the same, somewhat less sensitive, or much less sensitive), and perceived triggers for skin sensitivity.
To allow comparison between Cincinnati and Mississippi results, the data from the 2006 survey with 1039 respondents (which also included Hispanic, Asian, and male subjects) was analyzed to include only the responses of Caucasian and African-Americans females (to match the ethnical demographics in the Mississippi study), resulting in a subset of 764 women.
Statistical analysis of quantitative data between groups was performed using Student’s T-test; analysis of qualitative variables was conducted by Fisher’s Exact tests. All analyses were performed with SAS software version 9.3) (SAS Institute, Raleigh, NC, USA.)
Data obtained was compared to previously published data which reported similar parameters of skin sensitivity from other areas of the US. The objective of this analysis was to provide a comprehensive assessment of the prevalence of sensitive skin in the US population, particularly with regard to the existence of significant regional differences.
Southern US as surveyed in DeSoto County, Mississippi
A total of 89 subjects in DeSoto County, MS, completed surveys. All were females between the ages of 20 and 74. Caucasian women made up 89.9% of the total population; 10.1% of the subjects were African- American. No Hispanic or Asian women were recruited.
Of the 89 southern women who completed the survey, 11.2% perceived their skin to be “very sensitive,” 31.5% perceived their skin to be “moderately sensitive,” 34.8% perceived their skin to be “slightly sensitive,” and 22.5% perceived their skin to be “not sensitive at all.”
Of those who claimed sensitive skin, no subjects reported that their skin sensitivity had begun in the last 6 months, 2.9% believed their skin sensitivity had developed in the last year, 21.7% less than 5 years, 26.1% less than 10 years, and 49.3% greater than 10 years. Most subjects (55.7%) reported that their skin sensitivity had worsened over time. The majority of subjects also reported family members who also had sensitive skin (53.4%) as well as intentionally choosing products labeled hypoallergenic or safe for sensitive skin (61.4%). Most subjects were living in rural areas; none were urban. Although the majority of those who claimed sensitive skin reported unpleasant dermatological or sensory reactions to common products, primarily health and beauty products or cleaning products, nearly half (46.6%) could not identify specific ingredients that prompted skin reactions.
Most subjects identified themselves as having sensitive skin due to burning, stinging, itching, or other negative sensory reactions to personal products (36.1%), although substantial numbers claimed sensitive skin due to experiencing rash or redness after use of personal products (27.9%) as well as skin sensitivity specifically to weather conditions (27.9%).
The most sensitive area of the body was reported by a substantial majority (79. 8%) to be the face; however, 74.2% of responders reporting body sensitivity as well. Genital skin, specifically, was also reported to be sensitive by most subjects (57.3%).
De Soto County, Mississippi as compared to Cincinnati, Ohio
The same survey was employed for both DeSoto County, Mississippi and Cincinnati, Ohio, and all surveys in both states were performed face-to-face; however, the Ohio survey analyzed data from 764 women, while the Mississippi survey analyzed data from only 89. In addition, the Ohio population was primarily suburban, while the Mississippi population was primarily rural. The Ohio population was also significantly younger than the Mississippi population, mean age 35.01 vs 45.49, respectively (p=0.0034).
Overall prevalence of skin sensitivity was analyzed, as well as sensitivity specific to facial skin, body skin, and genital skin; and the course and duration of skin sensitivity. Women in Mississippi were more likely to report higher overall skin sensitivity than women in Ohio, as well as higher sensitivity of facial and body skin (Table 1 and 2). Women in Mississippi were also more likely to report pronounced sensitivity of genital skin (Table 1).
| Degree of Sensitivity by Anatomical Area | Responses by Geographical Arean/N(%) | P value | Chi square Probabilityc | Phi Coefficientd | |
|---|---|---|---|---|---|
| MS | OH | ||||
| Skin overall –any sensitivity | 69/89 (77.5) | 527/764 (69.0) | -- | 0.0112 | 0.1141 |
| Skin overall is very sensitive | 10/89 (11.2) | 37/764 (4.8) | 0.0230 | -- | -- |
| Facial skin – any sensitivity | 71/89 (79.8) | 600/759 (79.1) | -- | 0.0119 | 0.1137 |
| Facial skin is "very sensitive" | 19/89 (21.3) | 87/759 (11.5) | 0.0110 | -- | -- |
| Body skin – any sensitivity | 66/89 (74.2) | 460/760 (60.5) | -- | <0.0001 | 0.1759 |
| Body skin is "very sensitive" | 8/89 (9.0) | 15/760 (2.0) | 0.0014 | -- | -- |
| Genital skin – any sensitivity | 51/89 (57.3) | 437/758 (57.7) | -- | 0.1625 | 0.0778 |
| Genital skin is "very sensitive" | 3/89 (3.4) | 74/758 (9.8) | 0.0500 | -- | -- |
Table 1: Subjects with Any Level of Self-Reported Sensitivitya or Very Sensitive Skin by Anatomical Area in Total Populationb (Mississippi versus Ohio).
| Degree of Sensitivity by Anatomical Area | Responses by Geographical Area n/N(%) | P value | |
|---|---|---|---|
| MS | OH | ||
| Skin overall is “slightly sensitive” | 31/69 (44.9) | 315/527 (59.8) | 0.0200 |
| Facial skin is "slightly sensitive" | 25/71 (35.2) | 321/600 (53.5) | 0.0038 |
| Body skin is "slightly sensitive" | 30/66 (45.5) | 306/460 (66.5) | 0.0015 |
| Genital skin is "slightly sensitive" | 30/51 (58.8) | 251/437 (57.4) | 0.8821 |
Table 2: Subjects with Self-Reported Slightly Sensitive Skin by Anatomical Area versus All Responsesa of Skin Sensitivity (Mississippi versus Ohio).
Women in the South and in the Midwest who claimed skin sensitivity, however, were equally likely to report previous diagnoses of skin allergies, family members who also had sensitive skin, or a preference for purchasing sensitive skin care products.
The respective significance of potential triggers for sensitive skin between the two regions was also analyzed, with a variety of personal care products, cleaning products, and other environmental triggers analyzed.
When asked to define skin sensitivity to environmental exposures such as weather conditions, stress, menstrual cycles ,and fabrics, women from the Cincinnati area and from the southern US had similar sensitivity to all environmental irritants with the exception of wind (southern women were significantly more likely to report skin sensitivity to wind than women from Cincinnati) (Table 3).
| Environmental Factors | Responses by Geographical Area n/N(%) | Chi square Probabilityc | Phi Coefficientd | |
|---|---|---|---|---|
| MS | OH | |||
| Cold weather | 76/85 (89.4) | 600/714 (84.0) | 0.3125 | 0.0668 |
| Hot weather | 37/75 (49.3) | 404/704 (57.4) | 0.5904 | 0.0496 |
| Dry weather | 64/82 (78.0) | 515/704 (73.2) | 0.7302 | 0.0406 |
| Humid weather | 26/71 (36.6) | 274/684 (40.1) | 0.7301 | 0.0414 |
| Wind | 67/81 (82.7) | 461/690 (66.8) | 0.0034 | 0.1331 |
| Sun | 58/80 (72.5) | 559/717 (78.0) | 0.1860 | 0.0777 |
| Stress | 55/80 (68.8) | 385/701 (54.9) | 0.0867 | 0.0918 |
| Menstrual cycle | 35/62 (56.5) | 359/674 (53.3) | 0.5164 | 0.0557 |
| Rough fabrics | 59/79 (74.7) | 434/703 (61.7) | 0.1522 | 0.0822 |
Table 3: Self-Reported Skin Sensitivity to environmental factors: Any levela of perceived sensitivity compared to all Respondersb.
When health and beauty products were evaluated southern women were significantly more likely to report skin sensitivity to moisturizers, facial cosmetics, eye cosmetics, and lotions than women from Ohio (Table 4). All other health and beauty products evoked similar sensitivity in the two populations.
| Health or Beauty Product | Responses by Geographical Area n/N (%) | Chi square Probabilityc | PhiCoefficientd | |
|---|---|---|---|---|
| MS | OH | |||
| Facial moisturizer | 52/85 (61.2) | 341/717 (47.6) | 0.0290 | 0.1061 |
| Facial cosmetics | 55/82 (67.1) | 321/693 (46.3) | 0.0025 | 0.1361 |
| Eye cosmetics | 42/78 (53.8) | 244/685 (35.6) | 0.0059 | 0.1279 |
| Soap (hand or body) | 59/85 (69.4) | 431/741 (58.2) | 0.0818 | 0.0901 |
| Shampoo/Conditioner | 28/86 (32.6) | 173/733 (23.6) | 0.1909e | 0.0762 |
| Hair Products (spray, etc) | 22/82 (26.8) | 180/711(25.3) | 0.1676e | 0.0799 |
| Hair colorants | 25/68 (36.8) | 213/606 (35.1) | 0.1905e | 0.0840 |
| Body lotions | 57/86 (66.3) | 353/737 (47.9) | 0.0056 | 0.1236 |
| Deodorants | 35/84 (41.7) | 305/721 (42.3) | 0.7168 | 0.0410 |
| Antiperspirants | 30/82 (36.6) | 275/700 (39.3) | 0.3498 | 0.0648 |
| Sunscreens | 36/87 (41.4) | 257/705 (36.5) | 0.1042 | 0.0882 |
| Powders/talc | 14/69 (20.3) | 121/604 (20.0) | 0.6666e | 0.0483 |
| Perfumes/Cologne | 33/78 (42.3) | 261/698 (37.4) | 0.0892 | 0.0916 |
| Scented products | 41/79 (51.9) | 344/723 (47.6) | 0.1224 | 0.0850 |
| Anti-aging products | 24/62 (38.7) | 159/499 (31.9) | 0.1181e | 0.1023 |
| Facial cleansers | 52/85 (61.2) | 386/708 (54.5) | 0.0504 | 0.0992 |
| Facial Astringents | 46/76 (60.5) | 350/618 (56.6) | 0.2165 | 0.0801 |
Table 4: Skin sensitivity to health and beauty products: Self-reported sensitivity to each product (any levela perceived sensitivity) compared to all respondersb.
Finally feminine products were similarly likely to be described as a source of skin sensitivity with the exception of perfumes used in the genital area. Southern women were more likely to report genital perfumes as triggers for skin sensitivity. Southern women were more likely than Ohio women to report cleaning products such as laundry softener and dishwashing soap as triggers for skin sensitivity as well (Table 5).
| Feminine Product | Responses by Geographical Area n/N (%) | Chi square Probabilityc | Phi Coefficientd | |
|---|---|---|---|---|
| MS | OH | |||
| Menstrual pads | 20/62 (32.3) | 265/683 (38.8) | 0.1052e | 0.0907 |
| Panty liners | 15/62 (24.2) | 202/689 (29.3) | 0.4590e | 0.0587 |
| Incontinence pads | 2/28 (7.1) | 25/270 (9.3) | 0.7993e | 0.0582 |
| Tampons | 6/63 (9.5) | 144/624 (23.1) | 0.0336e | 0.1125 |
| Feminine wipes | 18/53 (34.0) | 122/437 (27.9) | 0.6570e | 0.0573 |
| Soaps | 40/81 (49.4) | 361/730 (49.5) | 0.3691 | 0.0623 |
| Deodorants | 17/65 (26.2) | 182/535 (34.0) | 0.3917e | 0.0707 |
| Douching products | 6/41 (14.6) | 64/323 (19.8) | 0.7286e | 0.0598 |
| Perfumes | 16/58 (27.6) | 163/483 (33.7) | 0.0287e | 0.1293 |
| Toilet paper | 14/80 (17.5) | 150/709 (21.2) | 0.8564e | 0.0313 |
| Underwear/clothing | 46/82 (56.1) | 265/718 (36.9) | 0.0066e | 0.1237 |
| Laundry detergent | 42/85 (49.4) | 318/737 (43.1) | 0.2514 | 0.0706 |
| Softener | 24/83 (28.9) | 223/725 (30.8) | 0.0435e | 0.1003 |
| Dishwashing soap | 25/85 (29.4) | 167/732 (22.8) | 0.0497e | 0.0979 |
| Household cleaners | 48/86 (55.8) | 397/743 (53.4) | 0.8097 | 0.0341 |
Table 5: Skin sensitivity to feminine products and household cleaning products: Any self-reported sensitivitya to each product compared to all respondersb.
Although differences in overall sensitivity between women in Mississippi and Ohio were not dramatic (77.5% as compared to 68.9%), women in Mississippi reported any skin sensitivity at significantly higher rates than those in Ohio. Additionally, women with selfperceived skin sensitivity were more likely to report their skin as very sensitive in Mississippi, but more likely to report their skin as slightly sensitive in Ohio. Sensitive skin subjects in Ohio were similarly more likely to report very sensitive body skin, and Mississippi subjects significantly more likely to report that their body skin was only slightly sensitive. Mississippi sensitive skin subjects were also more likely to report genital skin as very sensitive (Table 1).
The Mississippi population was older than that surveyed in Ohio and although populations of African American and European-American subjects were fairly similar, the Mississippi study did not recruit any Asian or Hispanic subjects. This disparity could have influenced the respective prevalence of sensitive skin in the two areas, as ethnic differences in skin structure and function with a potential to influence skin sensitivity have been observed, (e.g. thickness and lipid content of the stratum corneum, resistance of stratum corneum to stripping, and baseline transepidermal water loss [TEWL]) [29]. In order to facilitate statistical comparison or the Mississippi and Ohio populations, therefore, the Hispanic and Asian subjects were eliminated from the Cincinnati cohort for analysis. It should be noted as well, however, that previous studies, have not found significant racial differences in overall skin sensitivity [1,8]. Similar age-dependent disparities in skin structure and function exist, also with potential to affect skin sensitivity (i.e, barrier function, capacity for skin repair, innervation of the skin and nerve function) [29] so it is possible that the fact that the Mississippi population was statistically older than the Cincinnati population may have influenced results. In previous studies, however, no significant impact of age on skin sensitivity has been observed [1,12].
Mississippi and Ohio do have dramatically different climates. Mississippi experiences mild winters, but long summers characterized by high temperatures and high levels of humidity; Cincinnati, Ohio, has mild summers but cold winters. In this study, however, the only significant association observed was among Mississippi women, who were more likely to report skin sensitivity to wind; southern women, notably, reported no more sensitivity to heat than women in the Cincinnati area.
Cultural factors which influence southern women as compared to those farther north are widely recognized to be dramatically different. The South, particularly, is known for the more delicate female, the “southern belle” (a stereotypical ideal woman) that is still very much a part of southern culture. Well-documented in the popular literature, the significant difference between Ohio and Mississippi with respect to regional culture may play a substantial role in the higher self-reported skin sensitivity observed in this study among southern women [30].
Interestingly, southern women were revealed specifically to report sensitivity to facial moisturizers, lotions, and skin and eye cosmetics (products specifically associated with “primping”) more often than their northern counterparts, an observation that may imply that a more prevalent exposure to these products might be behind the increased perception of sensitivity.
It is interesting, as well, to compare our data from the South and the Midwest to other regional data from the US gathered by other authors, Jourdain et al. [8] and Misery et al. [1] (Figure 3). Jourdain et al. collected data from women in San Francisco, California, in 1998; Misery et al. [1] evaluated both men (49.8%) and women (50.2%) in four regions of the US (East, Central, Mountain, and West) in 2007. Since this regional comparison was not planned before data was obtained, treatment of the data was not uniform among authors. In the Misery survey, Ohio and Mississippi were both included in the Central region but regional differences were not reported. A comparison of study designs and populations is displayed in Table 6.
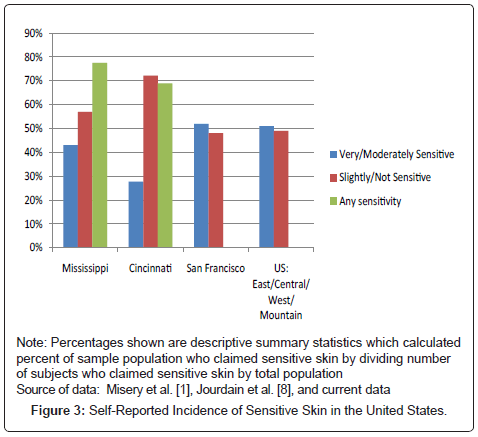
Figure 3: Self-Reported Incidence of Sensitive Skin in the United States.
| Author | Misery et al., 2011 [1] | Jourdain et al., 2002 [8] | Farage et al., 2009 [13] | Farage, 2013 | |||
|---|---|---|---|---|---|---|---|
| Year study conducted | 2007 | 1998 | 2006 | 2011 | |||
| Perceptions surveyed | Sensitive (sensitive or very sensitive) vs Not Sensitive (slightly or not sensitive) | Agreement/ Disagreement, slightly/strongly with “I have sensitive facial skin” |
Slightly, moderately, very, or not sensitive overall, facial, body, genital areas | ||||
| Other factors surveyed | Skin type, environmental and climatic factors, skin disorders, cosmetics use | Skin type, environmental and climatic factors, skin disorders, cosmetics use, food and beverages | Skin type, environmental and climatic factors, skin disorders, cosmetics use, hygiene and personal care products, household products | ||||
| Manner in which survey was conducted | Telephone | Telephone | Face-to-face | Face-to-face | |||
| Geographic Area | East | Central | West | Mountain | CA | OH | MS |
| Population setting | Mixed (urban/suburban/rural) |
Urban/ suburban |
Urban/ suburban |
Primarily rural | |||
| Number surveyed | 177 | 225 | 229 | 363 | 811 | 1039* | 89 |
| Sex: | |||||||
| Female | 50.2% | 100% | 83.6% | 100% | |||
| Male | 49.8% | 0% | 15.7% | 0% | |||
| Age range | 830 respondents were 18-64 154 respondents were > 65 |
18-54 | 18-76 Mean age 34.1 |
20-74 Mean age 44.9 |
|||
| Ethnicity | |||||||
| White | 70.1% | 25.9% | 78.7%** | 86.1% | |||
| Black | 12.0% | 24.8% | 12.1% | 13.9% | |||
| Hispanic | 13.4% | 24.7% | 1.2% | - | |||
| Asian | 2.7% | 24.7% | 1.5% | - | |||
| Not Reported | 1.8% | - | 6.2% | - | |||
Table 6: Comparison of studies evaluating sensitive skin in the US.
The Ohio and Mississippi surveys included the categories of “any sensitivity” compared to “no reported sensitivity” as well as “slightly,” “moderately,” and “very sensitive,” but Misery reported non-sensitive skin results as those who were self-described as “slightly sensitive or not sensitive” compared with sensitive as “sensitive or very sensitive.” Jourdain determined skin sensitivity by responses of strongly or somewhat agree or disagree to the statement “I have sensitive facial skin.” The Ohio and Mississippi studies included skin overall as well as anatomical sites of face, body, and genitals. The Misery study was general skin sensitivity and the Jourdain study was specifically facial skin.
Although no statistical comparisons could be made between the four reports of US sensitive skin data displayed in Figure 3 (Jourdain and Misery do not report specific data for “any sensitivity”), southern women are observed to report any skin sensitivity at a higher level compared to Ohio. Interestingly, Mississippi has a higher level of reported very/moderately sensitive skin than Ohio but less than that of San Francisco or the United States as a whole. However, Mississippi reports slightly sensitive skin at a lower level than Ohio.
In summary, this study confirms previous studies by demonstrating that women in every region of the United States, like women in other parts of the world, report some degree of skin sensitivity at fairly high levels, with sometimes significant regional differences difficult to explain on a solely biological basis. An admitted limitation of this study is that it evaluated only self-reported sensitivity skin and did not evaluate physical signs of irritation. As research efforts to identify consistent associations between irritants and sensitivity responses, however, much research has focused on information that can be attained by using epidemiological self-report methodology. As the biological contributors to the widespread perception of skin sensitivity in women continue to be unraveled, a reliable association of biophysical markers of skin irritation to the subjective experience of skin sensitivity will likely be achieved. In the meantime, epidemiological research has contributed significantly to a better understanding of these widespread perceptions of skin sensitivity, establishing its worldwide prevalence, identifying common triggers, and revealing populationbased differences that beg explanation. Cultural differences that may influence perceptions of sensitive skin have been largely unexplored; further consideration of the possible psychosocial component of sensitive skin perceptions, including culture, will contribute to a better understanding of the multifactorial nature of this pervasive complaint, including what sociological or economical factors can modify the frequency of this disorder. This paper supports a need to consider cultural influences on perceptions of sensitive skin.
The authors are grateful to Ms. Zeinab Schwen and Ms. Wendy Wippel (Strategic Regulatory Consulting, OH, USA) for review assistance with this manuscript and to Dr. Paul S. Horn (Department of Mathematical Sciences, University of Cincinnati, OH) for help with statistical analysis.