Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2015) Volume 5, Issue 3
Background: Urokinase plasminogen activator (uPA) is a serine protease which transforms inactive plasminogen into active plasmin. UPA plays an important role in neoplasm progression, cell growth and metastases through degradation of proteins in basement membranes and extracellular matrix. The aim of the study was the analysis of serum uPA concentration in patients suffering from pancreatic ductal adenocarcinoma (PDAC) and chronic pancreatitis (CP) in order to determine its possible diagnostic and prognostic value.
Methods: A study group involved 90 patients: 40 patients with PDAC, 30 patients with CP and 20 healthy individuals. UPA serum concentration was evaluated with ELISA.
Results: We observed the threefold increase of uPA serum concentration in patients with PDAC (3,23 ng/ml), twofold increase of uPA serum concentration in patients with CP (2,18 ng/ml) compared to the control group (1,01 ng/ ml) (PDAC vs CP p<0,01; PDAC vs control p<0,01; CP vs control p<0,01). We revealed significant positive correlation between uPA serum level and CA19-9 (r=0.305 p<0,05) in all analyzed groups. We also found the significant correlation between serum uPA concentration and the survival time. Higher uPA concentration was observed in patients with shorter survival time (r=-0,391; p<0,05). Significant differences were present between uPA levels lower and greater than 2 ng/ml and the patients survival time (p<0,05).
Conclusions: The presented results confirm the negative prognostic role of high serum uPA concentration in pancreatic cancer patients. The significant positive correlation between uPA serum concentration and CA19-9 provides new insights into the potential role of uPA in pancreatic cancer diagnosis.
<Keywords: Chronic pancreatitis, Pancreatic ductal adenocarcinoma,Prognostic marker, uPA
uPA: Urokinase Plasminogen Activator; PDAC: Pancreatic Ductal Adenocarcinoma; CP: Chronic Pancreatitis
Pancreatic ductal adenocarcinoma (PDAC) accounts for 3 % of all malignant neoplasms diagnosed each year in the world and is the fourth most common cause of cancer related deaths [1]. The aggressive course, late diagnosis and resistance to the treatment results in 5 year survival lower than 5% and very high mortality during 6 months after diagnosis. At the diagnosis 80-90% patients have an advanced disease and the tumor is inoperable [2-4]. Numerous studies concentrate on developing specific and sensitive diagnostic and prognostic markers of PDAC, but the results are so far unsatisfactory [5-10]. Chronic pancreatitis (CP) is a risk factor for PDAC and increases its risk even 10 to 20-fold, especially in advanced cases [11]. It is estimated that 4% of all PDAC is found among CP patients [12]. There is a growing evidence that extracellular matrix (ECM) cells play an important role in the development of PDAC. Desmoplastic environment with myofibroblastic stellate cells regulates neoplasm progression and capability to metastasize [13-18]. Cell migration, tissue transformation both in normal and pathologic states are also driven by extravascular activity of fibrinolysis proteins cascade [19]. The plasminogen activation system includes: urokinase plasminogen activator (uPA) controlled by the receptor of urokinase plasminogen activator (uPAR), tissue plasminogen activator (tPA) and inhibitors PAI-1 and PAI- 2 [20,21]. Plasminogen activators released from cancer cells catalyze the proteolytic conversion of the inactive zymogen plasminogen to the active proteinase plasmin. Tissue plasminogen activator plays a role in intravascular fibrinolysis. Additionally, uPA regulates extravascular proteolysis. Active plasmin catalyzes degradation of proteins in basement membranes and extracellular matrix and thus facilitates cancer cell invasion into surrounding tissue [21-30]. Urokinase plasminogen activator initiates (independently or through the activation of plasmin) metalloproteinases and growth factors: fibroblast growth factor – FGF, vascular epithelial growth factor – VEGF, insulin growth factor – IGF, tumor necrosis factor alfa – TNFα. Additionally, uPA stimulates cellular migration, induces chemotaxis and angiogenesis, thus promoting cancer invasion and metastasis formation [21-29,31,32]. Many studies presented an increased tissue expression of uPA in malignant neoplasms of breast, ovary, colon, oesophagus, stomach, liver, prostate and bladder which correlated with poor prognosis [33-41]. First study on the role of uPA in PDAC was conducted by Takeuchi et al. [42] and confirmed high immunoexpression of this protein in 78% of pancreatic adenocarcinoma surgical specimen which correlated with shorter survival. Harvey et al. [43] presented high expression of uPA in PDAC cells in 93% cases and also in surrounding uninvolved pancreatic cells in 87,5% of patients. No uPA expression was detected in pancreatic tissue distant from the tumor. In 37% of cases high immunoexpression of this protein was observed in blood vessels surrounding the malignant lesion. Patients with overexpression of uPA had a trend toward poor survival. The majority of uPA studies in PDAC were conducted in cell lines and postoperative specimen. There is no data regarding uPA serum levels in PDAC and CP. Some authors suggest the correlation of uPA serum concentration and tumor tissue expression in various human cancers [44,45]. The aim of the study is the analysis of uPA serum concentration in patients suffering from pancreatic ductal adenocarcinoma and chronic pancreatitis and evaluation of its possible role in PDAC and CP diagnosis and prognosis.
A group of 90 patients was examined: 40 patients with PDAC (19 women, 21 men, median age 65 years; range 35-89 years), 30 patients with CP (5 women, 25 men, median age 47, 3 years; range 28-69 years) hospitalized in the Department of Digestive Tract Diseases, Medical University of Lodz. The control group consisted of 20 healthy volunteers. The informed consent was obtained from all study participants. Final diagnosis of PDAC was based on imaging techniques (abdominal ultrasound, computed tomography, endoscopic ultrasound) and confirmed by cytological evaluation of material from common bile duct taken at ERCP, fine needle aspiration biopsy under EUS guidance or postoperative specimen pathology. The diagnosis of CP was made based on medical history and imaging studies (abdominal ultrasound, computed tomography). The resectability criteria of PDAC was lack of distant metastases, major blood vessels infiltration or lack of invasion of upper part of portal vain or lower part of superior mesenteric artery which allows for surgical vessel reconstruction. The data concerning patient’s demographics, symptoms and stage of the disease (according to TNM scale) were correlated. The time of survival was calculated from the time of diagnosis to the time of death. In all patients the blood samples were taken consistently at the time of the tumor detection in imaging diagnosis. Only patients with confirmed PDAC were included into this study. We followed up patients with CP for 3-4 years. We did not reveal any suspected pancreatic malignant lesions in chronic pancreatitis patients (yearly EUS/CT surveillance). We followed up PDAC patients until death (mean 242 days + 236; range 20-1039 days), 8 patients are still alive (mean 316 + 242 days; range 114-898). The concentration of uPA was measured in serum using enzyme-linked immunosorbent assay (ELISA) “sandwich” method by IMUBID® uPA ELISA Kit from American Diagnostica inc. The assay was conducted according to producer’s manual.
The distribution of uPA and CA 19-9 was not compatible with the normal distribution, so we used nonparametric tests for the statistical analysis. For measurable variables (age, uPA and CA 19- 9) we calculated following parameters: mean, median, SD, SE. We compared three groups using ANOVA rang Kruskal-Wallis test followed by a multiple comparisons test. We compared two groups using Mann-Whitney U-test. For immeasurable variables we defined two-way tables. To determine the relationship between the different characteristics of different groups we used the χ 2 test or χ 2 with Yates correction. Moreover, we calculated matrix correlation of all measurable characteristics with each other for all subjects and in PDAC and CP groups. To analyze the differences in survival of patients between groups we used Gehana test Wilcoxona, Mantel- Cox test and log-rank test. The results were statistically analyzed with Statistica software. Statistical significance was established at p<0.05. The study had an approval of local bioethics committee: RNN/168/10/KE.
The characteristics of patients are presented in Table 1. There was no statistical difference in age structure between PDAC patients and patients in control group. Patients with pancreatic cancer were significantly older than CP patients – 65,4+11,8 vs 47,3+10,5 (p<0,01). The mean serum concentration of uPA in patients with PDAC was 3,23ng/ml (SD ± 1,84; range: 1,24 - 7,6; median: 2,75) in CP: 2,18ng/ml (SD ± 1,45; range: 0,88 - 5,4; median: 1,51) and in the control group: 1,01 ng/ml (SD ± 0,32; range: 0,2 -1,66, median: 1,05) – Figure 1. The increase of uPA concentration was observed in patients with PDAC (threefold), and CP (twofold) compared to the control group. The differences between all groups were statistically significant (PDAC vs CP p<0.01; PDAC vs control p<0.01; CP vs control p<0.01) – Figure 1. There was no correlation between uPA concentration and patients’ age, gender, diabetes presence, pain and weight loss in pancreatic cancer patients. The presence of jaundice in PDAC patients correlated significantly with uPA serum concentration (p<0.01). Tumor was localized in the head of pancreas in 32 patients with PDAC (80%), in pancreatic body in 6 patients (15%) and in the tail in 2 individuals (5%).
| Characteristic of patients: | Pancreatic ductal adenocarcinoma | Chronic pancreatitis | Control group |
|---|---|---|---|
| Number of patients: | 40 | 30 | 20 |
| Sex: women | 19 (47,5%) | 5 (16,7%) | 9 (45%) |
| men | 21 (52,5%) | 25 (83,3%) | 11 (55%) |
| Age: women | 71 (52-89) | 49,8 (40-57) | 70 (31-88) |
| men | 60 (35-81) | 46,8 (28-69) | 64,5 (18-88) |
| Medium age | 65,4+11,8 | 47,3+10,5 | 66,9+19,5 |
| Symptoms: jaundice | 27 ( 67,5%) | 2 (11%) | - |
| Duration of symptoms: | 10 weeks (1 week- 6 months) |
2-40 years | - |
| Diabetes | 16 (40%) | 10 (33,3%) | - |
| Duration of DM: | 4 months- 20 years de novo - 2 (5%) |
2-11 lat | - |
| Tobacco smoking | 17 (42,5%) | 21 (70%) | 1 (5%) |
| Excessive alcohol concumption | 4 (10%) | 17 (56,6%) | - |
| Family history of cancer disease | 8-malignant tumor different than PC (20%) 3-pancreatic cancer (7,5%) | negative | negative |
Table 1: The characteristics of patients with PDAC, CP and control group.
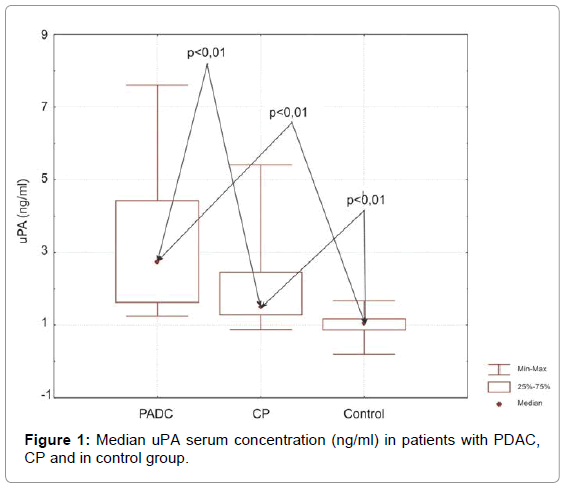
Figure 1: Median uPA serum concentration (ng/ml) in patients with PDAC, CP and in control group.
The serum concentration of CA 19-9 was evaluated in all patients. We revealed significant positive correlation between uPA serum level and CA19-9 (r = 0.305; p<0,05)- Figure 2. In individuals in which CA 19-9 level was lower than 500 U/mL the mean uPA concentration was 2,72 ng/ml (SD ± 1,72). Those with CA 19-9 levels greater than 500 U/ ml presented with mean uPA concentration of 3,70 ng/mL (SD ± 1,85). The difference was statistically significant (p<0,05)– Figure 3. We also examined the CA19-9 level in patients with uPA concentration lower and greater than 2 ng/ml and we confirmed statistically significant difference: 129,7 vs 280,2, respectively (p<0,01). In PDAC patients with CA 19-9 concentration >500U/mL, the survival was shorter than in those with CA 19-9 concentration <500 U/ml: 201,87 days (SD ± 150) vs 271,73 days (SD ± 289,52), with no statistical significance (p = 0,345). The sensitivity of uPA in detecting PDAC was 54%, specificity 84%, PPV 76% and NPV 67%. The sensitivity of CA19-9 in PDAC diagnosis was 72%, specificity 97%, PPV 97% and NPV 69%. The integrated evaluation of uPA and CA19-9 increases sensitivity and specificity of PDAC diagnosis to 63% and 90,5%.
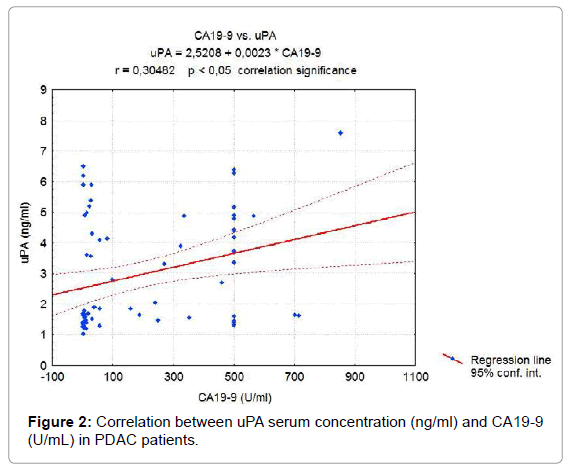
Figure 2: Correlation between uPA serum concentration (ng/ml) and CA19-9 (U/mL) in PDAC patients.
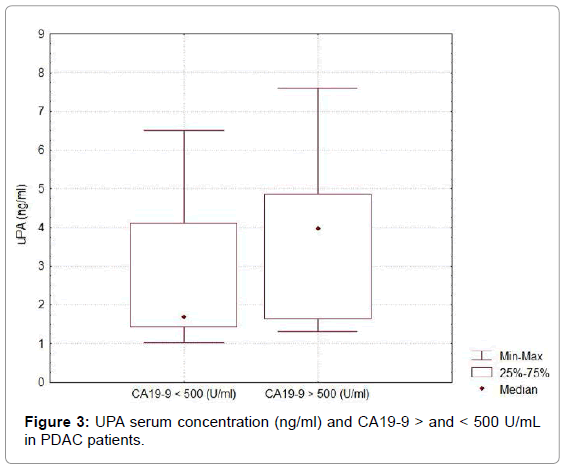
Figure 3: UPA serum concentration (ng/ml) and CA19-9 > and < 500 U/mL in PDAC patients.
Among all patients with PDAC, 9 had stage I tumor according to TNM classification (22.5%), 9- stage II (22.5%), 5- stage III (12,5%) and 17- stage IV (42,5%). Mean uPA concentration was 2,8 ng/ml (± 1.57) in stage I, 3,79 ng/ml (± 2,1)- stage II, 3,67 ng/ml (± 2,4)- stage III and 3,03 ng/ml (± 1,7) in stage IV. There were no significant differences between mean serum uPA concentrations in the different PDAC stage. Mean survival time in different TNM stages was accordingly: 345,5 days in stage I, 405,7 days- stage II, 156,2 days- stage III and 155,7 days- stage IV. The difference of survival time was significant between combined stages I and II vs combined stages III and IV (p<0,05). Among all patients with chronic pancreatitis 1 had stage I (3%) according to Cambridge classification, 3- stage II (10%) and 26- stage III (87%). No correlation between uPA level and CP advancement was found.
Among 40 patients with PDAC, 21 of them were qualified for surgery (52,5%). Radical resection - Whipple pancreatoduodenectomy was performed in 7 patients (33,3%; 17,5% cases).
In 14 patients (66,7%) the tumor appeared to be locally advanced and 6 of them had palliative by-pass anastomosis. Patients who underwent radical resection of PDAC presented with lower serum concentration of uPA comparing to patients with nonresectable PC – 2,28 ng/ml ± 1,24 (1,3 - 4,2) vs 3,4 ng/ml ± 1,89 (1,24 - 7,6), however no statistical significance was noted (p=0,14).
There was a significant correlation between serum uPA concentration and the survival time. Higher uPA concentration was observed in patients with shorter survival time (r = -0,391; p<0,05; Figure 4). Significant differences were present between uPA levels lower and greater than 2 ng/ml and patients survival time (p<0,05). Longer survival was observed in individuals with uPA concentrations lower than 2 ng/ml– 335 days (SD ± 313,75) vs 181 days (SD ± 155) in group of patients with uPA concentration greater than 2 ng/ml – Figure 5. Kaplan Meier survival curves are demonstrated in Figure 6. Statistical analysis confirmed that uPA can be an independent predictive factor for survival.
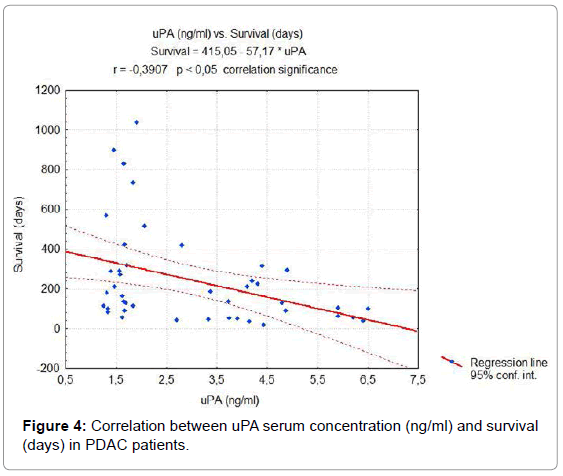
Figure 4: Correlation between uPA serum concentration (ng/ml) and survival (days) in PDAC patients.
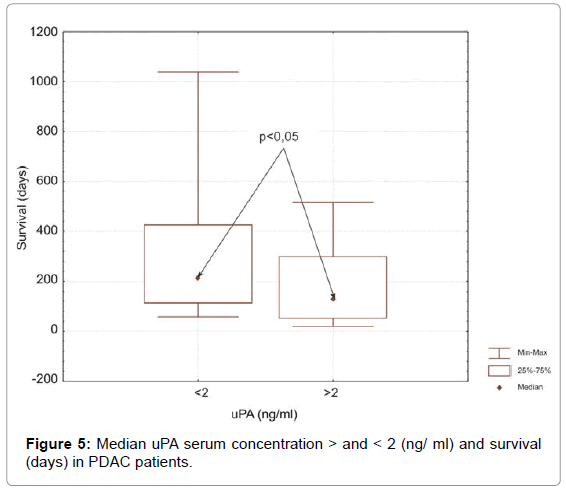
Figure 5: Median uPA serum concentration > and < 2 (ng/ ml) and survival (days) in PDAC patients.
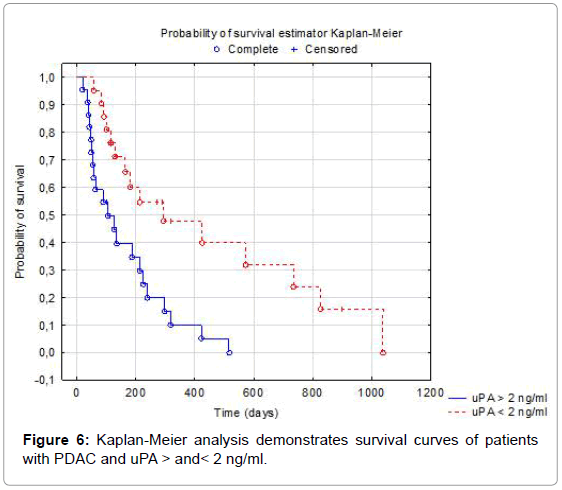
Figure 6: Kaplan-Meier analysis demonstrates survival curves of patients with PDAC and uPA > and< 2 ng/ml.
In our study, we found a 3-fold increase of uPA serum levels in patients with pancreatic cancer comparing to control group. There was only one study so far, conducted by Gibbs et al. [44] which evaluated uPA serum concentration in 11 patients with pancreaticobiliary cancer. The analysis showed its 2-fold increase compared to healthy subjects (1,27 ng/ml vs 0,56 ng/ml). The same authors evaluated uPA immunoexpression in 6 out of 8 brush cytology material from bile ducts taken at ERCP in pancreatic cancer patients (75%). The serum concentration of uPA correlated with its expression in brush cytology material (r=0,72; p<0,0001). Other research evaluated uPA immunoexpression in pancreatic cancer surgical specimen. Takeuchi et al. [42] confirmed high immunoexpression of this protein in 78% of pancreatic adenocarcinoma tissue samples. Similarly He [45] found expression of uPA in 17 of 20 (85%) examined pancreatic cancer tumors. Also Harvey et al. [43] presented high expression of uPA in PC cells in 93% cases and also in surrounding uninvolved pancreatic cells in 87,5% of patients and no uPA expression in pancreatic tissue distant from the tumor. High uPA concentration might result from its expression in cancer cells, extracellular matrix cells and endothelium involved in neoangiogenesis [46].
Multiple studies have reported the correlation between high levels of uPA and poor prognosis in different malignancies [34-41]. We have found a significant correlation between high uPA serum concentration in PDAC patients and shorter survival. Similar results were obtained by Cantero et al. [47] who revealed that PDAC patients with increased expression of uPA and uPAR had significantly shorter survival comparing to those without these biomarkers expression (9 months vs 18 months). Takeuchi et al. [42] also confirmed the correlation of high uPA immunoexpression and shorter survival in PDAC. Whereas, Harvey et al. [43] confirmed that patients showing overexpression of uPA showed a trend toward poorer survival, with no statistical significance. The correlation between high uPA concentration level and poorer survival may be the result of proteolytic activity of uPA [20], contributing to an early invasion of basal membrane and degradation of extracellular matrix [22,23], which enables cancer cells for local invasion and forming metastases in distant organs [47,48]. We found the significant difference of survival time between patients with combined stages I and II vs combined stages III and IV. Additionally, there was a significant positive correlation between the presence of jaundice in PDAC patients and uPA serum concentration. Similar results were presented by Sorio et al. [48] who analyzed urinary level of uPAR in PDAC and did not find its correlation with the TNM stage. On the contrary, Nielsen et al. [46] showed a 75-fold higher expression of uPA mRNA in stage III PDAC (according to UICC) in comparison to its expression in healthy pancreas, whereas in stage I and II uPA mRNA increase was minimal. Those discrepancies may be explained by different tumor classification and small group of patients (21 PDACs) in the last mentioned study. He et al. [45] revealed stronger staining for uPA at cancer nests of the metastatic pancreatic cancers compared with non-metastatic pancreatic cancers. We have also evaluated the serum uPA diagnostic value. Our data indicate significant positive correlation between uPA serum concentration and CA19-9. Unfortunately, uPA sensitivity and specificity in detecting pancreatic cancer did not exceed the diagnostic value of CA19-9. To our knowledge, there is no other study that analyzed correlations of uPA and CA 19-9 serum concentration in pancreatic cancer and chronic pancreatitis. Herszenyi et al. [49] analyzed the concentration of uPA, CEA and CA 19-9 in serum of patients suffering from colon cancer showing 69% sensitivity of uPA in detecting this tumor, while the sensitivity of CEA and CA 19-9 was 30% and 18%, respectively. Huber et al. [50] examined similar group of patients presenting higher diagnostic sensitivity of uPA comparing to combination of CEA and CA19-9 (75,5% vs 51,5%). Further improvement of uPA diagnostic efficacy might be obtained by including more PDAC patients in different stages into the study. There is a presumption that uPA is produced by interstitial stromal elements and further taken up in a paracrine fashion by receptors located on neighboring cells [51,52]. In chronic pancreatitis, a urokinase-dependent plasminogen activation occurs, contributing to the remodeling and damage of pancreatic parenchyma [53]. Our study showed a 2-fold increase of mean uPA serum concentration in patients with chronic pancreatitis comparing to healthy individuals. There was also a significant difference between the mean concentration of this protein in PDAC and CP. No correlation between uPA level and CP advancement was found. Friess et al. [53] presented increased expression of uPA mRNA (5,2 fold; p<0,001) and uPAR mRNA (5,9-fold; p<0,001) in 8 out of 14 pancreatic tissue samples with CP compared to normal pancreas. Moderate to strong mRNA staining was present in acinar cells, some ductal cells and areas with ductal metaplasia. Similar results were presented by immunohistochemical analysis of surgical specimen. Intense expression and immunostaining of these proteins in CP was associated with a higher degree of pancreatic damage: parenchyma destruction, fibrosis and metaplasia. Harvey et al. [43] confirmed positive staining for uPA in stromal elements, mainly histiocytes, monocytes and occasionally fibroblast in PDAC tissue specimen.
The presented results confirm the negative prognostic role of high uPA serum concentration in pancreatic cancer patients. Nevertheless, our data do not confirm diagnostic value of uPA serum concentration in PDAC patients. The significant positive correlation between uPA serum concentration and CA19-9 provides new insights into the potential role of uPA in pancreatic cancer diagnosis. Larger studies are needed especially in those with unidentified pancreatic masses, to evaluate its value in pancreatic cancer diagnosis and prognosis.
No conflict of interest was declared.
This study was supported by a research grant from Medical University of Lodz: 503/1-002/503-01, 502-03/1-002-01/502-14-040 and Polish Society for the Prevention of G.I. Neoplasms.