Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2015) Volume 4, Issue 2
Objective: To highlight the increased risk of severe hyperthyroidism leading to decompensation of pulmonary and cardiac hemodynamics post initiation of epoprostenol for treatment of pulmonary arterial hypertension (PAH).
Methods: Review of literature shows an increased incidence of autoimmune thyroid disease in patients
undergoing treatment of PAH with epoprostenol. We describe two incidences of seropositive thyrotoxicosis associated with acute decompensation of pulmonary and cardiac function.
Results: We report two patients with no prior history of thyroid disease who developed severe hyperthyroidism after initiation of epoprostenol.
Conclusions: Clinicians should be aware of the potential for development of severe hyperthyroidism leading to rapid decompensation in cardiac and respiratory status after initiation of epoprostenol in patients
Autoimmune thyroid disease has been described in patients with pulmonary arterial hypertension (PAH) [1]. However, the time of onset and type of thyroid disease associated with PAH is variable. Case reports suggest a higher prevalence of hypothyroidism than hyperthyroidism in patients with PAH [2,3]. Epoprostenol, an endothelium-derived prostacyclin is a systemic and pulmonary vasodilator that inhibits platelet aggregation through increased intracellular cyclic adenosine monophosphate (cAMP) activity [4]. Prostacyclins have antiproliferatives, antithrombotics and immunomodulatory activity and are frequently used in the treatment of PAH. Initiation of epoprostenol has been reported with thyroid disease in some studies [5]. We describe two cases of acute hyperthyroid autoimmune disease in previously euthyroid patients who were started on epoprostenol for PAH. The severity of hyperthyroidism resulted in worsening pulmonary/cardiac status and rapid growth of a compressive goiter in one patient suggesting that thyroid function should be monitored closely in PAH patients.
Case 1 is a 63 year old woman with history of PAH on epoprostenol for 9 months who presented to the Emergency Department with a chief complaint of 2-3 months of weight loss, worsening dyspnea on exertion, tremors, increasing diarrhea, and increased oxygen requirements. She had no personal or family history of thyroid disease. Physical exam was notable for heart rate of 120, diffusely hyperemic skin, no exophthalmos, proptosis or lid lag, normal size thyroid without discrete nodules, no thyroid bruit and no cervical lymphadenopathy. Laboratory evaluation revealed: TSH<0.01 mIU/L (ref 0.4-4.0), FT4 3.02 ng/dL (ref 0.70-1.80), T3 229 ng/dL (ref 83-160), thyroid-stimulating immunoglobulin activity 496% (ref<140%), and antiTPO Abs 774 IU/mL (ref<5.0). Radioactive iodine uptake scan at 4 hours was diffusely increased at 32.9% (expected 5-15%). She was started on methimazole and a beta-blocker. Thyroid function tests normalized and cardiopulmonary function improved with decreased oxygen requirements and she remained on continuous infusion epoprostenol. The patient remained euthyroid on low dose methimazole and is currently awaiting lung transplantation for her PAH.
Case 2 is a 33 year old man with history of PAH on epoprostenol for 6 months who presented to a local Emergency Department with a chief complaint of difficulty breathing and rapid, severe neck enlargement. He had no personal or family history of thyroid disease. Physical exam was notable for heart rate of 120; plethoric face, no exophthalmos, proptosis, or lid lag; neck exam revealed a severely enlarged lobular thyroid and bilateral cervical lymphadenopathy. Due to severe compressive symptoms a neck CT with contrast was obtained which showed a diffusely enlarged thyroid gland with cervical lymphadenopathy (Figures 1 and 2). Laboratory evaluation revealed: TSH<0.02 mIU/L, FT4 4.48 ng/dL, T3 8.63 pg/mL (ref 2.3-5.0), thyroid-stimulating immunoglobulin activity 334% (ref<140%), and antiTPO Abs<1.0 IU/mL. He was started on methimazole (MMI) and a beta blocker. Thyroid function tests normalized on MMI but the beta-blocker was stopped due to deterioration in cardiopulmonary function. He underwent thyroidectomy due to continued compressive symptoms including dysphagia with the inability to swallow solid food and orthopnea requiring him to sleep in a recliner. Post thyroidectomy he resumed eating solid food and was able to sleep lying down. His cardiopulmonary function improved, oxygen requirements decreased, and he lost weight. Weight gain, not weight loss, is typically associated with treatment of autoimmune hyperthyroidism and return to a euthyroid state. However, this patient’s post treatment weight loss may have been due to improved sleep with resolution of his positional airway obstruction and decreased physiologic stress resulting in decreased production of stress hormones such as cortisol and catecholamines [6,7]. Obstructive sleep apnea (OSA) and elevated stress hormones are both associated with weight gain, obesity, insulin resistance, and type 2 diabetes. Treatment of OSA and reduction of stress hormones are associated with improved metabolism and weight loss [6]. Surgical pathology confirmed hyperplastic thyroid follicles with fibrosis and chronic inflammation, consistent with Graves’ disease (Figure 3). The presence of cervical lymphadenopathy may have been a marker of severe pulmonary hypertension however resolution of this with treatment indicates it may have been secondary to autoimmune hyperthyroidism. Lymph node biopsy was not done due to resolution of the lymphadenopathy with treatment of the patient’s hyperthyroidism.
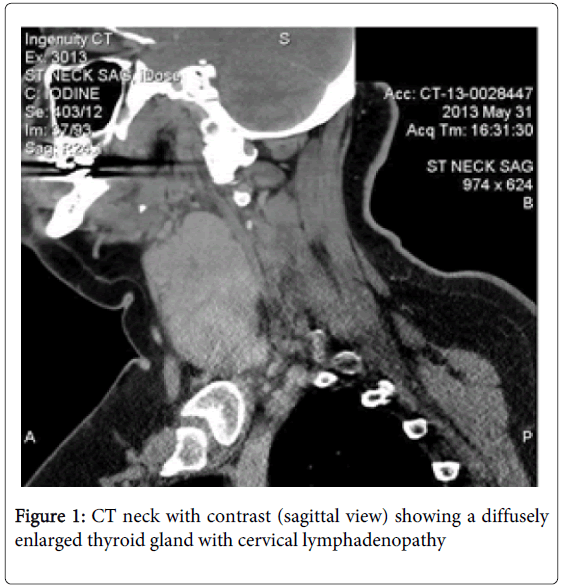
Figure 1: CT neck with contrast (sagittal view) showing a diffusely enlarged thyroid gland with cervical lymphadenopathy
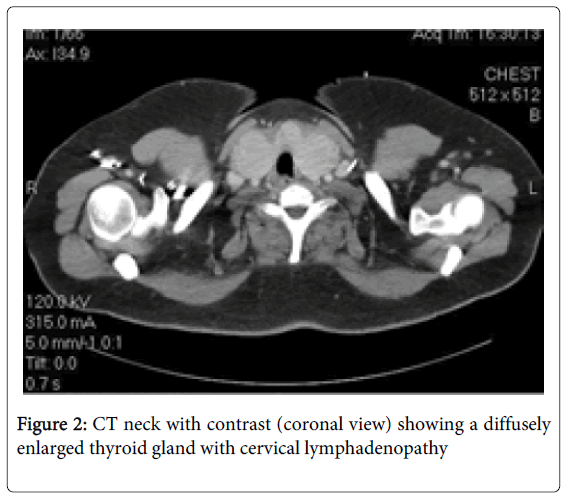
Figure 2: CT neck with contrast (coronal view) showing a diffusely enlarged thyroid gland with cervical lymphadenopathy
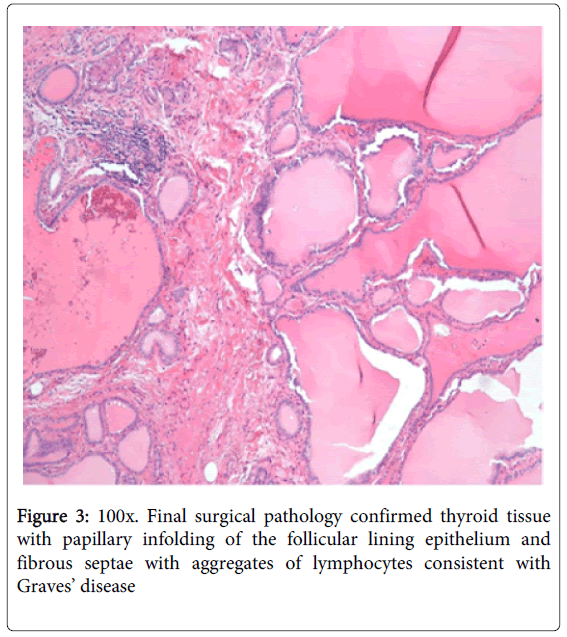
Figure 3: 100x. Final surgical pathology confirmed thyroid tissue with papillary infolding of the follicular lining epithelium and fibrous septae with aggregates of lymphocytes consistent with Graves’ disease
The prevalence of autoimmune thyroid disease in patients with PAH has been reported to be as high as 49% [1] with hypothyroidism affecting up to 10-24% of PAH patients with thyroid disease [8]. Although both hyper- and hypothyroidism have been noted, the majority of studies describe a higher prevalence of hypothyroidism or elevated TSH in patients with PAH [5]. Prior retrospective studies suggest an association between thyroid dysfunction and the diagnosis and/or treatment of PAH. Ferris et al. first postulated that epoprostenol treatment triggers thyroid disease in PAH in 2001 [8]. Chadha et al observed that the time from initiation of treatment with a PGI2 to the manifestation of hyperthyroidism in 3 patients on epoprostenol ranged from 8 to 24 months [9]. The prostacyclin epoprostenol may cause rapid thyroid enlargement and hyperthyroidism by stimulation of cAMP production in the thyroid cell membrane [10]. Chu et al. reported a possible common immunogenetic component between PAH and thyroid disorders given the higher prevalence of autoimmune thyroid disease in PAH in 2002 [1]. Thyrotoxicosis results in changes in both pulmonary and cardiac function but the mechanism is not well studied. A recent review by Marvisi et al. in 2013 described possible mechanisms may include enhanced catecholamine sensitivity leading to pulmonary vasoconstriction, increased metabolism of pulmonary vasodilating substances such as prostacyclins and/or decreased or impaired metabolism of vasoconstrictors. Finally an autoimmune process leading to endothelial damage may play a role in PAH patients [11].
We describe two cases of autoimmune hyperthyroidism in the setting of epoprostenol use for PAH. These patients had no known thyroid disease prior to initiation of epoprostenol indicating that long term treatment with prostacyclins likely induces thyroid disease in PAH patients. Clinicians should be aware of the disproportionately high rates of autoimmune thyroid disease in patients with PAH, particularly hyperthyroidism given the adverse effects of excess thyroid hormone on cardiopulmonary function including increased oxygen demand. Manifestations often occur within 2 years after initiation of epoprostenol, but can be sooner. Furthermore clinicians should be aware of the potential for development of severe hyperthyroidism with compressive goiter and worsening of cardiac and pulmonary status after treatment with prostacyclins in PAH patients. Thorough evaluation of thyroid function in all patients with PAH is warranted, especially prior to initiation of epoprostenol. Treatment of hyperthyroidism can rapidly improve cardiac and pulmonary function.