Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Case Report - (2013) Volume 2, Issue 3
Although autoimmune hypoparathyroidism is extremely rare in contrast to very common thyroid autoimmune diseases the combination of those two was recently shown to be to some extent higher than previously thought. Flareups of autoimmune diseases in the post-partum period are very common, however, to the best of our knowledge,this is the first report of an autoimmune hypoparathyroidism presenting with severe hypocalcaemia in a patient with autoimmune thyroid disease and normal thyroid function during the post-partum period. We present a case of a young woman with muscle spasms and basal ganglia calcifications due to severe hypocalcaemia induced by primary hypoparathyroidism. Here we discuss the pathophysiology and diagnostic aspects of this treatable disease.
<Insufficient parathyroid hormone (PTH) activity disturbs body calcium homeostasis with inadequate mobilization of calcium from bone matrix, reabsorption from the kidney and decreased synthesis of 1-hydroxyvitamin D, resulting in hypocalcaemia and hyperphosphatemia. Primary hypoparathyroidism remains a rare cause of hypocalcaemia with an estimated prevalence of 7.2 per million [1]. The electrolyte alterations in hypoparathyroidism mainly affect the neuromuscular system and usually result in spasms, cramps and twitching, but the spectrum of possible clinical presentations ranges from congestive heart failure to syndromes mimicking neurodegenerative disease [2]. Autoimmune hypopyrathyroidism is an extremely rare disorder. Considering post-partum evolution of symptoms and positive anti-thyreoglobuline antibodies, autoimmunity may be the likely underlying mechanism of the disease in our patient. Autoantibodies to CaSR may activate the receptor on PTH cells instead of calcium, resulting in false signaling and inhibition of adequate PTH secretion [3]. CaSR antibodies are found in up to 50% cases of idiopathic hypoparathyroidism but their role in the pathogenesis of the disease is not clear [4].
To the best of our knowledge, this is the first report of an autoimmune hypoparathyroidism presenting with severe hypocalcaemia in a patient with autoimmune thyroid disease and normal thyroid function during the post-partum period. Our patient presented with neuro-muscular symptoms due to severe hypocalcaemia in unrecognized primary hypoparathyroidism with several distinct features. Here we discuss the pathophysiology and diagnostic aspects of this treatable disease.
A 29-year old woman presented to emergency room with perioral numbness and speech difficulty resembling transitory is chemic attack. Symptoms gradually resolved after one hour. She reported several episodes of carpal spasmsin the last 18 months, starting shortly after her first delivery. Her past medical history included euthyroid multinodular goiter diagnosed 5 years earlier. Early development and family history were unremarkable.
On admission, she appeared to be in distress. General physical examination was normal except for thyroid enlargement. Neurologic examination indicated markedly reduced muscle tendon reflexes with normal muscle strength and tone and otherwise unremarkable examination, with no involuntary movements. Both Chwostek’s and Trousseau’s signs were positive. Brain computed tomography (CT) scan showed bilateral basal ganglia calcifications (Figure 1). Prolonged QT interval (QTc 0.480s) was observed on the electrocardiography. Transthoracic echocardiography was unremarkable. Laboratory analyses revealed low serum free calcium, high phosphate and normal intact parathyroid hormone (PTH) levels, inadequate for the degree of hypocalcemia (Table 1). Magnesium level was within the reference range (Table 1). Patient was euthyroid, but an increased level of serum anti-thyreoglobulin antibodies was found (Table 1). Cortisol and calcitonin levels were normal (Table 1). A moderate increase of serum creatine kinase (CK) and lactic dehydrogenase (LDH) levels were noted; CK-MB fraction was normal. Electromyography (EMG) of deltoid and quadriceps muscles showed no signs of myopathy. Brainmagnetic resonance imaging (MRI) confirmed calcifications in the basal ganglia and excluded vascular lesions. Transcranial sonography of the brain parenchima (TCS) demonstrated hyperechogenicities in both lentiform nuclei equivalent to CT and MRI findings of basal ganglia calcifications (Figure 2). Endocrinological evaluation comprising ultrasound examination, fine needle aspiration biopsy and thyroid function tests, confirmed diagnosis of benign multinodular goiter, autoimmune thyroid disease i.e. chronic lymphocytic thyroiditis with normal thyroid function.
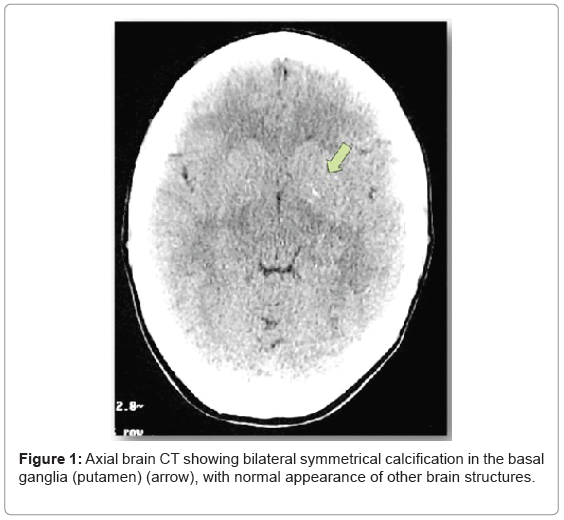
Figure 1: Axial brain CT showing bilateral symmetrical calcification in the basal ganglia (putamen) (arrow), with normal appearance of other brain structures.
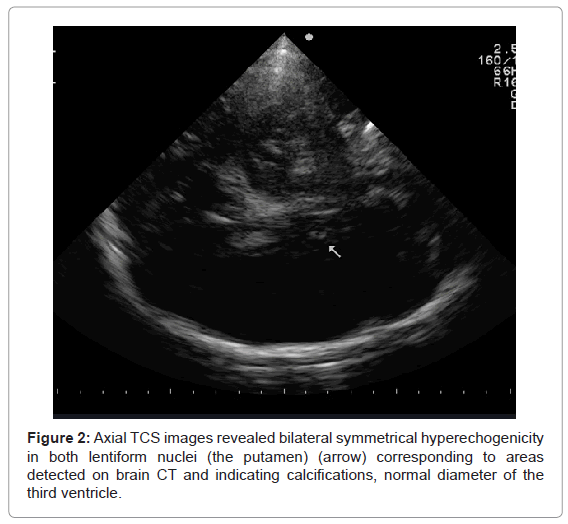
Figure 2: Axial TCS images revealed bilateral symmetrical hyperechogenicity in both lentiform nuclei (the putamen) (arrow) corresponding to areas detected on brain CT and indicating calcifications, normal diameter of the third ventricle.
Given the severe degree of hypocalcemia, the supplementation therapy was initiated with parenteral administration of calcium salts and continued with oral administration of active vitamin D3-calcitriol (1.5 μg/day) and calcium supplementation (2 g/day). Rapid and concomitant normalization of muscle enzymes level was observed with normalization of calcemia. Patient remained symptom-free during 6 months of follow-up and calcium dose was decreased to 1 g/day while D3-calcitriol was increased to 2 μg/day.
| Value (reference range) | Baseline values | Day 2 | Day 7 |
|---|---|---|---|
| Ca2+ (1.18-1.29 mmol/l) | 0.55 | 0.82 | 1.04 |
| Ca total (2.10-2.55 mmol/l) | 1.20 | 2.09 | 2.21 |
| Phosphorous (0.81-1.45 mmol/l) | 2.1 | 1.61 | 1.59 |
| Vitamin D (>75 nmol/l) | 36 | ||
| Mg2+ (0.70-1.15 mmol/l) | 0.73 | ||
| U-Ca2+ (2.5-7.5 mmol/24h) | 0.3 | ||
| PTH (15-65 pg/ml) | 34 | ||
| BUN (2.5-6.1 mmol/l) | 4.1 | ||
| Creatinine (46-92 μmol/l) | 60 | ||
| Alkaline phosphatase (38-126 U/l) | 57 | ||
| LDH (313-618 U/l) | 927 | 693 | 574 |
| CK (30-135 U/l) | 813 | 120 | 59 |
| CK-MB (0-24 U/l) | 24 | ||
| FT4 (9-22 pmol/l) | 18.4 | ||
| TSH (0.3-5.5 mU/I) | 3.76 | ||
| AntiTg Ab (<70 U/mL) | 1740.8 | ||
| AantiTPO Ab (< 130 U/mL) | 19.1 | ||
| Calcitonin(0-10 pg/ml) | 2.1 | ||
| Cortisol (131-642 nmol/L) | 429.5 |
Table 1: Laboratory values.
We present a case of a young woman with muscle spasms and basal ganglia calcifications due to severe hypocalcaemia induced by primary hypoparathyroidism. The case presentation raises several interesting points for discussion the first being the etiology of the disease.
Autoimmune hypoparathyroidism is an extremely rare autoimmune disorder. Considering post-partum evolution of symptoms and positive anti-thyreoglobuline antibodies, autoimmunity resulting in formation of auto-antibodies to calcium sensing receptor (CaSR) may be the likely underlying mechanism of the disease in our patient. Autoantibodies to CaSR may activate the receptor on PTH cells instead of calcium, resulting in false signaling and inhibition of adequate PTH secretion [3]. CaSR antibodies are found in up to 50% cases of idiopathic hypoparathyroidism but their role in the pathogenesis of the disease is not clear [4]. Since we were not able to measure CaSR antibodies we relied on other clinical and laboratory findings that supported our hypothesis of autoimmune etiology. Age at presentation, normal growth and development, absence of dysmorphic features and normal baseline cortisol values excluded rare congenital causes of primary hypoparathyroidism. The relative paucity of clinical features in opposition to a very severe degree of hypocalcaemia was suggestive of chronic, gradual decrease in calcium concentration due to autoimmune process. Although autoimmune hypoparathyroidism is extremely rare in contrast to very common thyroid autoimmune diseases the combination of those two was recently shown to be to some extent higher than previously thought [4]. This combination may be a part of an autoimmune polyglandular syndrome imposing the need for further endocrinological investigation, follow-up and extensive immunological work-up.
Flares of autoimmune diseases in the post-partum period are very common especially, in patients with positive anti-thyroid antibodies. Immune tolerance in pregnancy is the absence of a maternal response against the fetus and placenta leading to unusually successful “allografts” as the fetus is genetically different from the mother. This adaptive phenomenon involves all aspects of immune response. The physiological changes surrounding pregnancy include changes allowing an immune-tolerant environment for the fetus and this result in decline in autoantibodies. So in pregnancy there is a fall in both TPO and Tg auto-antibody levels followed by an increase in the post-partum period. Estrogen has also been shown to deliver a negative signal toward B cell function in pregnancy and this effect is lost postpartum. However, to the best of our knowledge, this is the first report of an autoimmune hypoparathyroidism presenting with severe hypocalcaemia in a patient with autoimmune thyroid disease and normal thyroid function during the post-partum period.
Another unusual finding in our patient with hypocalcaemia was markedly increased level of serum muscle enzymes. This phenomenon has rarely been reported in patients with hypocalcaemia and myopathy due to hypoparathyroidism [5-9]. While myopathy in long lasting hypocalcaemia associated with osteomalaciais well described, it is not followed by an increase in serum CK levels [10]. Increased CK levels have been linked to tetany, but several reports questioned this hypothesis, noting increased levels of CK in the absence of apparent tetany. Kruse et al. proposed a mechanism in which hypocalcaemia induced functional changes in striated muscle cells thus allowing leakage of intracellular enzyme content [11]. Some experimental data exist that support this hypothesis, which is also favored by our case. Intracellular Ca2+ concentration rises in hypocalcaemia, and presumably activates a cascade of Ca2+ dependent cytotoxic processes, which disrupt cytoskeletal and membrane organization [12,13]. We observed no manifest tetany in our patient during hospitalization and noted a rapid decline in serum muscle enzyme levels following initiation of therapy. Moreover, aside from hypoactive tendon reflexes, this patient had normal muscle strength and no evidence of myopathy on EMG. The biopsy had not been performed but available literature descriptions report mild, non-specific myopathy without inflammatory changes in similar cases [14].
Another unique feature of the presented case was the finding of hyperechogenicities in brain parenchyma on transcranial sonography (TCS). Bilateral multifocal hyperechogenicities in the basal ganglia region corresponded well to the observed calcifications on the CT and MRI images. This is highly coherent in comparison to data from previously reported results of TCS in patients with idiopathic basal ganglia calcification [15]. To our knowledge this is the first description of TCS in patients with intracranial calcifications due to primary hypoparathyroidism.
We presented a case of severe hypocalcaemia due to an unrecognizedprimary hypoparathyroidism in a patient with an autoimmune thyroid disease and normal thyroid function during postpartum period. This combination may be a part of an autoimmune polyglandular syndrome imposing the need for further endocrinological investigation, follow-up and extensive immunological work-up. We emphasize the importance of diagnosing hypocalcaemia, which can be missed for a considerable time but comprises complications that are highly preventable. Patients with hypocalcaemia should be checked for any signs of muscle damage and measurements of muscle enzyme level should be obtained as this could potentially lead to a better understanding of this interesting phenomenon. Additionally, TCS may be useful and inexpensive tool in screening patients with chronic hypocalcaemia for intracranial calcifications.
This work has been supported by the Ministry of Science and Technological Development of Serbia, Scientific Projects No. 175022 and No 175033