Angiology: Open Access
Open Access
ISSN: 2329-9495
ISSN: 2329-9495
Research Article - (2018) Volume 6, Issue 2
It is well known that because of turbulence flow and shear stress, bifurcation sites of coronary arteries are vulnerable to atherosclerotic disease. Bifurcation lesions comprise 15% to 20% of all coronary lesions. Bifurcation lesions are treated by either using provisional or double stent technique. The main drawback of provisional stenting is side branch occlusion. We aimed to investigate the predictors of side branch occlusion in provisional stenting technique. We enrolled 803 patients (231 female, 572 male, average age 60.5 ± 12.0) whose bifurcation coronary lesions treated by provisional stenting in Adana Numune Education and Training Centre. Demographic, angiographic and interventional data’s are recorded. 182 patients (22.7%) admitted to hospital with stable angina and 621 (77.3%) with acute coronary syndrome (or unstable angina). 582 (72.5%) patients had left anterior descending artery, 166 (20.7%), circumflex and 55 (6.8%) right coronary artery as the culprit vessel. Side branch occlusion occurred in 52 patients (6.5%). Need for side branch intervention occurred in 160 patients. The predictors of need for side branch intervention were, multivessel disease, type of main branch stent, oversize of stent, presence of side branch disease before intervention, TIMI frame count (TFC) and the alpha angle. In conclusion multivessel disease, type of main branch stent, oversize of stent, presence of side branch disease before intervention, TIMI frame count (TFC) and the alpha angle were independent predictors of need for side branch intervention.
Keywords: Bifurcation lesions, Provisional stenting, Side branch occlusion
It is known that atherosclerosis is common due to increased turbulence and high wall stress in bifurcation regions. Bifurcation lesions constitute 15% to 20% of all coronary lesions [1]. Percutaneous coronary intervention (PCI) techniques for bifurcation lesions are more complex than those of nonbifurcated procedures and therefore have low success rates and high restenosis rates [2]. In the studies performed, single stenting techniques many studies have shown that the long-term outcome is better [3]. In addition, provisional stenting is a less complicated and easier procedure because of the lower number of major cardiac events, radiation exposure during the procedure, and the relatively low amount of contrast material used. The greatest disadvantage of the proximal stenting technique is side branch loss and reported incidence rates of 15% to 41%. The most frequent causes of minor branch loss are plate and carina shift [4,5]. All attempts to be made after minor branch loss make the operation complex. While small side branch loss can be easily tolerated, large side branch loss can cause major complications. Long-term side branch loss may cause Myocardial Infarction and hemodynamic impairment during the procedure [6,7]. Our aim in this study is to investigate the determinants of side branch loss in patients undergoing provisional stenting.
Study populations
In this study patient selected retrospectively from bifurcation lesions treated with provisional technique between 2012 and 2013 in Adana Numune Training and Research Hospital Cardiology clinic. A total of 803 patients (572 males, 231 females, mean age 60.5 years ± 12.3 years) were included in the study. Patients with side branch diameter <2 mm, previous stent implantation, coronary by-pass, and double stenting were excluded. Our working protocol has been approved and approved by the local ethics committee. Before angiography in our clinic informed consent was obtained routinely that all patients accepted the procedure.
Coronary angiographic assessment
Patients with percutaneous intervention were selected as patients with bifurcation lesions and provisional stented. Coronary angiography was performed in our clinic using standard arterial angiography techniques with Siemens (nAxiom Sensis XP Berlin, German) and Toshiba (Infinix CSI Tokyo, Japan) devices used in the catheterization laboratory.
Coronary lesions were evaluated by at least two experienced cardiologists. Patients with a stenosis of more than 70% in the left main coronary artery and/or other coronary arteries (LAD, Cx, RCA and IMA) were accepted as critical vascular disease. Patients with ≥ 70% stenosis (≥ 50% for LMCA) in two or more vessels were considered multivessel disease. Morphological evaluation of bifurcation lesions was done according to MEDINA classification. Angle of bifurcation without main coronary artery is defined by the European Bifurcation club: angle A (proximal bifurcation angle) angle between proximal main branch and side branch, angle B (distal bifurcation angle) angle between distal main branch and side branch, angle C is main branch proximal and the angle between the distal and the distal (Figure 1). The coronary angiography is performed by monitoring the coronary arteries, the number of critical vessels, the presence of critical vessels, the location of the responsible bifurcation lesion, the percentage of lesion, the length of the lesion, the characteristics of the lesion, the major and minor branch lesion fractions, diameter, initial Synergy between PCI with TAXUS ™ and Cardiac Surgery (SYNTAX) score, angle between main branch and side branch, initial Thrombolysis in Myocardial Infarction (TIMI) score, initial TIMI cross section number (TFC), and whether the lesion was thrombotic or not. In addition, bifurcation angles were recorded with major and/or side branch stenosis fractions.
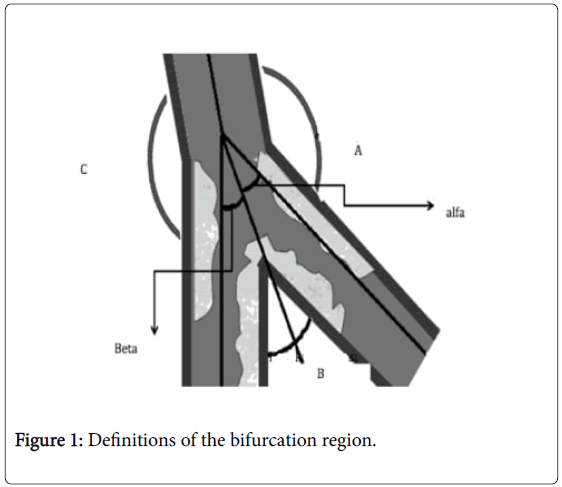
Figure 1: Definitions of the bifurcation region.
Percutaneous coronary intervention
All coronary angiographic procedures and percutaneous coronary interventions were performed by standard methods with a femoral percutaneous approach by interventional cardiologists with ≥ 75 interventional experiences per year.
All patients were given 300 mg aspirin and 600 mg clopidogrel before the procedure. Patients in need were given tirofiban infusions for 24 hours at a dose of 10 μg/kg during the procedure and 0.15 μg/ kg / min after the procedure. 10,000 units of IV heparin were made during the procedure. None of the patients received thrombolytic therapy before or after the procedure. After the procedure, all the patients were followed up in the coronary intensive care unit until they were stabilized. Patient’s information was handled separately. Patient's CD's and operation reports were examined and the results of tirofiban use, number of stents used, predilatation made before stenting, main stent applied stent, dilatation of stent, major stent length and diameter, applied stent exit atmosphere and coronary complications were recorded.
Side branch lesion rates, major branch and side branch TIMI flow grades were recorded after stenting. Side branch loss determined to be
Statistical analysis
All analyses were performed using SPSS 20.0 (Chicago, IL, USA) statistical software package. Continuous variables in group data were expressed as mean ± standard deviation (mean ± SD). Categorical variables were given by number and percentage. When comparing categorical variables, ''chi-square'' test was used. Comparisons of continuous variables were made with the Student-T test. Statistical significance was accepted as p<0.005.
Clinical features of patients
231 (28.8%) of the patients were female and 572 (71.2%) were male and the mean age was 60.5 ± 12.0. Stable angina pectoris (SAP) was found in 182 patients (22.7%), unstable angina pectoris (USAP) in 135 patients (16.8%), 161 (20%) non ST segment elevation Myocardial Infarction (NSTMI) acute anterior Myocardial Infarction (31%), and acute inferior Myocardial Infarction (76) (9.5%).
Angiographic characteristics of patients
LAD was found in 582 (72.5%) of 803, CX in 166 (20.7%) and RCA as a responsible lesion in 55 (6.8%). Of these patients, 477 (59.4%) were single vessels, 230 (28.6%) were two vessels and 96 (12%) were three vessel patients. The initial SYNTAX score average was calculated as 14 ± 7.5. The mean initial TIMI was 2 ± 1.3. Main branch-side branch angle (A) 138.9 ± 30.1, bifurcation angle (B) 66.4 ± 19.5, main branch-major branch angle (C) 154.4 ± 28.2, carina angle alpha) of 37.2 ± 14.7, beta angle of 66.4 ± 19.5. Proximal diameter of main branch was calculated as 3.2 ± 0.47, main branch distal diameter 2.98 ± 0.42 and side branch diameter 2.39 ± 0.3. Main branch proximal lesion was 58.4 ± 43.4 and main branch distal lesion was 79.5 ± 30.9. Patients according to Medina classification 0.1.0. 271 (33.7%), 0.11. 11 (1.4%), 1.1.1. 27 (3.4%), 1.01. 5 (0.6%), 1.1.0. 395 (49.2%), 1.0.0. 94 (11.7%). Four of the responsible lesions (0.5%) were tortious, 5 (0.6%) were calcific, 224 (27.9%) were total occlusion, 315 (39.2%) were thrombotic and 1 (0.1%) ectasia.
Percutaneous coronary intervention information
803 patients had TIMI 3, 29 (53.6), TIMI 2, 9 (1.1%) and TIMI 1 and 4 (0.5%) TIMI was assessed as 0. Tirofiban infusion was initiated in 682 (84%) of these patients. Forty-two patients (56.3%) were predilated before stenting. Predilatation balloon was recorded as 1.86 ± 0.36 diameter, 16.1 ± 3.57 length average. Only one of the patients had no stenting after the balloon. 617 (76.8%) patients had bare metal stents, 185 (23%) patients had drug-coated stents. The brands of the inserted stents were liberty 617 (76.8%), promus 67 (8.3%), coracto 54 (6.7%), endeavor 11 (1.4%), bioMatrix 40 (5%). The bare metal stent length of the applied stents was 19.6 ± 5.9, the diameter was 3.1 ± 0.4 and the atmospheric pressure was 12.7 ± 2.2. The drug-coated stent length was recorded as 23.9 ± 6.2, diameter 2.87 ± 0.27 and atmospheric pressure 13 ± 2.3. After the stenting, the side branch TIMI current was TIMI 0 20 (2.5%), TIMI 1 16 (2%), TIMI 2 16 (2%) and TIMI 3 751 (93.5%).
During the procedure, 397 (49.4%) stents were dilated too much. 160 (19.9%) patients required side branch intervention. In 68 (8.5%) of these patients permanent side branch loss occurred, in 92 (11.5%) temporary side branch loss occurred.
Parameters related to the need for side branch interference
Side branch loss was seen in 52 patients; 20 patients had TIMI 0, 16 patients had TIMI 1, 16 patients had TIMI 2 flow. 160 (19.9%) of 803 patients required side branch intervention. None of our patients had side branch dissections. After the main branch stenting, the side branches were TIMI 0 20, TIMI 1 16, TIMI 2 16 patients. All patients with minor branch involvement had >70% lesion. There was no difference between the two groups in terms of age, gender, and admission to the hospital when the patients were classified according to need of side branch intervention after the procedure.
In patients with angiographic characteristics, side branch intervention is classified as needing classifying MEDINA classification 1.1.0. 86 (53.8%) patients were found to have more proximal and distal lesions in the patient group (p<0.001) (p=0.016-0.029). The preprocedural side branch lesion presence was found to be greater in the side branch requiring intervention (p=<0.001). The percentage of proximal and distal lesions of the main branch was high in the group requiring intervention (p=0.007-0.029). The percentage of side branch lesions before the procedure was significant in the group requiring intervention (p=<0.001). The baseline TFC value was significantly lower in those requiring side branch intervention (p=0.018). In the group requiring side branch intervention, A angle was higher (p=<0.001), B angle (p=<0.001) and alpha angle (p=<0.001) were lower. The diameter of the main branch distal vessels was smaller in the group requiring side branch intervention (p=0.026) (Table 1).
| Variable | Side Branch Intervention Needed | Side Branch Intervention Needed | P |
|---|---|---|---|
| (+) | (-) | ||
| -160 | -643 | ||
| Medina Classification | <0.001 | ||
| 0.1.0. | 39 (24.4) | 232 (36.1) | |
| 0.1.1. | 4 (2.5) | 7 (1.1) | |
| 1.0.0. | 9 (5.6) | 85 (13.2) | |
| 1.0.1. | 2 (1.2) | 3 (0.5) | |
| 1.1.0. | 86 (53.8) | 309 (48.1) | |
| 1.1.1. | 20 (12.5) | 7 (1.1) | |
| Number of Coronary Artery with Lession | 0.031 | ||
| 1 | 112 (70) | 365 (56.8) | |
| 2 | 29 (18.1) | 201 (31.3) | |
| 3 | 19 (11.9) | 77 (12) | |
| Before Intervention TIMI | 0.118 | ||
| 0 | 51 (31.9) | 176 (27.4) | |
| 1 | 9 (5.6) | 23 (3.6) | |
| 2 | 8 (5) | 26 (4) | |
| 3 | 92 (57.5) | 418 (65) | |
| Thrombosis | 0.36 | ||
| (-) | 92 (57.5) | 396 (61.6) | |
| (+) | 68 (42.5) | 247 (38.4) | |
| Proximal Main Artery Lession | |||
| (-) | 43 (26.9) | 238 (37) | |
| (+) | 117 (73.1) | 405 (63) | |
| Distal Main Artery Lesion | 0.029 | ||
| (-) | 11 (6.9) | 84 (13.1) | |
| (+) | 149 (93.1) | 559 (86.9) | |
| Side Branch Lession | <0.001 | ||
| (-) | 134 (83.8) | 623 (97.3) | |
| (+) | 26 (16.2) | 17 (2.7) | |
| Proximal Main Artery Lession Percentage | 66.3 ± 40.3 | 56.4 ± 44 | 0.007 |
| Distal Main Artery Lession Percentage | 83.6 ± 24.9 | 78.5 ± 32.1 | 0.029 |
| Side Branch Lession Before intervention | 24.5 ± 28.7 | 9.2 ± 17.3 | 0 |
| Before Intervention Syntax | 14.5 ± 7.2 | 13.9 ± 7.58 | 0.363 |
| Before Intervention TFC | 25 ± 13.8 | 21.6 ± 10.8 | 0.018 |
| Angle A | 147.2 ± 27.8 | 136.9 ± 30.3 | 0 |
| Angle B | 60.4 ± 17.8 | 68 ± 19.6 | 0 |
| Angle Alpha | 32.4 ± 11.7 | 38.4 ± 15.1 | 0 |
| Angle Beta | 27.9 ± 11.05 | 29.5 ± 10.3 | 0.09 |
| Angle C | 152.2 ± 29.7 | 154.9 ± 27.8 | 0.294 |
| Proximal Main Artery Diameter | 3.21 ± 0.46 | 3.25 ± 0.48 | 0.34 |
| Distal Main Artery Diameter | 2.92 ± 0.36 | 2.99 ± 0.43 | 0.026 |
| Side Branch Diamater | 2.42 ± 0.34 | 2.39 ± 0.30 | 0.26 |
Table 1: Angiographic features according to the need for side branch.
When the patients' percutaneous coronary intervention information was separated according to the need for side branch intervention, the coronary artery to be operated was the most LAD and the most required intervention was in LAD (p=0.04) (Table 2).
| Variable | Side Branch Intervention Needed | Side Branch Intervention Needed | P |
|---|---|---|---|
| (+) | (-) | ||
| -160 | -643 | ||
| Intervention Coronary Artery | 0.04 | ||
| LAD | 125 (78.1) | 457 (71.1) | |
| CX | 29 (18.1) | 137 (21.3) | |
| RCA | 6 (3.8) | 49 (7.6) | |
| After Intervention | 0.004 | ||
| 0 | 3 (1.9) | 1 (0.2) | |
| 1 | 4 (2.5) | 5 (0.8) | |
| 2 | 6 (3.8) | 23 (3.6) | |
| 3 | 147 (91.9) | 614 (95.5) | |
| Tirofiban | 0.035 | ||
| (-) | 127 (79.4) | 555 (86.3) | |
| (+) | 33 (20.6) | 88 (13.7) | |
| Predilatatıon | 0.21 | ||
| (-) | 83 (51.9) | 369 (57.4) | |
| (+) | 77 (48.1) | 274 (42.6) | |
| Main Artery Stent | 0.009 | ||
| BARE | 110 (68.8) | 507 (79.0) | |
| DES | 50 (31.2) | 135 (21.0) | |
| Main Artery Stent | 0.07 | ||
| Liberte | 110 (68.8) | 507 (79) | |
| Promus | 23 (14.4) | 44 (6.9) | |
| Coracto | 11 (6.9) | 43 (6.7) | |
| Endeavor | 2 (1.2) | 9 (1.4) | |
| Biomatrix | 11 (6.9) | 29 (4.5) | |
| Xience | 3 (1.9) | 10 (1.6) | |
| Overdilatatıon of Stent | <0.001 | ||
| (-) | 33 (20.6) | 372 (57.9) | |
| (+) | 127 (79.4) | 270 (42.1) | |
| Main Artery Stent | 20.8 ± 6.1 | 20.5 ± 6.3 | 0.591 |
| Main Artery Stent Diameter | 3.05 ± 0.36 | 3.09 ± 0.39 | 0.301 |
Table 2: Percutaneous coronary intervention information according to the need for side branch intervention.
The TIMI 3 flow rate in the main branch was lower in the group requiring side branch intervention (p=0.004). The use of tirofiban (p=0.035), drug-coated stent (p=0.009) and stent overdilatation were more frequent in patients requiring side branch intervention (p=<0.001).
Significant parameters were multivessel lesion (OR: 0,589 [0.393-0.881 95% CI] p=0.01) when analysed with bivariate and multivariate analysis, post-treatment main vessel TIMI (OR: 0.373 [0.155-0.899 95% CI] (OR: 0.169 [0.096-0.300 95% CI] p: <0.001), the main branch stent type (OR: 0.530 [0.310-0.906 95% CI] (OR: 1.029 [1.017-1.042% 95 CI] p: <0.001), initial TFC (OR: 0.145 [0.026-0.800 95% CI] p=0.027), pre-procedural side branch lesion [1.008-1.049% 95 CI] and alpha angle (OR: 0.974 [0.954-0.994 95% CI] p=0.010) were associated with the need for side branch stenting (Table 3).
| Bivariable | Multivariable | p | |||
|---|---|---|---|---|---|
| R | p | Odds ratio | 95% CI | ||
| Medina | 0.023 | 0.518 | - | - | - |
| Intervention coronary artery | -0.072 | 0.04 | - | - | - |
| Multivessel disease | -0.076 | 0.031 | 0.589 | 0.393-0.881 | 0.01 |
| After intervention TIMI | -0.101 | 0.004 | 0.373 | 0.155-0.899 | 0.028 |
| Tirofiban | 0.077 | 0.028 | |||
| Main artery stent | 0.097 | 0.006 | 0.53 | 0.310-0.906 | 0.02 |
| Main artery stent brand | 0.063 | 0.077 | - | - | - |
| Overdilatation of stent | 0.298 | <0.001 | 0.169 | 0.096-0.300 | <0.001 |
| Proximal main artery lession | 0.085 | 0.016 | - | - | - |
| Distal main artery lession | 0.077 | 0.03 | 0.145 | 0.026-0.800 | 0.027 |
| Side branch lession | 0.241 | <0.001 | - | - | - |
| Before intervention side branch lession | 0.291 | <0.001 | 1,029 | 1.017-1.042 | <0.001 |
| Before intervention TFC | 0.116 | 0.005 | 1,028 | 1.008-1.049 | 0.005 |
| Angle A | 0.137 | <0.001 | - | - | - |
| Angle B | -0.155 | <0.001 | - | - | - |
| Angle alpha | -0.162 | <0.001 | 0.974 | 0.954-0.994 | 0.01 |
| Angle beta | -0.061 | 0.085 | - | - | - |
| Distal main artery diameter | -0.07 | 0.046 | - | - | - |
Table 3: Parameters that determine the need for side branch intervention.
803 patients with bifurcation who were treated with the provisional method were included. 182 (22.7%) of the patients were treated with SAP and 621 (77.3%) with AKS. The most frequent diagnosis in patients was acute anterior myocardial infarction. In 52 of the patients, side branch loss occurred. All patients with minor branch involvement had 70% lesion. Patients were classified as requiring or not requiring side branch intervention. Patients who need side branch intervention were significantly more likely to have multiple vascular diseases, major TIMI, major branch stent, major branch distal lesion presence, initial TFC, alpha angle, over-dilatation.
There is no ideal method for stenting coronary bifurcation lesions. Until now, there are a lot of randomized and nonrandomized studies on this subject. In the NORDIC bifurcation study, only 202 main branches and 202 side branches and main branch interventions were conducted. According to the results, there was no difference between the provisional and double-stenting groups in terms of death, myocardial infarction, target vessel revascularization, and stent thrombosis [8]. In CACTUS study, 177 crushes and 173 patients were provisionally stented. In the study, primary endpoints (death, Myocardial Infarction, revascularization) were equally found in stenting patients with provisional half crush method [9]. A total of 498 patients were included in the BBC ONE study, 249 patients with simple stenting and 249 patients with complex stenting (crush or culottte). Double stenting techniques (crush or culottes) were compared with the provisional method. In this study, the primary outcome point (death, Myocardial Infarction and target vessel revascularization) was lower in the provisional group.
Myocardial Infarction was significantly higher in the crush or culotte group [10]. In the DKCRUSH-II study, 185 patients were treated with PS and 185 patients were treated with DK. Transaction success between the two groups, major cardiac adverse events, and stent thrombosis was equally found. Lesion revascularization difference between the DK-treated group and the PS-treated group was less (4.3% vs. 13%, p=0.005). Coronary vessel revascularization was also found to be more in the PS group. Major cardiac adverse events were found to be the same in both groups. There was no difference between the two groups in stent thrombosis [3]. In all these studies, the European Bifurcation Club suggested bifurcation lesions as the first choice in stenting as a provisional approach. The European Society for Cardiology (ESC) 2014 recommends a provisional method of class IIa as a stenting technique for bifurcation lesions in the myocardial revascularization guide of 2014, in the presence of a large osteal lesion and a lateral branch lesion >3 mm long.
Compared to provisional stenting versus double stenting, it was observed that undesired cardiovascular events were few, the duration of the procedure was short, and the amount of contrast used was low [11]. The most important complication of the proximal stent is side branch loss. The incidence of side branch loss is reported between 12-41 [4,5]. In our study this rate was found to be 6.5%. In case of side branch loss, the side branch should be lumped again and the side balloon/stent application should be done. However, side branches cannot be rewired or some do not pass balloons or stents. In cases where side branch current cannot be achieved in this way, chest pain, Myocardial Infarction or hemodynamic disorder can occur especially in developed side branch lesions. There are many reasons for the loss of side branches; plaque shift, carina shift, spasm in the side branch ostium, dissection due to barotrauma caused by balloon, and prolapse of the main branch stent in the side branch lumen [12-15].
Predicting side branch loss and using side branch protection methods (balloon protection or elective double stent) can provide better results. The patients with multivessel, major branch stent type, major branch distal lesion presence, initial TFC value, alpha angle, over-dilatation of stent and presence of side branch lesion before treatment were found to be independent determinants of disease. In our study, the presence of a critical lesion before intervention in the side branch was identified as an important factor that increased the need for side branch intervention. In a study conducted by Aliabadi and colleagues, >50% lesion presence increased side branch loss in side branch [6] Kralev and colleagues have shown that side branch osteal lesion presence in patients with ST-elevation patients increases the need for side branch intervention [15].
The presence of lesion in the side branch before main coronary intervention increased the need for side branch intervention in COBIS II (COronary BIfurcation Stenting) study and in our study [16]. Carina angle (alpha) was associated with side branch loss, as in most studies. Vassilev et al. [17] found that the carina angle was an important factor [17]. The study of Kane and his colleagues in patients with left main coronary artery stenosis with crossover technique showed the importance of carina angle [17,18]. The COBIS II study showed that the carina angle did not affect the final TIMI flow [16]. In the COBIS study in the small carina angle group no significant difference was found between the major cardiac events and the target lesion revascularization despite the need for side branch stenting and final kissing balloon technique [19]. In the IVUS (intravascular ultrasound study) study performed by Xu et al. [20] although the carina angle was associated with carina shift were found to be irrelevant.
We think that there is more risk of carina shift in the smaller carina angles and accordingly we are thinking about the risk of side branch loss. In our study, we found that the need for side branch stenting was increased in the use of drug-coated stents. We think that this is due to the fact that the use of drug-coated stent is much more complex than that of stent technology.
One of the important factors is over-dilatation of the stent in the main branch. According to Murray's law, the main branch proximal at the coronary bifurcation is always large main branch distally and side branch. European Bifurcation Club proposes that the stent diameter be selected according to the distal main branch in the provisional method and the POT (Proximal Optimization Technique) in the proximal branch. Selection of stent according to proximal main branch diameter according to distal main branch diameter carina slides side to side. We also found that stent over-dilatation in our study was a side-branch loss risk. Another consequence of the IVUS study of Xu et al. [20] was found to be related to the need for atmospheric side branch intervention from the distal main stent [20].
In the case of proximal lesions in bifurcation lesions, there is a hypothesis of "snow plow" effect and plaque side slipping after the main branch stenting. As another consequence of COBIS II trial, proximal lesion increased the need for side branch stenting. According to the study of Ghayemian et al. [21] proximal lesion rate in the main branch affects the branch loss [21]. side branch intervention was more which had proximal main artery lesion.
• A total of 803 patients were enrolled, 231 of whom were female (28.8%) and 572 (71.2%) were male.
• 182 (22.7%) patients were treated with stable angina pectoris (SAP) and 621 (77.3%) with acute coronary syndrome (ACS) diagnosis.
• In patients with multiple vascular diseases, the need for side branch intervention was increased.
• The application of main drug-coated stent increased the need for side branch intervention.
• Main branch distal lesion presence increased the need for side branches intervention.
• Since the initial TFC is low, the demand for side branch intervention is increased.
• The small size of the carina angle increased the need for side branch intervention.
• Stent overdilatation increased the need for side branch intervention.
• Side branch lesion increased the need for side branch intervention before the procedure.