Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Case Report - (2014) Volume 4, Issue 3
Introduction: Typically found in young women, solid pseudopapillary tumors of the pancreas (SPTP) are part of the differential diagnosis for solid and cystic neoplasms of the pancreas. SPTP may cause diagnostic confusion when presenting with massive cystic degeneration.
Case Report: A 59 year-old woman undergoing surveillance PET-CT was found to have a 9 cm, calcified, complex cyst arising in the pancreatic tail. Endoscopic ultrasound, as well as cytology and fluid analysis from fine needle aspiration findings were thought to be consistent with pancreatic pseudocyst; however, after referral to a specialty surgical clinic, resection was offered because the unusual appearance and presentation of the pseudocyst triggered concern for an underlying neoplasm. After distal pancreatectomy with splenectomy, histologic examination of the cyst revealed SPTP with necrosis and no evidence of pancreatic pseudocyst.
Discussion: SPTP may be confused for pancreatic pseudocyst when significant tumor necrosis and cystic degeneration has occurred. Clinicians evaluating pancreas cysts must keep a high index of suspicion for cystic neoplasm particularly when the history lacks the common causes of pancreatic pseudocyst.
<Keywords: Cystic neoplasm of the pancreas, Solid pseudopapillary tumor of the pancreas
Solid pseudopapillary tumor of the pancreas (SPTP) constitutes less than 10% of cystic neoplasms of the pancreas [1]. These infrequent pancreatic tumors usually are identified as part of the evaluation of nonspecific abdominal complaints or are incidental imaging findings. SPTP may give the appearance of a solid mass on axial imaging, but when significant tumor necrosis occurs, SPTP can appear as cystic pancreatic neoplasms. Cystic degeneration of SPTP can complicate identification of these lesions [2,3].
The nature of a pancreas cyst governs recommendations for definitive treatment, prognosis, and the need for long-term surveillance [1]. Axial imaging and endoscopic ultrasound with fine needle aspiration (EUS/FNA) are the mainstay diagnostic modalities for determining the etiology of a pancreas cyst preoperatively [4]. Many cystic lesions of the pancreas are pseudocysts while most of the remainder are neoplastic in nature [5]. The treatment and outcome of pseudocysts may diverge considerably from neoplastic lesions. It is desirable to define the nature of the cyst in the least invasive manner so that the appropriate treatment scheme may be applied. We report a case of SPTP with massive cystic degeneration which illustrates the potential diagnostic challenge this lesions presents when confused for pancreatic pseudocyst.
A 59-year-old woman previously treated for squamous cell carcinoma of the tongue underwent a Positron Emission Tomography-Computed Tomography (PET-CT) for cancer surveillance which revealed a large (9 x 7 cm), non-PET avid, complex, calcified cyst in the tail of the pancreas (Figure 1a).
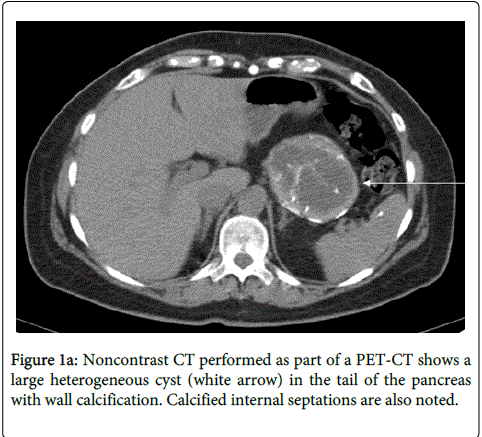
Figure 1a: Noncontrast CT performed as part of a PET-CT shows a large heterogeneous cyst (white arrow) in the tail of the pancreas with wall calcification. Calcified internal septations are also noted.
The radiology interpretation was a pancreatic pseudocyst or, less likely, a splenic artery aneurysm. Her oncologist referred her to a vascular surgeon for evaluation of a splenic artery aneurysm. CT imaging with IV contrast eliminated the possibility of a splenic artery aneurysm (Figure 1b)
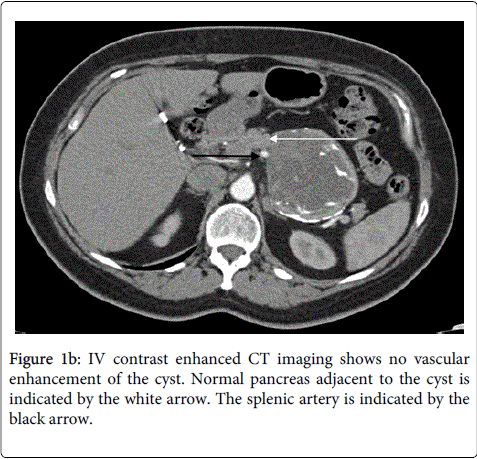
Figure 1b: IV contrast enhanced CT imaging shows no vascular enhancement of the cyst. Normal pancreas adjacent to the cyst is indicated by the white arrow. The splenic artery is indicated by the black arrow.
Subsequently, she was referred for advanced endoscopy to characterize the cyst. EUS revealed a large cystic pancreatic mass with heterogeneous fluid and debris. Dark brown, turbid fluid was aspirated. Analysis of the fluid revealed a fluid amylase level of 51 Units/L and CEA 0.82 mg/mL. Cytology showed histiocytes, debris and a group of reactive glandular cells. After this, she was referred to a general surgeon who was uncomfortable treating this patient and so she was referred to our specialty surgical clinic for definitive evaluation and treatment.
The patient had no abdominal complaints referable to the cystic pancreatic mass. Cholecystitis, cholelithiasis, pancreatitis, abdominal trauma, or excessive alcohol use were all absent from her history. Physical examination of the abdomen was unremarkable. Basic chemistry and blood counts were normal. Serum pancreas enzymes and pancreas tumor markers were not tested because of the lack of a definitive cancer diagnosis. The wall calcifications and lack of antecedent history gave concern for an underlying pancreatic neoplasm and surgical resection was recommended. A distal pancreatectomy with splenectomy was performed. Her surgery and post-operative course were uncomplicated. There is no sign of recurrence two years after resection
Histological evaluation of the pancreas mass revealed a SPTP characterized by abundant necrosis with cystic wall calcifications that on gross examination simulated a pseudocyst. Microscopically, the tumor was composed of well-differentiated cells with no mitotic activity arising in a background of hyalinized eosinophilic matrix. Immunohistochemical stains were positive CD10, CD56, alpha-1 anti-trypsin, and progesterone receptor, and negative for chromogranin, insulin, glucagon, and somatostatin. Margins were free of tumor and four regional lymph nodes were free of metastases.
Solid pseudopapillary tumor of the pancreas (SPTP) occurs most frequently in young adults and affects women far more often than men [6]. SPTP arise with even distribution throughout the pancreatic parenchyma [7]. Patients with SPTPs typically present with symptoms of abdominal pain, abdominal mass, or the tumor may be asymptomatic. In the latter case, SPTP are recognized as an incidental imaging finding [7]. SPTP are low grade neoplasms, thus, despite occasional reports of metastatic disease, surgical resection usually portends a good prognosis [7,8].
CT and MRI are the most common initial means of identifying and evaluating SPTP. SPTP will generally be seen as a well-demarcated mass with a thickened wall. Calcification may be present but is not common [9]. Tumor size and the amount of degeneration influence imaging appearance. Smaller SPTPs may appear as a solid mass, while larger tumors may appear as cystic neoplasms due to necrotic or hemorrhagic components [9]. A non-enhancing mass with complex central necrosis is most common [10]. As with other solid pancreatic neoplasms, cystic degeneration in SPTP may be massive [2,3]. When massive cystic degeneration occurs, the diagnosis of SPTP may be difficult to determine preoperatively [11].
As in the case presented here, SPTP with massive cystic degeneration may be initially identified as a pancreatic pseudocyst [2,3]. Cystic degeneration is part of the disease process with SPTP [6] and can contribute to large size at presentation [12]. When SPTP undergo degeneration, they do not form true cysts, but instead have nonepithelial lined cavities filled with debris and fluid [6,13]. Pseudocysts are also nonepithelial lined cavities filled with debris and fluid, hence SPTP with massive cystic degeneration may be difficult to distinguish from pancreatic pseudocyst preoperatively. Unlike pancreatic pseudocyst which may communicate with the pancreatic duct, SPTP should not communicate with the pancreatic duct. EUS-guided FNA with cytological examination has been used to diagnose SPTPs that cannot be differentiated from other cystic lesions of the pancreas by CT or MRI; however in the setting of a large amount of necrosis sampling error may decrease the accuracy of the results [8]
The noncystic component of SPTP is microscopically characterized by areas of uniform polygonal cells arranged as papillary cords and sheets of cells surrounding capillary-sized vessels alternating with cystic spaces [9]. The immunohistochemical (IHC) staining signature is important to make the diagnosis of SPTP and can be key to identifying SPTP when the tumor has undergone massive cystic degeneration [14]. Positive nuclear ß-catenin staining and loss of expression of membrane-bound E-cadherin has been identified in the majority of SPTPs [15]. Diagnostic IHC may include positive CD10, CD56, alpha-1 antitrypsin, progesterone receptor, and vimentin, with negative chromogranin, keratin, and variable synaptophysin staining [8,9].
Treatment of SPTP necessitates complete tumor resection with reported approaches including enucleation and partial pancreatectomy. Tumor size and location within the pancreas are important considerations in the approach to resection. Some authors suggest enucleation may undertreat this tumor with malignant potential and one can find recommendations against enucleation for SPTP in the literature [9]. With surgical resection, patients with SPTPs have excellent long-term survival [7]. Although SPTPs generally have low malignant potential, as many as 19% of these tumors have locally invaded or metastasized at the time of presentation, with the most common locations of metastasis being the liver, portal vein and spleen [7]. Surgical resection of metastases has been shown to improve survival; however, survival of over 10 years has also been reported in cases with unresectable metastases speaking to the relative indolent nature of the tumor [12,16]
In this report, we present a case of SPTP with massive cystic degeneration initially identified as a pancreatic pseudocyst. This case highlights the capacity of SPTP with cystic degeneration to appear as other cystic lesions of the pancreas by axial imaging and FNA with cytology. Complex calcifications, internal septations, and history absent of common etiology for pancreatic pseudocyst raised suspicion of an underlying pancreatic neoplasm in this case. Clinicians must keep a high index of suspicion for underlying tumor when the patient history does not include a common pseudocyst etiology. We recommend referral to a specialty center with experience in evaluation and treatment of pancreas neoplasms when the diagnosis does not match the clinical parameters.