Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Research Article - (2011) Volume 1, Issue 1
Purpose: A retrospective study of 89 hypo-fertile male patients attending for in vitro fertilization was undertaken in order to evaluate possible correlations among sperm DNA damage, sperm analysis parameters and pregnancies.
Methods: Sperm parameters (concentration, normal morphology and multiple anomalies) were evaluated according to the World Health Organization guidelines. DNA damages were simultaneously evaluated on each sperm sample by i) sperm chromatin decondensation test; ii) sperm DNA fragmentation evaluated by Sperm Chromatin Dispersion and Halo sperm Kit; iii) sperm DNA fragmentation evaluated by the Terminal Uridine Nick-End Labelling procedure.
Results: Statistical analysis was performed by using analysis of variance and least squares regression.
The sperm chromatin dispersion and fragmentation assays showed a statistically significant positive correlation (P=0.0017) in all the samples confirming the good efficacy of either of the two tests in detecting sperm DNA damage. Both the two test negatively correlated with normal sperm morphology (P=0.008), however only by using Halo sperm test we obtained a significant correlation with multiple sperm pathological morphologies (P=0.029) and an inverse correlation with pregnancies outcome (P=0.013). No correlation was detected among DNA damages, sperm concentration and chromatin decondensation.
Conclusions: These data suggest a similar efficacy of sperm chromatin dispersion and Terminal Uridine Nick-End Labelling in detecting sperm DNA integrity. Due to the higher sensitivity of Halo test, its prognostic role in the diagnosis of fertilizing ability of a semen sample and possible pregnancy rate is discussed
Keywords: Spermatozoa, Chromatin condensation, DNA fragmentation, TUNEL test, Halo test
It has been documented that almost 50% of the infertility problems are at present attributed to male factors. In IVF centres, potential infertile men are screened for the sperm quality by semen analysis, in particular investigating concentration, motility and morphology according to WHO guidelines [1]. However, at present, these parameters appear to be poor predictors of the fertilization success since infertile men may often show normal semen analysis [2]. For these reasons, it is claimed that, due to poor diagnostic methods and no fully effective infertility treatments, the use of sperm functionality test should be mandatory and routinely associated to conventional semen analysis [3-5].
In the last decades the importance of sperm DNA integrity has been highlighted as a factor which affects the functionality of spermatozoa [6]. In fact, due to the diffuse application of ICSI, it has been stressed that the injection of DNA-damaged spermatozoa may introduce damaged genome into the oocytes with dangerous drawbacks on fertilization, embryonic, foetal and post-natal development [7,8].
Among these, investigating the sperm DNA integrity seems to have important implications for the success of fertilization and the following embryo development [6,9,10].
On these bases, DNA nuclear chromatin decondensation and DNA fragmentation are two kinds of tests for DNA damage indicated as diagnostic tools to predict the fertilizing ability and possibly the pregnancy outcome in many human fertility clinics [11,12].
The compact structure of sperm nuclear chromatin is important for the protection of genetic integrity during transport of the paternal genome through the male and female reproductive tracts. Sperm chromatin is in a highly condensed state prior to fertilization and in vivo decondensation occurs in the oocyte, giving rise to the formation of male pronucleus and the zygote. The chromatin decondensation state is associated with an incorrect sperm maturation during spermiogenesis, when nuclear compaction is caused by a change in nuclear tertiary structure of chromatin due to the substitution of histones with protamines [13,14]. However, recently, our group has also shown a significant impact of cryopreservation on the condensation state of human spermatozoa [15,16] using the nuclear chromatin decondensation test.
Sperm DNA fragmentation is characterized by single- and doublestrand DNA breaks that, by occurring during or after DNA packaging, may overcome the mechanism of DNA repair and successively be delivered to the mature sperm. Defective sperm chromatin packaging, abortive apoptosis and oxidative stress have been suggested among the etiologies of DNA strand breaks [2,17].
Many tests have been developed to detect DNA breaks in the spermatozoa, giving rise to variable but somewhat comparable results [18]. Among the commonly used tests to detect DNA breaks there are Terminal Deoxynucleotidyl Transferase-mediated Nick End Labeling (TUNEL) which is based on a direct assay, and the Sperm Chromatin Dispersion test (SCD), performed with the Halo test based on an indirect assays.
Since the two tests are based on different principles and experimental procedures they may express different sensitivity in the identification of the DNA fragmentation. Furthermore no study has been performed to correlate sperm DNA damage assays and the pregnancies obtained after an in vitro fertilization treatment.
The objective of this study was to correlate the two types of DNA damage evaluated with different methods with some parameters of conventional sperm analysis and the pregnancy outcomes in patients undergoing In Vitro Fertilization (IVF) treatment at the IDF center.
Patients and sperm analyses
A total of 89 male patients were randomly selected and gave their written consent to participate to this study between November 2010 and May 2011 at the IDF centre.
The sperm samples were collected by masturbation in a sterile plastic container after three days of abstinence. Each semen sample was allowed to liquefy for 30 minutes, after that the sample was mixed carefully, divided into four aliquots and simultaneously processed as follows: i) sperm concentration and morphology; ii) nuclear chromatin decondensation test; iii) DNA fragmentation test evaluated by the TUNEL; iv) DNA fragmentation test evaluated by Halo test.
Pregnancies obtained following an IVF treatment by applying only the Intra Cytoplasmic Sperm Injection (ICSI) technique were reported as term delivery of healthy baby at home.
Routine semen analysis
The sperm concentration/ml was determined on the liquefied sample by using the computer-assisted sperm analysis (Sperm Class Analyzer -SCA, Microptic S.L. Spain). Sperm morphology was evaluated by using pre-treated slides Test Simplets (Waldeck, Gmbh, Germany). A total of 100-200 sperm cells were scored for normality according to the Krüger strict criteria [19]. Results were reported according to World Health Organization (WHO) criteria [1].
Nuclear chromatin decondensation test
This test was modified by Franken et al. [20] and expressed as Sperm Decondensation Index (SDI). Briefly, samples were washed twice by centrifugation (1,500 rpm for 5 minutes) in Ham’s F-10 salt solution (PAA laboratories, Gmbh, Austria). The supernatant was removed and the pellet re-suspended in a minimum amount of medium; one drop of resuspended semen was spread on a glass slide previously washed in 70% alcohol and allowed to air-dry. All the smears were fixed in 4% (v/v) buffered glutaraldehyde (Sigma, Italy) for 30 minutes and then rinsed in phosphate buffer solution (PBS, Sigma, Italy) and in distilled water for 20 seconds each. Slides were then allowed to dry at room temperature and stained with 5% (w/v) aqueous Aniline Blue (Sigma, Italy) 5% mixed with 4% acetic acid (pH 3.5) for 15 minutes. Slides were then rinsed in distilled water to remove all the aniline excess and air-dried.
A total of 100 to 200 sperm cells were evaluated by phase contrast microscopy at 1,000 X magnification, and the percentage of stained sperm heads was calculated. Three classes of head staining intensities were noted, namely unstained (pale blue), partially stained (pale and intense blue together) and stained (intense blue). A > 25% threshold value is generally accepted as an indicator of decondensed sperm [21].
Evaluation of sperm DNA fragmentation
TUNEL test: was assayed using In Situ Death Detection Kit (Roche Diagnostic Corp.). A semen aliquot was centrifuged at 1500 rpm at room temperature for 10 minutes. After removal of the seminal plasma, the pellet was suspended in 1 ml of Phosphate Buffer Solution (PBS) 1X and further centrifuged at 1500 rpm at room temperature for 5 minutes. The pellet was suspended in 0.5mL of PBS 1X and one aliquot of 10 μl smeared on a microscope slide and fixed with 4% paraformaldehyde in PBS (pH 7.4) for 1 h at room temperature. After fixation the sample was permeabilized with 0.1% Triton X-100 in 0.1% sodium citrate in PBS 1X for 2 minutes at 4°C, then the cells were incubated with 50 μl of staining solution containing Terminal Deoxytransferase (TdT), for 1 hour at 37°C in the dark. Negative and positive controls were performed, respectively, by omitting the TdT enzyme in accordance with the kit instructions and by preincubating fixed and permeabilized sperm samples with DNase I (40 IU/ml) for 10 minutes at room temperature to produce DNA breaks. Each slide was stained with 200 μl of DAPI (4’,6-diamidino-2-phenylindole that is a DNA-specific probe which forms a fluorescent complex by attaching in the minor grove of A-T rich sequences of DNA) for 10 minutes at room temperature and performed with PBS-glycerol. For microscopic evaluation, the slides were studied in transmitted and fluorescent illumination under the 40X and 100X objective of a Nikon Eclipse E200 microscope. For each slide, about 200 spermatozoa were evaluated and the percentage of fragmented spermatozoa was calculated.
SCD test: The SCD test was performed with Halo test by using the Halosperm kit (Halotech DNA SL, Madrid, Spain). An aliquot of each sperm sample was diluted to 5- 10 million/ml in sperm preparation medium (Medicult, Denmark). Gelled aliquots of low melting-point agarose in Eppendorf tubes are provided in the kit, each 1 to process a semen sample. The Eppendorf tube was placed in a boiling water bath for 5 minutes to melt the agarose, and then in a water bath at 37°C. After 5 minutes 25 μl of the diluted semen sample was added to the Eppendorf tube and mixed with the melted agarose. Twenty microliters of the semen/ agarose mix was pipetted onto an agarose precoated slide (previously kept in the refrigerator at 4°C), provided in the kit, and gently covered with a 22 mm coverslip. The slide was placed on a cold plate in the refrigerator (4°C) for 5 minutes to allow the agarose to produce a microgel entrapping the sperm cells. The coverslip was gently removed and the slide immediately immersed horizontally in an acid solution, previously prepared by mixing 80 μl of HCl from an Eppendorf tube in the kit, with 10 ml of distilled water, and incubated for 7 minutes. The slides were horizontally immersed in 10 ml of the lysing solution for 25 minutes. After washing 5 minutes in a tray with abundant distilled water, the slides were dehydrated in increasing ethanol baths (70%-90%-100%) for 2 minutes each and air dried. The slides were horizontally covered and immediately stained for bright-field microscopy with a mix of Wright’s solution (Merck, Darmstadt, Germany) and phosphate buffer solution (Merck) (1:1) for 10 minutes, with continuous airflow and then briefly washed in tap water and allowed to dry. At least 500 spermatozoa were scored under the 40X and 100 X objectives under bright-field microscopy.
Statistical analysis
Statistical analysis was carried out by using Systat 11.0 release. Before the analyses, percentage values were transformed in arcsin and homogeneity of variances and their normal distribution were tested. Hypothesis testing was performed by parametric tests, which included Linear Regression Analysis (LRA) and Analysis Of Variance (ANOVA), Coefficients of correlation (R) were recorded for each LRA model A probability (P) value of ≤ 0.05 was selected as a criterion for a statistically significant difference; a P value of ≤ 0.001 for high significant difference.
According to Fernandez et al. [22] using the Halo test kit, four types of halos were evaluated by using their own nucleoid as a reference as follows: i) Big halos: those whose halo width is similar or higher than the minor diameter of the core; ii) Medium-size halos: the halo size is between those with high and with very small halo; iii) Small-size halo: the halo width is similar or smaller than one third of the minor diameter of the core and; iv) No halo. The percentage of sperm bearing DNA fragmentation was expressed as DNA Fragmentation Index (DFI) and evaluated as the percentage of small and no halo sperm cells over the total sperm count. (Figure 1)
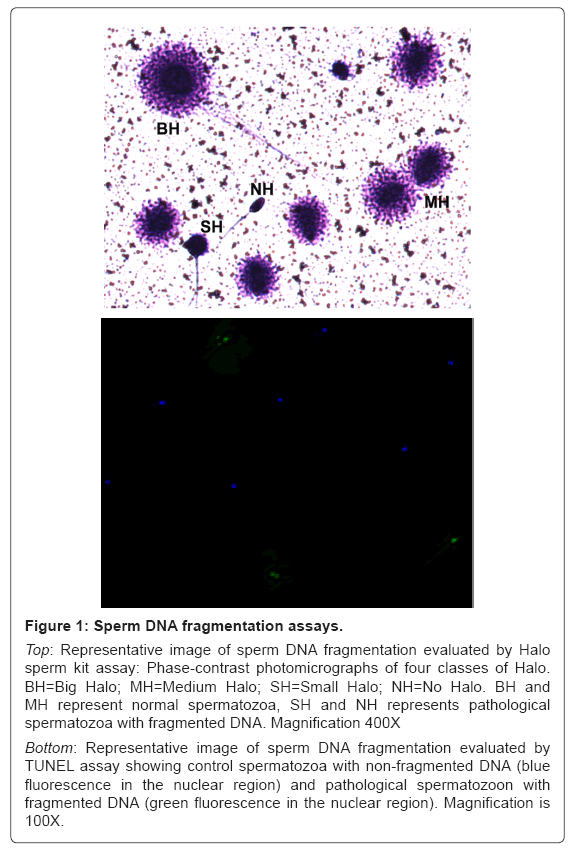
Figure 1: Sperm DNA fragmentation assays.
Top: Representative image of sperm DNA fragmentation evaluated by Halo sperm kit assay: Phase-contrast photomicrographs of four classes of Halo. BH=Big Halo; MH=Medium Halo; SH=Small Halo; NH=No Halo. BH and MH represent normal spermatozoa, SH and NH represents pathological spermatozoa with fragmented DNA. Magnification 400X
Bottom: Representative image of sperm DNA fragmentation evaluated by TUNEL assay showing control spermatozoa with non-fragmented DNA (blue fluorescence in the nuclear region) and pathological spermatozoon with fragmented DNA (green fluorescence in the nuclear region). Magnification is 100X.
By using TUNEL assay the percentage of spermatozoa with fragmented DNA was determined simultaneously by analysing each field using both DAPI filter to count the total number of spermatozoa and using FITC filter. DFI was evaluated as the percentage of spermatozoa with intense green fluorescence representing positive TUNEL cells vs. normal spermatozoa showing blue fluorescence (Figure 1). Sperm nuclear chromatin decondensation rate was calculated as the total of partially stained (pale and intense blue together) and stained (intense blue) cells (Figure 2).
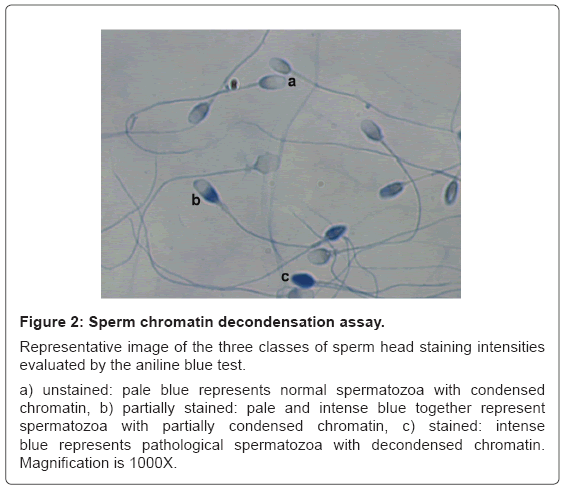
Figure 2: Sperm chromatin decondensation assay.
Representative image of the three classes of sperm head staining intensities evaluated by the aniline blue test.
a) unstained: pale blue represents normal spermatozoa with condensed chromatin, b) partially stained: pale and intense blue together represent spermatozoa with partially condensed chromatin, c) stained: intense blue represents pathological spermatozoa with decondensed chromatin. Magnification is 1000X.
Separate groups of men were divided according to normal and abnormal semen standard parameters (where normal values were: sperm concentration ≥ 20 × 106/ml, morphology ≥ 4 %) [1].
Sperm concentration was evaluated by the SCA, providing an objective and reproducible set of results. Multiple anomalies were considered as the combination of head (large or small, tapered, pyriform, round, acrosome defects, double head), neck and flagellum anomalies.
Out of the 89 sperm samples submitted to simultaneous analysis of concentration/ml; morphology, SDI and DFI, 17 % resulted oligospermic, 39% teratospermic, 19% decondensed, 9% fragmented by TUNEL assay and 11% fragmented by Halo assay. Pregnancies were obtained in 15 % of cases. Percentage of decondensed spermatozoa was calculated as over 25% threshold and fragmented spermatozoa over the 30 % threshold.
Pathological DFI analysed by either TUNEL and Halo techniques was detected in the 3% of samples, nonetheless, a statistically significant positive correlation (R= 0.254; P = 0,017) was determined between the DFI detected by either halo and TUNEL on all the 89 considered samples. When we evaluated the DFI results vs. patients with normal sperm morphology, a significant negative correlation (R= -0.351; P < 0.001) was detected between either Halo or TUNEL determination of DFI. A further correlation (R= 0.233; P = 0.029) is shown by comparing the percentage of multiple anomalies and the DFI but in this case significance was obtained only for Halo test-determined DFI. At last a significant negative correlation (R= -0.264; P= 0.013) was found by comparing the DFI detected only by Halo test and the pregnancies obtained in this group of patients. On the contrary we did not observe any correlation between the DFI measurements performed by the two different assays and sperm concentration or SDI. These results are summarized in table 1.
| Halo vs. TUNEL | R= 0.254 | P= 0.017* | ||
|---|---|---|---|---|
| Halo DFI | TUNEL DFI | |||
| R | P | R | P | |
| Concentration/ml | 0.150 | 0.162 | 0.082 | 0.45 |
| Normal morphology | -0.283 | 0.008** | -0.351 | <0.001** |
| Multiple anomalies | 0.233 | 0.029* | 0.173 | 0.107 |
| Chromatin decondensation | 0.139 | 0.195 | 0.097 | 0.370 |
| Pregnancies | -0.264 | 0.013* | 0.012 | 0.915 |
*marks significant value,
**marks highly significant value.
Table 1: Coefficients of correlation (R) and significant values (P) between sperm DFI evaluated by Halo vs. TUNEL assays, and between Halo/TUNEL vs. sperm parameters, chromatin decondensation and pregnancies.
By comparing the sensitivity of Halo test and that of TUNEL assay in detecting sperm DNA fragmentation, we show a significant inverse correlation with either sperm morphology and the pregnancies obtained in patients undergoing assisted reproduction techniques.
Different assays have been developed to investigate a possible sperm DNA damage to provide additional information on sperm competence. In the last decades, TUNEL assay has become an established method to identify the programmed death (apoptosis) ratio in somatic cells and this property was correlated with those of abnormal sperm cells that have lost their reproductive capability [23]. Subsequently other tests have been developed based on the sperm chromatin dispersion. Among them, the Halo test is a relatively new technique based on the acid incubation and subsequent lysis of the sperm cell that allow the avoidance of complex and expensive instruments as the fluorescence microscope and the flow cytometer necessary for TUNEL evaluation.
Although a recognized threshold value for DFI has not been established yet, in this work we referred to some recent studies that have indicated: i) 30% as the cut off value above that natural pregnancy is not possible to be achieved [3,24] ii) DFI > 30% provides significantly lower embryo implantation rate and pregnancy rate [25]. These data supported also previous statistical studies indicating that the pregnancy rates were lower in case of DFI over 30% [26] and significantly higher in men with DFI below the thresholds of 30% [27].
In this paper we have simultaneously treated the same sperm sample from 89 different males from infertile couples with the two different techniques reporting a significant positive correlation between them. In particular with Halo test we were able to detect more DNA fragmented spermatozoa (2%) with respect to TUNEL assay.
Although contrasting results from the literature criticized the lack of new information [28] and of the statistical rigor [29], for Halo test, our data are in agreement with other authors who found a similar efficacy of both the assays [18] and even a higher sensitivity of Halo test in detecting damaged DNA [30,31].
Although the clinical significance of sperm morphology is still a matter of debate, it has been recently recognized that an accurate definition of morphological anomalies plays a very important role in the determination of male fertility potential [32].
A considerable heterogeneity of studies trying to relate classical semen parameters and the sperm chromatin structure assay exist in literature [33,34], hence of interest is our finding on the relationship between sperm abnormal morphology and DNA fragmentation detected with both the two test. Furthermore in agreement with Daris et al. [35] who found that the percentages of amorphous heads and overall head abnormalities were significantly higher in sperm samples with elevated degree of DNA fragmentation. Of particular interest is the correlation between the DNA fragmentation and multiple anomalies. It has been shown that severe teratospermia due to the presence of different categories of defects, may be attributed to andrological pathologies and/or genetic disorders [36]. The strict correlation found in this study substantiates the need of a correct detection of DNA damage in the sperm population in order to identify possible aetiologies and therapies. Here, when we evaluated the spermatozoa bearing multiple anomalies it resulted that they correlate only with DNA fragmentation identified by Halo test, further confirming the specificity of this test with respect to TUNEL assay.
Similarly to DNA fragmentation, sperm chromatin decondensation test represents a modern tool for the assessment of male subfertility [16,30]. In absence of recognized standard values, some reports established that a normal semen sample generally contains less than 25% stained spermatozoa [37,38] and more recent clinical observations identified threshold values from 28 to over 30%, since no pregnancies were reported following in vitro fertilization and ICSI with semen samples exceeding this percentage [3,24,39,40].
In this study we did not find any correlation between SDI and DFI. This lack of correlation has been also shown by other authors [41,42] suggesting that the two kinds of DNA damage are generated by different etiological pathways leading to abnormal chromatin packaging during sperm maturation process for SDI and to an increased sensitivity to oxidative stress and/or apoptosis for DFI [2,43].
Recent papers show a low DNA fragmentation index associated with a higher pregnancy rate [44] and that sperm DNA damage assessed by the Comet assay has a close inverse relationship with livebirth rates after IVF [45]. Interestingly, in this study we show for the first time a significant inverse relationship between pregnancies and the DNA fragmentation detected only by the Halo test. Due to the recognized need of developing and using tests with reliable prognostic value, the correlation between the Halo test and either abnormal sperm morphology and pregnancies highlights the stronger sensitivity of Halo test, suggesting including it in the routine sperm analysis panel as a complement for the initial diagnosis of male infertility in the clinical practice.
Conventional sperm analysis is traditionally based on the assessment of concentration, motility and morphology of spermatozoa in order to evaluate male infertility.
During the last decade, investigation of sperm DNA integrity has emerged as a new potential biomarker of sperm quality, able to identify male infertility and even to predict pregnancy in IVF program [46].
At present, data on the prognostic value of sperm DNA damage are still controversial but substantially promising, encouraging the andrology laboratories to include DNA integrity assessment as a part of routine semen analysis. In this respect it has also been claimed the need to develop new protocols in order to establish reliable clinical thresholds [46].
In this study we found a correlation between Halo and TUNEL tests in detecting sperm DNA fragmentation. However a significant positive correlation with pathological sperm morphology and negative correlation with the pregnancies obtained in the IVF program was found only with the results obtained by using the Halo test. These data confirm that sperm DNA damage has a negative impact on assisted reproduction treatment outcome and in particular highlight the efficacy of Halo test as a simple and reliable procedure to screen the DNA fragmentation in human spermatozoa.
We thank Prof. Raffaele Boni for statistical analysis and useful comments on the manuscript and Dr. Franco Fulciniti for his help in the English stylization of the manuscript. Dedicated to the dear memory of Prof. Bob Edwards