Andrology-Open Access
Open Access
ISSN: 2167-0250
ISSN: 2167-0250
Research Article - (2015) Volume 4, Issue 1
Almost 15% of infertile males have normal semen parameters and DNA Fragmentation Index (DFI) could be reasonably a valued tool for fertility extrapolation than the conventional semen analysis. To the best of our knowledge, this is the first study to assess the prevalence of high DFI in Saudi infertile men with normal standard semen parameters in order to support the generalizability about sperm DFI as a marker of male infertility. A total of 79 infertile men with normal semen standards were identified (study group). Standard semen analysis and sperm chromatin dispersion were carried out. 33 men (41.8% of the whole study group) had a DFI ≥ 20%; with 19 men (24.1%) (95% CI: 14.67-33.53) had a 20% ≤ DFI<30%, and 14 men (17.7 %) (95% CI: 9.28-26.12) had a DFI ≥ 30%. The mean DFI was 21.14% (±10.26%) with a median of 18.12% [5.09-57.23]. Our findings showed that a considerable proportion of men with normal semen parameters had high sperm DNA damage levels. Thus, the DFI by sperm chromatin dispersion test is essential to explain causes of infertility in cases where semen analysis has not shown any deviation from the norms.
<Keywords: Infertility; SCD test; Semen parameters; Sperm DNA fragmentation
Infertility is defined as the failure to conceive after one year of regular, unprotected intercourse [1]. It affects approximately 15% of all couples seeking to have children. Male factor is evident in about 30% to 50% of clinical infertility cases worldwide [2]. Investigation of the male partner in an infertile couple is primarily based on the routine semen analysis. Poor sperm quality is represented by abnormal semen parameters, including low sperm concentration, poor sperm motility, and abnormal sperm morphology [3]. It has also been reported that sperm concentration, mortality and morphology might be affected by sperm DNA fragmentation [4]. Nevertheless, DNA integrity assessment is not being carried out as a conventional part of semen analysis in the clinical laboratory [2,5]. Recently, the integrity of sperm DNA is being recommended as a new parameter of semen quality and a marker of male infertility [5].
High levels of sperm nuclear DNA have been related to low fertility potential, failure to obtain blastocysts, blockage of embryo development after embryo implantation, increased risk of recurrent miscarriages, reduced chances successful implantation, and negative effect on the health of the offspring [6].
To date, there is no data about the prevalence of high DFI in infertile men from Saudi Arabia. Therefore, the aim of this study was to assess the prevalence of high levels of sperm DNA damage among Saudi infertile men with normal standard semen parameters in order to support the generalizability about sperm DFI as a marker of male infertility.
This is an observational cross-sectional study design for men with normal standard semen parameters presented at Thuriah medical Center, Riyadh, Saudi Arabia between June 2012 and August 2014 for infertility investigation to assess the prevalence of high DNA fragmentation. This study was approved by Thuriah Institutional Review Board that operates according to Declaration of Helsinki and Belmont Report. A written informed consent was obtained from each subject included in this study after a detailed explanation by the principal investigator about the aim and procedure of the study.
The diagnosis of unexplained infertility in men with at least one year of unprotected intercourse without pregnancy was based on the following:
• Normal sperm concentration, motility and morphology according to 2010 World Health Organization (WHO) guidelines [7].
• Ordinary andrological profile (drug abuse, chemo or radiotherapy, no cryptorchidism or other iatrogenic factors).
Seventy nine infertile men with normal semen standards parameters fulfill the inclusion criteria and were considered for final data analysis.
Age, BMI (kg/m2), smoking status (yes/no) and reproductive parameters (primary/secondary) were assessed in addition to sperm concentration (million/ml), motility (%), Morphology (%) and DFI (%).
Semen Analysis
Semen samples were collected by masturbation after an abstinence period of 3-5 days. Semen parameters were scored upon WHO 2010 guidelines [7]. The following cut-off levels were considered normal:
1. Sperm concentration ≥15 million.
2. Sperm motility ≥40% progressive motile and nonprogressively motile sperms.
3. Sperm morphology ≥4% normal forms.
Sperm DNA fragmentation assessment
The sperm DNA damage was evaluated by Sperm Chromatin Dispersion (SCD) test [8] using the Halosperm G2® kit (Halotech, DNA Spain). A sperm sample from each patient containing after dilution 5-20 million spermatozoa per milliliter, then the agarose was liquefied by incubating it in the water bath at 95-100°C for 5 minutes or until the agarose was fully melted and we maintained it in a water bath at 37°C for 5 minutes until the temperature has equilibrated. Next, we transferred 50 μl of the sperm sample to the 100 μl agarose tube and mixed it gently with the pipette and maintained it at 37°C. At that time, we put a drop of 8-9 μl of the cell suspension onto the center of the well and covered it with 22*22 mm cover slides and pressed gently to avoid the air bubbles formation, keeping in mind to held the slide always in a horizontal position.
The slide then was placed on a cold surface (metal pre-cooled at 4°C) and transferred to the fridge at 4°C, for 5 minutes to solidify the agarose. After the solidification of the agarose the coverslide was removed by sliding it off gently, all the processing was performed at a 22°C room temperature).
In the Denaturation step we placed the slide horizontally on the Petri dish and apply the denaturant agent (provided in Halosperm G2® kit) for 7 minutes on the wells and made sure that they were fully immersed.
After removal from this solution, the slide was incubated for 20 minutes lysing solution 1, 4 dithiothreitol (DTT). After rinsing in distilled water for 5 minutes, the slide was dehydrated for 2 minutes each in two concentration of alcohol (70%, and 100% vol.). Then, we allowed them to dry; we processed immediately with staining solution A for 7 minutes then staining solution B for 7 minutes. At least 300 spermatozoa were scored under the Inverted bright-field microscopy for every patient into five groups (Figure 1):
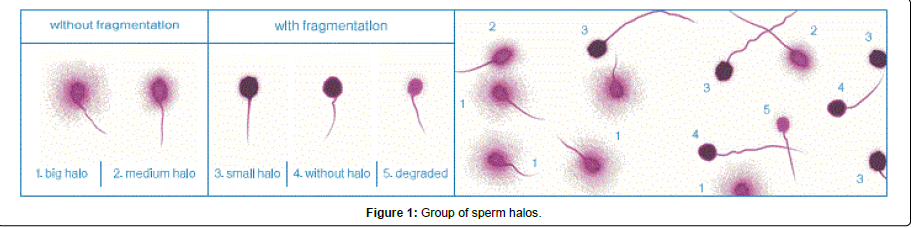
Figure 1: Group of sperm halos.
1. Spermatozoa with large halos: halo width is similar or larger than the minor diameter of the core.
2. Spermatozoa with medium-size halos: halo size is between those with large and very small halo.
3. Spermatozoa with very small-size halo: halo width is similar or smaller than 1/3 of the minor diameter of the core.
4. Spermatozoa without a halo.
5. Spermatozoa without a halo and degraded spermatozoa: no halo and weakly or irregularly stained core is present.
Sperms with big and medium halo without DNA fragmentation were counted as normal sperms, whereas sperms with small halo, without halo and degraded without halo with DNA fragmentation were counted as abnormal sperms [9].
Statistical analysis
Results were expressed as percentage of men with DFI ≥ 20%, 20% ≤ DFI<30% and DFI ≥ 30 respectively in relation to the total number of men with normal semen parameters. The reason behind selecting these DFI cutoffs was based on previous studies using the SCD [10,11]. A 95% confidence interval was estimated for each group.
The additional parameters: sperm concentration, motility, and morphology were expressed as mean (± standard deviation) and median (Minimum-Maximum).While BMI, smoking status and reproductive parameters were showed as numbers (percentage).
Odds ratios of DFI% (<30 and ≥30) in relation to BMI, smoking status and Infertility type were measured. P-values and 95% confidence intervals were calculated.
Final data analysis included seventy nine in fertile Saudi men with normal standard semen parameters in total, 33 men had a DFI ≥ 20% prevalence of 41.8 % (95% CI: 30.9-52.66).As well, 19 men (24.1% of the le study group) (95% CI: 14.67-33.53) had a 20% ≤ DNA fragmentation index (DFI)<30%, and 14 men (17.7 %) (95% CI: 9.28-26.12) had a DFI ≥ 30%. The mean DFI was 21.14% (±10.26%) with a median of 18.12% [5.09-57.23].
Table 1 represents the characteristics of the seventy nine included men with normal standard semen parameters. BMI average was 30.7 kg/m2 and 36 men (45.56%) were smokers and 60 men (75.94%) suffered from primary infertility while 19 men (24.06%) had secondary infertility.
| Age (Years) | 35.23 (±±4.78) 35.00 (25-49) |
| Sperm concentration (Million/ml) | 73.22 (±46.17) 60.00 (16-250) |
| Sperm motility (A+B) (%) | 58.42 (±11.21) 59.00 (39-88) |
| Sperm morphology (%) | 88.78 (±10.70) 92.00 (30-96) |
| DFI (%) | 21.14 (±10.26) 18.12 (5.09-57.23) |
| BMI average | 30.7 kg/m2 |
| Smokers (%) | 45.56% |
| Primary infertility (%) | 75.94% |
| Secondary infertility (%) | 24.06% |
Table 1: Characteristics of the seventy nine men with normal standard semen parameters.
Data are presented as numbers for age and sperm concentration parameter and as percentages for the remaining parameters. Data are presented as mean (± Standard deviation) and median [Min-Max]. Low level of DFI (<20%) was observed among 28 (56.0) obese subjects which did not signify any difference when compared with high DFI (≥20%) subjects. Likelihood of low DFI (<20%) among obese subjects was (Unadjusted OR) OR = 0.9 (0.3 to 2.5) and the adjusted OR was 1.1(0.4 to 2.8), that also predicted insignificant relationship.
Low level of DFI (<20%) among primary infertility cases was 2.2 (0.7 to 7.2) times more than the secondary infertility subjects that had DFI (≥20%), but the adjusted odds ratio predicted an incidence of 0.4 (0.1 to 1.2) and the difference was not significant.
However; Low level of DFI (<20%) among smokers was 0.5 (0.2 to 1.3) times more than the smokers that had DFI (≥20%), but the adjusted odds ratio predicted its likelihood of 2.2 (0.9 to 5.6) times and the difference was not significant. As shown in Tables 2 and 3.
| DFI | p value | |||||||
|---|---|---|---|---|---|---|---|---|
| ≥ 20 | <20 | Total | ||||||
| n | % | n | % | n | % | |||
| BMI (kg/m2) | <30.0 | 12 | 41.4 | 17 | 58.6 | 29 | 36.7 | OR=0.9 (0.3 to 2.5) P>0.05 (NS) |
| ≥30.0 | 22 | 44.0 | 28 | 56.0 | 50 | 63.3 | ||
| mean ± SD | 31.2 ± 5.7 (16.0, 45.0) | 30.4 ± 5.4 (17.0, 50.0) | 30.7 ± 5.5 (16.0, 45.0) | |||||
| Infertility | Secondary | 11 | 57.9 | 8 | 42.1 | 19 | 24.1 | OR=2.2 (0.7 to 7.2) P>0.05 (NS) |
| Primary | 23 | 38.3 | 37 | 61.7 | 60 | 75.9 | ||
| Smoking | NO | 15 | 34.9 | 28 | 65.1 | 43 | 54.4 | OR=0.5 (0.2 to 1.3) P>0.05 (NS) |
| YES | 19 | 52.8 | 17 | 47.2 | 36 | 45.6 | ||
| Total | 34 | 43.0 | 45 | 57.0 | 79 | 100.0 | ||
Table 2: DFI (%) in relation with BMI, infertility and smoking.
| B | Sig. | Exp(B) | 95% C.I.for EXP(B) | ||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| BMI (kg/m2) | 0.068 | 0.891 | 1.070 | 0.407 | 2.812 |
| Infertility | -0.866 | 0.115 | 0.421 | 0.143 | 1.235 |
| Smoking | 0.783 | 0.100 | 2.188 | 0.861 | 5.558 |
| Constant | 0.052 | 0.892 | 1.053 | ||
Table 3: Adjusted odds is binary coefficient for odds ratio.
Sperm DNA damage has been attributed to a variety of intrinsic and extrinsic factors, even in case of presence of some ‘female factor’. The most important is the production of reactive oxygen species that is excited by excessive stress, competitive sports, alcohol and drug abuse or nicotine. Increased levels of DNA fragmentation could explain a realistic method, for instance lifestyle modification or antioxidant supplementation to manage the oxidative stress related damage [12].
The current study shows that 41.8% of infertile men with normal standard semen parameters have a DFI level ≥ 20%. These findings support the use of DFI as a marker of male infertility in cases of infertile men with normal and to be carried out as a conventional part of semen analysis.
Our findings are in line with those of a previous study conducted in Lima, Peru among infertile men aged of 30-39 and 40-49 with DFI of 39 percent and 42 percent respectively [13].
On the other hand, our DFI prevalence was higher than 25% DFI prevalence found in a Swedish study conducted by Oleszczuk in 2012 [5]. In addition, our DFI > 30% (17.7%) was higher than infertile men with normal semen standard parameters who had a DFI >30% of 5% in a study conducted by Erenpreiss et al. [14].
The major limitations of this studythe limited sample size collected from a single specialized infertility center in Riyadh and the chance to exclude female sub-fertility as a reason adding to the infertility of the couple.
A comprehensive testing of DNA damage in adequately infertile men with normal semen standards can have a critical impact to overcome the primary pathology in pre-assisted reproductive technique assessment [15,16]. Our results suggest that sperm DNA integrity assessment may help to differentiate men with fertility problems and can therefore be of help in counseling of infertile couples.
It is interesting that sperm DNA impairment can provide answers to infertile cases and may guide selecting the appropriate assisted reproductive technique like avoiding the prolonged attempts to become spontaneously pregnant, repeated abortions, or referral for intra uterine insemination for couples in which the DFI of the male partner is high.
This cross sectional study reveals that prevalence of DFI ≥ 20% and ≥30% as seen in our Saudi infertile men with normal semen standard parameters was found to be 41.8% and 17.7% respectively. This prevalence would support the generalizability about DFI by sperm chromatin dispersion as an essential test to explain causes of infertility in cases where semen analysis has not shown any deviation from the norms.
M. G, H. M, H. S and M. T have all given substantial contributions to conception and design of the present study. All authors have contributed to acquisition of data, analysis as well as interpretation of data. M. G has drafted the manuscript and H. M, H. S and M. T have revised the content critically. All authors read and approved the final manuscript.
The study was supported by a grant from the Saudi Research Society.