Journal of Osteoporosis and Physical Activity
Open Access
ISSN: 2329-9509
ISSN: 2329-9509
Case Report - (2015) Volume 3, Issue 1
Spondylodiscitis is an infection of the spine that involves the intervertebral disc and the vertebral body characterized by insidious onset and non-specific symptoms.This paper aims to emphasize the many opportunities presentation of spinal infections.We describe a retrospective case of a 74-year-old male with back pain that develop a spondylodiscitis with non-specific symptoms. The diagnostic work-up included Tc_99m Leukocyte scintigraphy, computed-tomography, MRI and cultures. The infective organism was Oxacilline-sensitive sthaphylococcusaureus and the patient was successfully treated with intravenous amoxicillin+clavulanic acid combined with moxifluoxacin followed by surgery. Diagnosis of spondylodiscitis is frequently delayed. Suspicion for diagnosis is required in patients with back pain.
<Keywords: Spondylodiscitis; Back pain; Intervertebral disc; Amoxicillin+clavulanic acid; Moxifluoxacin
The incidence of Pyogenic Spondylodiscitis (PS) seems to be increasing in the last years as a result of the higher life expectancy of older patients with chronic debilitating diseases; also a number of co-morbidities have been found to increase the risk of disease such as diabetes (11-31%), immunosuppression, intravenous drug use, alcoholism, chronic debility disease with decubitus ulcers, malignancy, alcohol use and renal failure. The source of infection in the elderly has been related to the use of intravenous access devices and the asymptomatic urinary infections [1].
A single organism is usually involved, although polymicrobial infections do occur in chronic and debility conditions [2]. Staphylococcus aureus is the most common organism isolated implicated into 15- 84% of nontuberculosis cases of infection and frequently observed as complication of invasive spinal procedures (17-33%) [3,4]. Bacilli gramnegative such as E.Coli, Proteus and Pseudomonas are often associated with immunosuppressive conditions, diabetes, procedures or infection involving the genitourinary and gastrointestinal tract [5]. At the other hand immuno compromise patients, homeless, alcolists, prisoners or immigrants from sub-Saharan Africa, the Indian sub-continent and south-east Asia are exposed to tuberculosis infection.
Finally fungal infection represents1% of non-tuberculosis spondylodiscitis in adults immuno compromise patients and usually involves Candida albicans, less commonly other Candida or Aspergillus [6]. The incidence of vertebral osteomyelitis is estimated to be 2.4 cases per 100000 annually with male predominance [7].
Epidemiologic studies confirmed that males are more affected than female in the ratio of 2:1 for unknown reason. The average age is in the fourth to fifth decades and the most common level of involvement is the lumbar spine, followed by the thoracic, cervical and sacral levels [8].
Unremitting back pain, characteristically worsening during the night and exacerbated by movement and may radiate to the abdomen, hip, legs, scrotum or perineum, is the most common presentation combined with general symptoms as weakness, fatigue, fever and chills.Radicular symptoms are present in 50-93% of cases. Paravertebral muscle tenderness, spasm, and limitation of spine movement represent the predominant signs. Neurologic complications such as spinal cord or nerve root compression and meningitis occur in approximately 12% of patients. The progression of spinal pain to radicular signs followed by weakness and paralysis suggests the formation of an epidural abscess [2].
The diagnosis of haematogenous vertebral osteomyelitis may be very difficult, as the symptoms can be sometimes not specific, vague or absent.Arise in the ESR and CRP is seen in over 90% of patients [9].
Rath et al. have reported that the C-Reactive Protein (CRP), although nonspecific, may be a more clinically useful index than the ESR, and should be used to follow the course of the disease. Serumprocalcitonin is said not to be useful. Leucocytosis occurs in less than 50% [3]. Blood, urine and focal supportive processes should be cultured. Blood cultures may be positivein approximately 50% of patients and are helpful in guiding the choice of antimicrobial therapy [10]. The usual delay in diagnosis has been reported to be two to four months despite the use of imagine-technique. X-ray is helpful at the beginning; however it is not a sensitive methods for diagnosis [7]. In the early diagnosis it is important the role of bone scintigraphy and Fluorodeoxy glucose PET (FDG-PET) to localize the abnormalities and monitoring response to treatment [11]. MRI is the most sensitive (93-96%) and specific (92.5-97%) modality for early detection of spondylodiscitis [2]. It can differentiate between pyogenic discitis, neoplasia and TB, provides better definition of the paravertebral and epidural spaces. It also allows optimal assessment of any compression of neural elements [12].
The treatment of pyogenic spontaneous spondylodiscitisis either conservative or surgical. The goals of treatment should be to relieve pain, prevent or reverse neurologic deficits, eradicate infection, prevent relapse, and establish spinal stability.Conservative management generally comprises intravenous followed by oral antibiotics, spinal immobilization, monitoring clinical and radiological evidence of spinal instability, progression of infection or neurological impairment. Therapy must therefore be based on theoretical considerations including antimicrobial activity against the known or likely pathogens, ability to penetrate bone and particularly disc tissue, together with considerations such as side effect profile and easiness of administration. There are no data from controlled trials that suggest the duration of therapy. At this time the recommended duration of therapy isfrom 4 to 6 weeks to 3 months [7].
The general principles for the management of spine infections are non operative consisting of external immobilization and intravenous antibiotics, followed by oral antibiotics.
Indications for surgery should be given in case of absence of clinical improvement after 2-3 weeks of intravenous antibiotics, persistent back pain and systemic effects of chronic infection and with presence or progression of neurological deficit in elderly or in cervical infection. Chronic osteomyelitis may require surgery in case of a development of biomechanical instability and / or vertebral collapse with progressive deformity [13].
A clinical follow-up at 4 weeks is useful to assess the response to treatment and to evaluate the onset of worsening conditions [7].
The complications of spondylodiscitis are related to the level of the spine involved and to the extension of the process to the surrounding tissue. Epidural abscess, subdural abscess, meningitis, loss of lordosis, segmental collapse with subsequent spinal instability and progressive neurologicalimpairment may complicate spondylodiscitisinvolving any level.Epidural abscess is a serious complication, affecting 4-38% of cases of spontaneous spondylodiscitis.
Hadjipavlou et al. reportedthat the rate of epidural extension complicating spondylodiscitis was 90% in the cervical spine, 33.3% in the thoracic spine and 23.6%in the lumbar spine, suggesting that spondylodiscitis affecting more cephalic regions of the spine carries a significantly increased risk of secondary epidural abscess [14]. A longterm sequelae of vertebral osteomyelitis include irreversible paralysis that affect 4-22% of patients with spinal epidural abscesses and a mortality in a range of 2-20% [10].
This report concerns a geriatric malewith spondylodiscitis presenting withnon-specific symptoms. This case underlinesthat PS should be included inthe differential diagnosis of unexplained back pain.
A 74-year male with unremarkable medical history presented with a two months history of cervical pain and scapular-humeral girdle functional impairment without relevant general symptoms; only associated morning stiffness was present. Cervical spine and scapular-humeral girdle plain X-ray were normal while mild abnormal laboratory tests were describedincluding Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP). Patient was treated as a rheumatic polymyalgia and started corticosteroid therapy (prednisone 25 mg once a day, slow tapering).
Three months later the patient was still on prednisone treatment but cervical pain worsened and night dorsal pain emerged. A physical examination found local tenderness over dorsal spine areas and a lateral-dorsal spine X-ray showed a vertebral fracture of thoracic level (T9) (Figure 1).
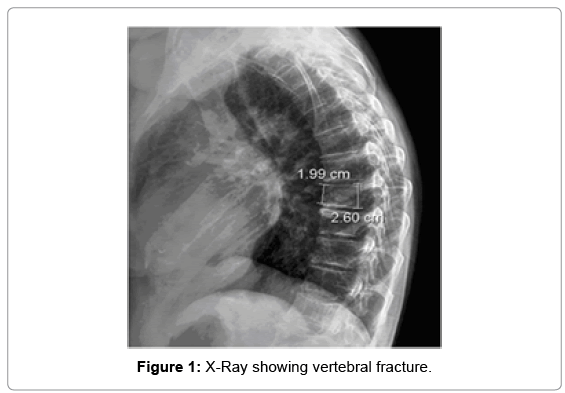
Figure 1: X-Ray showing vertebral fracture.
Dual-Emission X-Ray Absorptiometry (DEXA) revealed lumbar ( T-score L1-L4:-3.4; BMD L1-L4: 0.826 g/cm2) and femoral (T-score total hip:-1.5; BMD total hip: (0.900 g/cm2) osteoporosis but the study of bone metabolism did not revealed tests abnormality, looking for secondary causes of osteoporosis, was presented. Glucocorticoidsinduced osteoporosis was diagnosed and anti-resorptive treatment with oral alendronic acid 70 mg, once a weekstarted.
One month later the patient developed fever (39°C), legs pain and muscle spasms, worsening of dorsal pain (patient’s VAS=80 mm) with abnormality of laboratory tests(ESR=120 mm/h PCR 170 mg/dL); serial blood culture was detected and Oxacilline-sensitive sthaphylo coccusaureus was isolated.
Tc_99m Leukocyte scintigraphy identified thoracic T8 abnormal uptake of radiolabeland confirmed suspicion of vertebral spondylodiscitis and a CT-scan helped to outline the extension of bone destruction. The patient was treated with amoxicillin+clavulanic acid (2gr i.v/daily) combined with moxifluoxacin (400 mg daily orally), analgesic treatment (oxycodone 5 mg+ acetaminophen 325 mg two once a day) and ortesical spinal immobilization.
The patient was re-admitted after six weeks for incomplete sensory paraplegia with motor impairment below the T8 dermatome. MRI showed extensive reduction of vertebral canal diameter and spinal cord compression (Figure 2). Posterior decompression by laminectomy surgery and vertebral stabilization was performedand after 24 months the patient was fully recovered (Figure 3).
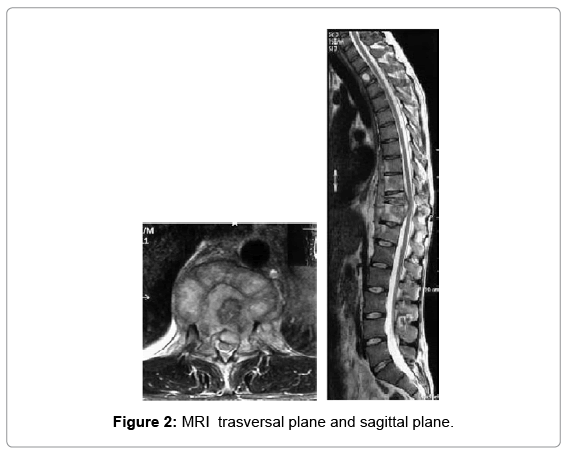
Figure 2: MRI trasversal plane and sagittal plane.
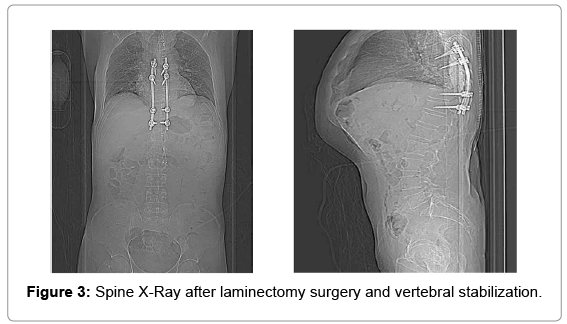
Figure 3: Spine X-Ray after laminectomy surgery and vertebral stabilization.
Low back pain is secondreason for visits to a physician in the older population over 65 years of age [15].
Experimental studies suggest that low back pain mayoriginate from many spinal structures and 85 percent of patients with isolated lowback pain cannot be given a precise pathoanatomical diagnosis. The association between symptoms and imaging results often feeble [16]. In the literature fever suggests the possibility of spinal infection as spondylodiscitis, discitis, vertebral osteomyelitis, and epidural abscess [14,17]; the infection is usually the result ofsystemic bacteremia from a distant septic focusand predisposing factors include immunosuppression,diabetes, underlying diseases, intravenous drug abuse,previous spinal surgery, and spinal anesthetic procedures [18].
As reported by a recent work of McHenry MC et al also spinal trauma is a considered a risk factor of disease.
After Myc tuberculosis, S.aureusis the commonest etiological cause of bone and joint infection [19].
S.aureus is an evolved pathogen that express many surface proteins namely adhesins or MSCRAMMs (microbial surface components recognizing adhesive matrix molecules) that facilitates the adherence to bone matrix components such as laminin, fibronectin [20]; moreover the pathogen is able to form a biofilm which creates a “sanctuary site” in which the pathogen grows protected from antimicrobial drugs.
The clinical course of infection differing between adult and child, in the first case the onset of disease is slow and gradual without specific symptoms and diagnosis is common delayed [21].
As reported by Goel et al. often in the older population the absence of fever or leukocytosis in almost half the patients, coupled with nondiagnostic plain radiograph changes resulted in a delayed diagnosis [15].
Furthermore in this age group with other more prevalent causes of back pain,such as vertebral fractures fromosteoporosis and osteoarthritis, the infective spinal disease often is not considered in the differential diagnosis.
In our patient the clinical presentation confirmed this data resulted into a non specific presentation of symptoms and into a notresponsive radiological assessment with traditional X-ray. Plain radiography is not highly sensitive for early cancer or infection, and therefore ancillary tests, such as measurement of the erythrocyte sedimentation rate and a complete blood count, may help rule out systemic diseases.
The clinical presentation of our patient did not suggested at the beginning a differential diagnosis betweenosteoporosis and spondylodiscitis; X-ray showed a vertebral lesion compatible with osteoporosis fracture without specific symptoms. and has proved a less specific and sensitive instrumental. The definitive diagnosisof spondylodiscitiswas reached by gadolinium-enhanced spinalMRI.
Spinal infection oftenmasquerades as osteoporosis on X-ray underline the importance of MRI to differentiate osteoporosis, vertebralosteo myelitis, and spondylodiscitis, especially when other investigations(spinal x-rays and CT scan) still yield negative results or insufficient data [7,11,12].
These infections are notoriously difficult to treat: treatment includes medical or conservative management, when clinical symptoms are mild with minimal bony destruction, by a combination of prolonged antibiotic therapy; the standard protocol includes an intravenous approach with β-lactam agents preferably a penicillinaseresistant penicillin. Vancomycin is an inferior drug due toa poor bone penetrationand a molecule unable to sterilize the bone, as performed in some animal studies, so it is associated with a major risk of treatment failure [14]. Recommended duration of therapy is from 4 to 6 weeks to 3 months.The oral antimicrobialtherapy is an attractive alternative possibility but at this time there is not sufficient evidence that recommended this approach [15].
Surgical intervention is required only if the patient presented complications such as neurological deficits, significant bone involvement with instability;recommendations regarding the optimal surgical strategy for spondylodiscitis remain controversial.
Our patient presented neurological manifestations and did not responded to medical therapy alone; surgery was necessary and effective.
Spontaneous spinal infection in geriatric population is common and should be included inthe differential diagnosis of unexplained back pain; suspicion and early approach can reduce the complications.