Journal of Thyroid Disorders & Therapy
Open Access
ISSN: 2167-7948
ISSN: 2167-7948
Research Article - (2014) Volume 3, Issue 3
Background: Restrictive strabismus is a common feature of Thyroid-Related Ophthalmopathy (TRO) causing intractable diplopia. We reviewed the surgical outcome for TRO patients.
Methods: We retrospectively reviewed patients of TRO who underwent strabismus surgery from January, 1998 to September, 2012. Preoperative characteristics were recorded such as age, sex, disease severity, presence of compressive optic neuropathy or elevation of intraocular pressure, symmetry of orbitopathy, duration between onset of TRO and surgery, smoking status, and treatment. The length of muscle recession and the numbers of strabismus surgeries was recorded for further analysis.
Results: Twenty-four patients were enrolled with twelve female and twelve male in a mean age of 55.5 years (SD + 10.71). The mean number of surgery was 1.29 (SD + 0.46). Patients with asymmetric involvement at onset, presence of elevated intraocular pressure, and longer intervals between the onset of TRO and first surgery needed significantly more surgeries to correct strabismus. Factors such as age, gender, smoking status, medical treatment before surgery, presence of compressive optic neuropathy or previous orbital decompression procedure had no statistically significant effect on the number of surgery required.
Conclusion: Strabismus surgery showed favorable outcomes in correcting diplopia induced by thyroid-related ophthalmopathy. The average number of surgery needed is 1.29 (±0.46) in this study, and the mean surgical effect we got was 4.09+0.26 PD/mm of rectus muscle recession.
Thyroid-related ophthalmopathy [1]/ orbitopathy (TRO), also known as thyroid-associated ophthalmopathy [2]/ orbitopathy (TAO)[3], thyroid eye disease (TED),[4,5] or Graves’s ophthalmopathy [6]/orbitopathy,[7] is considered an autoimmune disease which is characterized by chronic inflammation of orbital soft tissue, extraocular muscles, conjunctiva and even eyelids [1,8]. Usually, we see patients with eyelid retraction, swelling and erythematous change of periorbital tissue and conjunctivae, and exophthalmos [6,9]. It causes social and visual problems by disturbed appearance and visual function [10].
Pathologically, anti–thyrotropin-receptor antibodies binding to thyrotropin receptor result in overproduction of thyroid hormone in Graves' hyperthyroidism patients [11]. The fact of that almost all patients with Graves' ophthalmopathy have anti–thyrotropin-receptor antibodies suggests that Graves' ophthalmopathy and hyperthyroidism may share the same mechanism of immunoreactivity against the thyrotropin receptor [12]. Gerding et al. reported that the levels of anti–thyrotropin-receptor antibodies and clinical features of TRO are in a positive correlation [13]. Furthermore, the study of Eckstin et al. suggested that the levels of anti–thyrotropin-receptor antibodies influence the prognosis [14].
In the acute phase of the disease, patients usually report orbital pain, diplopia and ocular movement limitation which result from lymphocytic infiltration and congestion of orbital tissues including the extraocular muscles. In the chronic phase, the adipose tissue infiltration and fibrotic change of the extraocular muscles result in restrictive strabismus [6,15]. Among these signs of TRO, impaired ocular motility and alignment have been found to profoundly influence the quality of life of affected individuals [6,10]. Clinically, TRO most frequently involves the inferior and medical rectus muscles [4,5]. The diplopia usually progresses from intermittent to constant, and finally needs surgical management. Due to the tightness and poor elasticity of involved muscle, the surgical outcome is not always predictable, and patients may need more than one surgery. To present the outcome of strabismus surgeries and to investigate the possible factors for multiple surgeries, we reviewed the surgical outcome and analyzed the surgery-related features in TRO patients.
We performed a retrospective chart review of consecutive patients with TRO who underwent strabismus surgery, based on medical records of patients in a tertiary referral center, Kaohsiung Veterans General Hospital, from January, 1998 to September, 2012. Patients were identified from hospital electronic diagnostic database according to ICD-9 codes (376.21: Thyrotoxic exophthalmos) combined with a hospital surgical coding system (strabismus surgery). The inclusion criteria are as following:
1. Age older than 18 and younger than 80 years old.
2. Patients in euthyroid status during follow-up
3. Stable deviation in at least 3 month’s follow-up, which means a variation of less than 2 prism diopter between two consecutive visits
4. Received at least one strabismus surgery, including muscle weakening or strengthening procedures.
5. Complete 6 month’s follow-up postoperatively
Patients with previous strabismus surgeries, or postoperative follow-up less than 6 months were excluded. The hospital Institutional Review Board and Ethics Committee approved this study, which adhered to the tenets of the Declaration of Helsinki.
The preoperative and postoperative ocular examination included best-corrected visual acuity, color discrimination test (Ishihara color plate), intraocular pressure (IOP), deviation at primary position by alternate prism cover test, ocular motility, existence of exophthalmos (Hertel exophthalmometer), examination of external eye, anterior segment and posterior segment. The decision of surgical dose was based on preoperative deviation, the pattern of motility limitation and forced duction test during surgery. All surgeries were performed by the same surgeon, M.C. Lin with non-adjustable method.
Preoperative data included gender, age at onset of TRO, smoking status, symmetry of TRO at onset, amount of horizontal and vertical deviation in prism diopter, elevation of intraocular pressure(IOP) after diagnosis of TRO, compressive optic neuropathy, previous orbital decompression procedure, treatment before strabismus surgery, interval between onset of TRO and strabismus surgery. According to the standard National Health Interview Survey (NHIS) current smoking definition, current smoker was defined as having smoked at least 100 cigarettes in his/her entire life and smoking cigarettes every day or some days [16]. Symmetry of TRO was divided into symmetric and asymmetric, according to first presentation of the patient. If the patient presented as redness, swelling, pain, or limitation of extraocular muscle in only one eye, or more than (or equal to) 2 mm of the difference of exophthalmia, he was classified into the asymmetric group. If the patient presented with above symptoms of both eyes or less than 2mm difference of exophthalmia, he was defined as having symmetric TRO [17]. Elevation of IOP after diagnosis of TRO was defined as new onset of elevated intraocular pressure(more than 21mmHg) with or without glaucomatous optic disc change or compatible visual field defect. The steroids responder was excluded from this group if the patient’s intraocular pressure returned to normal within one month after discontinuation of steroids.
The treatment before strabismus surgery included intravenous pulse methylprednisolone therapy (3 eyes, 12.5%), retrobulbar injection with triamcinolone (7 eyes, 29.2%), and oral prednisolone (12 eyes, 50%). The intravenous methylprednisolone pulse therapy was given as 250mg g6h for 3 days (total 12 doses) followed by oral prednisolone according to clinical condition. The retrobulbar injection of triamcinolone was given as 20mg/0.5ml/shot, repeated in 3-4 weeks’ interval. The oral prednisone was started as 1mg/kg/day, and then gradually tapered by 5-10 mg /day every 1-2 weeks.
The surgery perform on TRO patients included muscle recession, muscle resection or tucking, and sometimes myotomy. The surgery of choice is recession of tight muscles. Although there are still controversies about performing resection or tucking of a rectus muscle in TRO patients [4,18,19], we did resection on the antagonist muscle if maximal recession or myotomy could not bring the globe into primary position. We performed myotomy only when the muscle planned to be recessed was too tight, and the forced duction test was still positive after the muscle was detached.
All strabismus surgeries were performed under general anesthesia. The surgeries were done through limbal incisions. The sutures used were 6-0 vicryl (Ethicon). The only exception was when operation on the inferior rectus muscle, then 5-0 dacron (Alcon) was used to prevent late overcorrection. Maximally two rectus muscles in the same eye were operated in one surgery to prevent anterior ischemic syndrome; however, if myotomy was performed, no more muscle surgery was done in six months. Operative data included the amount and the number of muscles recession (both horizontal and vertical). We followed patients at 1week, 6 weeks, 3 months and 6 months postoperatively, and the follow-up time was counted from the last surgery if more than one surgery was done. Success was defined as patients have no diplopia in primary position at distant and near without abnormal head position. If the patient had persistent diplopia after six months’ follow-up, a second surgery was considered. The preoperative, postoperative ocular alignments and the numbers of strabismus surgeries required were collected for analysis. Mean surgical effect was calculated from data of patients receiving only muscle recession, and the data of patients receiving myotomy, recession-resection and the data of the second surgery were excluded. The mean surgical effect was expressed by the corrected deviation in prism diopters (PD) divided by the length of muscle recessed in millimeter (mm). All statistical analyses, including Fishers’ test, Mann-Whitney U test were conducted using SPSS version 20.0 (IBM Inc., New York, United States).
Twenty four patients were enrolled in this study, twelve female (50%) and twelve male (50%). Mean surgical effect was calculated on 14 patients receiving pure muscle recession. The data of other 10 patients not receiving pure muscle recession is shown in table 1. The mean age was 55.50 + 10.71 years (range, 32 to 73 years). The mean age of males was 57.17+10.28 years (range, 41 to 73 years) and females was 53.83+11.31 years (range, 32 to 69 years) (p=0.59)(table 2).
| One surgery (N=17) |
Two surgery (N=7) |
p- value | |
|---|---|---|---|
| Age at surgery (mean, year old) | 55.35±10.83 | 55.86±11.25 | 0.71a |
| Sex | 9F, 8M | 3F, 4M | 1.00b |
| Unilateral at onset | 3(17.6%) | 5(71.4%) | 0.02a,b |
| Current smokers | 2(11.8%) | 1(14.3%) | 1.00b |
| Seconadry Glaucoma | 3(17.6%) | 6(85.7%) | 0.004b,c |
| Compressive optic neuropathy | 3(17.6%) | 2(28.6%) | 0.61b |
| Previous Treatment for TRO Intravenous pulse steroids therapy |
3(17.6%) | 0(0%) | 0.53b |
| Retrobulbar steroids injection | 7(41.2%) | 0(0%) | 0.06b |
| Oral steroids | 9(52.9%) | 3(42.9%) | 1.00b |
| Decompression | 5(29.4%) | 2(28.6%) | 1.00b |
| Mean time(months) between TRO onset and surgery | 27.41%±24.97 | 51.29±29.92 | 0.01a,c |
| F= female; M= male; TRO= Thyroid related Opthalmopathy a= Mann Whitney U test, b= Fisher’s test, c= Significant |
|||
Table 1: Preoperative parameters in relation to outcome
Eight patients (33.3%) had asymmetric involvement at onset. Three current smokers (12.5%) at first presentation were identified. Nine patients (37.5%) were grouped in the elevation of IOP during follow-up before strabismus surgery. Five patients (20.8%) had a history of compressive optic neuropathy related to TRO. Seven patients (7 eyes, 29.2%) had previous orbital decompression procedure. The mean duration from the onset of TRO and the first strabismus surgery was 32.21+27.08 months (range, 6 to 114 months).
The mean number of surgeries each patient received was 1.29+0.46 (range, 1 to 2). All patients, whether received one or more than one surgery, reached the status of diplopia-free at 6-month-follow-up after the last surgery, without prisms needed. Outcomes were correlated with preoperative characteristics. The main outcome measurement was the number of surgeries required for correcting diplopia, and the residual or recurrent strabismus after the first surgery. The maximal number of surgery each patient received is two. Seven patients received two surgeries, and seventeen patients just needed one surgery (table 2). The mean age of patients receiving one surgery and two surgeries were 55.35+10.83 (n=17, range, 32 to 72) and 55.86+ 11.25 (n=7, range, 36 to 73) years ago, respectively (p=.71). Patients with asymmetric involvement at onset (p=.02*) (Figure 1), presence of elevation of IOP (p=.004*) (Figure 2), and longer intervals between onset of TRO and first surgery (p=.01*) (Figure 3) needed more surgeries to correct strabismus significantly (Table 2). Logistic regression analysis still revealed that more surgeries is correlated with patients with asymmetric involvement at onset (Adjusted odds ratio= 9.41, p=.03*) and presence of elevation of IOP (Odds ratio= 23.79, p=.002*) (Table 3).
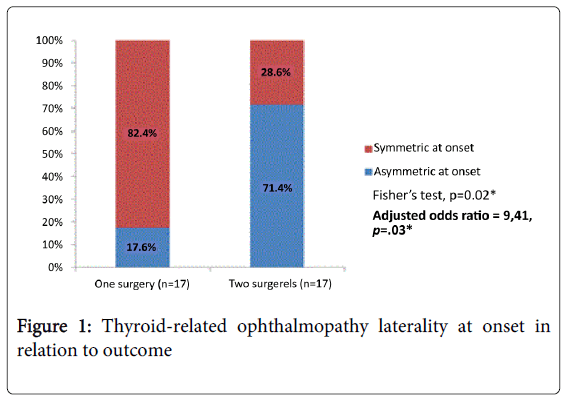
Figure 1: Thyroid-related ophthalmopathy laterality at onset in relation to outcome
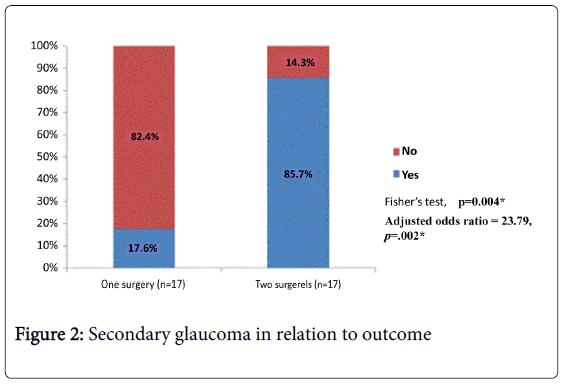
Figure 2: Secondary glaucoma in relation to outcome
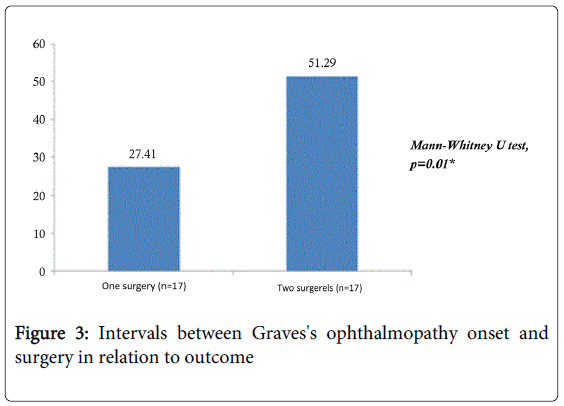
Figure 3: Intervals between Graves's ophthalmopathy onset and surgery in relation to outcome
Factors such as age, gender, smoking status, medical treatment before surgery, presence of compressive optic neuropathy or previous orbital decompression procedure had no statistically significant effect on the number of surgeries required (Table 2). However, there was a trend that retrobulbar injection with triamcinolone (p=.06) seemed to reduce the number of surgeries (Table 2). The surgical outcome calculated from the first muscle surgery was as following.
The numbers of patients receiving only muscle recession without strengthening of antagonist was eight for horizontal deviation and eleven for vertical deviation respectively, and the mean surgical effect was 4.29+0.34 PD/mm recession of horizontal muscles and 3.99+0.24 PD/mm recession of vertical muscle, respectively. The average surgical effect was 4.09+0.26 PD/mm of muscle recession.
Approximately 4% to 7% of patients with TRO require strabismus surgery [4]. In general, staged surgeries may be needed to correct the strabismus induced by TRO. Most surgeons recommend an observation time up to 6 months after ocular deviation have stabilized [7,20-22]. Meyer, D.R suggested that a stable postoperative alignment is more likely reached after an extended period of stable preoperative alignment, and it minimizes the need for repeated strabismus surgery [7]. However, the re-operative rates for strabismus with TRO were reported to be between 17% and 45%, even in patients having had stable deviations [6,7,23-26]. Of the twenty four patients in our study, seven (29.2%) received a second surgery due to unsatisfactory surgical result (table 1). The reoperation rate is comparative to literature.
Our previous study revealed that the severity of TRO was correlated with patients’ age [27]. However, there is no significant correlation between age and number of surgeries required in this study. (p=.71) (table 2). We didn’t use the clinical activity score 11 (CAS) to access the severity of TRO in this study. Mahmoud et al used CAS to access the disease severity of their patients, and noted that although better postoperative outcomes were associated with earlier surgery, they did not have good correlation with CAS [6]. That means CAS was probably not useful to predict the postoperative stability. Further investigation will be needed for the relationship between the severity of TRO and the number of surgeries.
Smoking has been well known to be associated with more severe TRO and smokers respond less well to treatment in the active phase of TRO [8,28-33]. Cytokine release following smoking-induced hypoxia may increase the inflammation of TRO [34,35]. Rajendram et al. points out that the strabismus surgery in TRO patients can be more difficult because of the post-inflammatory changes in the peribulbar tissues and the muscular contracture and fibrosis. They suggested that smoking at presentation aggravated the myopathy and the strabismus in TRO [36]. However, smoking might have no direct impact on the surgical result. Mahmound et al found that an active smoker did not necessarily show worse surgical outcome in their study [6]. There were three current smokers in our study (12.5%) and they did not show higher reoperation rate than others (Fisher’s exact test, p=1.0) (table 2). However, we need more investigation to support this point because the sample size was too small. Furthermore, TRO in current smokers may not stabilize in months, and that’s probably why we only had three smokers.
In this study we also found that the presence of elevated IOP, asymmetric orbital involvement at onset, and longer intervals between TRO onset and surgery were significantly correlated with increased numbers of surgeries.
Clinically, although increased intraocular pressure was noted frequently in patients with TRO, the definite mechanism was not well known. In literatures, there are several theories on the causes of increased IOP in TRO, including increased mucopolysaccharide deposition in the trabecular meshwork, increased resistance to trabecular outflow, increased episcleral venous pressure resulting from orbital congestion and obstruction of venous outflow, a genetically linked predisposition to glaucoma, and restriction and compression of the globe by fibrotic and enlarged rectus muscle [2,37-43]. In our study, the reoperation rate in patients with elevation of IOP was higher significantly. It suggested that patients with elevation of IOP might have more severe orbital congestion, muscle fibrosis or muscle enlargement, thus increased the unpredictability and complexity of strabismus surgery.
Soroudi et le analyzed the Hertel measurements of TRO patients before orbital decompression surgery and found that 36 of 391 patients (9%) had asymmetric exophthalmos with a difference equal to or more than two mm [17]. In our study, eight of the twenty four patients (33.3%) had asymmetric involvement at onset which was significantly correlated with increased numbers of surgeries. Patients with asymmetric involvement at onset may show more unpredictable disease course. Mahmound et al also found that the outcome of patients with symmetric TRO is more favorable, and suggested that asymmetric orbital or muscle involvement would need asymmetric surgery also [6].
Patients with longer intervals between TRO onset and surgery might have a more eventful course, and it took longer to reach stable condition. The complexity also explained the need of more surgeries.
Although patients with TRO may need more than one surgery to correct their strabismus, the overall outcome, including the elimination of diplopia and improvement of ocular movement and cosmetic appearance, is favorable. In this series, we got mean surgical effect of 4.09+0.26 PD/mm of rectus muscle recession. This should be taken into consideration when planning surgical dosage. Although we expected multiple surgeries in such patients, the average number of surgery required to eliminate diplopia is 1.29 (±0.46) which is encouraging. In conclusion, the outcome of strabismus surgery on TRO patients is good as long as the hormonal condition and the ocular deviation are stable. *The authors have no financial interest in the material presented.