Advanced Techniques in Biology & Medicine
Open Access
ISSN: 2379-1764
ISSN: 2379-1764
Case Report - (2015) Volume 3, Issue 3
Transplant infectious disease has evolved toward prevention and early detection, in order to prevent full-blown syndromes [1]. Recipients of a solid organ transplant are susceptible to developing a variety of infectious complications that occur frequently with nonspecific symptoms, mimicking other complications such as rejection or drug toxicity [2]. The complications could be controlled, but if is not, this could end in an allograft dysfunction or even worst in a fatal ending with multiple organ failure and dead [1]. Parasitic infections in transplant patients are rare, limited to tropical countries (Brazil) and endemic areas of Iberian countries (Spain) [3] of all the parasitic species that can infect the human, only 5% has been identify [4]. The most common causes parasitic infections are protozoa like P. jirovechi and toxoplasma gondi with Strongyloides stercoralis and schistosomas in second place [4]. Below a case of S. stercoralis infection in renal transplant patient is exposed.
We present a case of a 54 years old female from Tamaulipas, Mexico (North-eastern of the country), with hypertension history , stage 5 chronic kidney disease diagnosed the previous year treated with renal replacement therapy in hemodialysis with arterio-venous fistula (AVF). The patient present with an atypical pneumonia seven months after she receives kidney transplant from a deceased donor.
Talking about the kidney transplant the patient presented as relevant data a positive crossmatch and high panel reactive antibody (PRA) test at transplant time, class I 30%, class II 56% (previous class I 90% class II 96%), polyclonal antibodies were used as induction therapy and plasmapheresis as peri transplant desensitization therapy. She had adequate graft function and was discharged from hospital clinically stable with prednisone, mycophenolate mofetil and tacrolimus as immunosuppressive therapy, valganciclovir and sulfamethoxazoletimethroprim as prophylaxis.
Two weeks before her last hospitalization, the patient presented epigastric pain without improvement after the use of proton pump inhibitors. An endoscopy was performed where we found erosive gastritis, 48 hours later she developed dyspnea with minimal effort, therefore is hospitalized to initiate management as atypical pneumonia, probably influenza, with oseltamivir. Due the patient do not improvement a bronchoscopy with biopsy is performed. After that the patient develops moderate adult respiratory distress syndrome (ARDS) whereby orotracheal intubation is need, after her stabilization, the patient was transferred to our hospital in Monterrey, Nuevo Leon, as atypical pneumonia (bilateral diffuse micronodular infiltrate and ground glass was described in her chest tomography) (Figure 1).
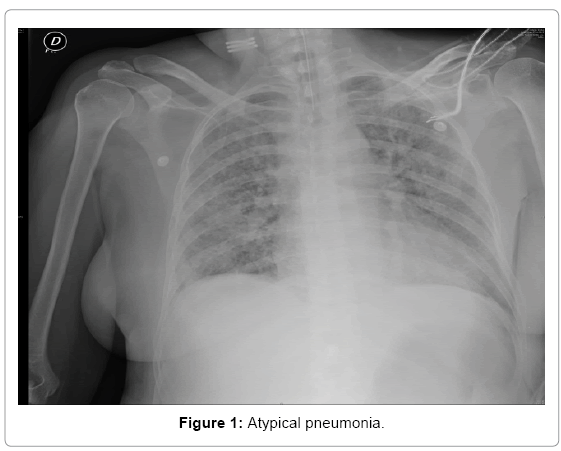
Figure 1: Atypical pneumonia.
In her blood count pancytopenia was evidenced and no eosinophilia was found. After that immunosuppressive therapy and valganciclovir were suspended, a slight elevation of nitrogenous with diuresis kept at 1 ml/kg/hr was also documented, 48 hours after admission the patient showed an improvement of pancytopenia and treatment with tacrolimus and valgancilcovir was restarted.
The lung biopsy reported a picture of helminth S. stercolaris, due to this treatment with ivermectin was initiated. Despite treatment she presented severe hypoxemia with ventilatory difficulty and cardiopulmonary arrest 24 hours later, after 10 minutes of advanced cardiopulmonary resuscitation with pulse recovery the patient presented impaired renal and hepatic function and it was decided to install acute hemodialysis catheter and initiate continuous renal replacement therapy (Figure 2).
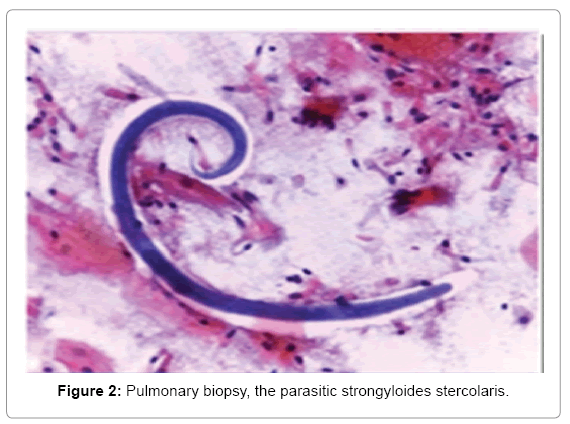
Figure 2: Pulmonary biopsy, the parasitic strongyloides stercolaris.
By this moment the patient was diagnosed as hyperinfection syndrome, appearing as multiple organ failure, with mixed acidosis (lactic and respiratory), acute renal injury with elevated creatinine from 1.2 mg/dl to 4.1 mg/dl with oliguria and respiratory distress syndrome.
We try to stabilize and provide her every opportunity despite knowing the dismal prognosis, but six hours after the first cardiac arrest the patient died.
Parasitic infections in the post renal transplant, are difficult to diagnose because there are few patients who have symptoms. The most important pest in these patients probably is S. stercoralis. Because of its cycle of self-inoculation is the only worm that can remain in the gastrointestinal tract for decades after the individual left the endemic area (Latin America, Southwest Asia and southeastern United States [5].
S. stercoralis is an intestinal parasite, clinically presents with nausea, diarrhea, hemoptysis, severe bronchospasm and eosinophilia. In transplant patients may be aggravated by increasing adult worms causing multiple organ failure.[6] Temporally distant S. stercoralis infection may reemerge, often in the first year after transplantation, as a hyperinfestation syndrome consisting of hemorrhagic enterocolitis, pneumonia and gram-negative bacteremia or meningitis [7] It may be due to reactivation of an existing infection or come from the transplanted kidney.
It has a mortality rate of over 90% [6]. Empirical treatment with ivermectin before transplantation prevents such infection in strongyloides seropositve recipients [7]. Diagnosis is by ELISA but definitive diagnosis is made by finding the larva. The proposal treatment is thiabendazole, albendazole or ivermectin [6]. In the International literature there are few clinical cases reported, mostly in men presenting high mortality.