Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Research Article - (2015) Volume 0, Issue 0
Objective: Patients with pancreatic adenocarcinoma have an increased propensity for diabetes. Recent studies suggest patients with diabetes and pancreatic adenocarcinoma treated with metformin have increased survival. This study was undertaken to determine if metformin use is associated with increased survival for patients with pancreatic adenocarcinoma.
Methods: Patients who underwent pancreaticoduodenectomy for pancreatic adenocarcinoma from 1991-2013 were included in this study. Survival was evaluated by Kaplan-Meier analysis. Median data are reported. Significance was accepted with 95% probability.
Results: Out of 414 patients undergoing pancreaticoduodenectomy for pancreatic adenocarcinoma, 132 (32%) was diabetic. Of diabetic patients, 35 (27%) were diet-controlled, 34 (26%) were treated with insulin alone, 18 (14%) were treated with metformin alone, 14 (10%) were treated with sulfonylureas alone, 7 (5%) were taking sulfonylureas with insulin, and 24 (18%) patients were taking metformin with sulfonylureas and/or insulin. Patients with or without diabetes not taking sulfonylureas had survival of 16.4 months compared to patients taking sulfonylureas who achieved survival of 27.5 months after undergoing pancreaticoduodenectomy (p<0.05).
Conclusion: Patients taking sulfonylureas with or without other therapy had improved survival compared to patients not taking sulfonylureas after pancreaticoduodenectomy. Metformin does not appear to be beneficial for patients with resectable disease, but may have a benefit for patients with unresectable and/or metastatic disease as shown in prior studies. The use of sulfonylureas is associated with a survival benefit for patients undergoing resection for pancreatic adenocarcinoma. Tumor staging and margin status continue to be the overriding predictors of survival for patients with resectable pancreatic adenocarcinoma, not metformin therapy.
<Keywords: Metformin; Pancreatic adenocarcinoma; Diabetes; Pancreaticoduodenectomy
The impact of medical management of type II diabetes mellitus is of great interest given its inextricable relationship with pancreatic cancer. Pancreatic cancer is the fourth leading cause of cancer death in the United States and has the highest fatality rate worldwide with the overwhelming majority (~80%) having locally advanced and/or metastatic disease [1-5]. It is well know that obesity has become an epidemic in the United States and is a major risk factor to type II diabetes mellitus [6,7]. Both obesity and diabetes have been shown to increase the risk of pancreatic cancer.
Gemcitabine has become the standard of care chemotherapeutic agent for pancreatic adenocarcinoma, but the survival benefit for patients treated with Gemcitabine in the neoadjuvant and adjuvant setting is dismal [8-11]. Complete tumor resection for pancreatic cancer is the only hope for cure and has shown to significantly improve survival particularly when achieving an R0 margin [12]. Medical management for pancreatic cancer is limited; however, medical therapy for type II diabetes is well established [13,14].
Metformin was FDA approved in 1996 for the management of type II diabetes. Metformin targets the predominant feature of type II diabetes (i.e., insulin resistance) by increasing the sensitivity of insulin. More recently, metformin has been correlated with improved survival for patients with pancreatic adenocarcinoma and has proven to inhibit pancreatic cancer cell and tumor growth [15,16]. Survival for patients who underwent pancreaticoduodenectomy for pancreatic adenocarcinoma is detailed herein. This study was undertaken to determine if patients undergoing resection for pancreatic adenocarcinoma who are taking metformin have improved survival. In undertaking this study, we hypothesized that patients taking metformin who undergo resection for pancreatic adenocarcinoma will have increased survival compared to patients with pancreatic adenocarcinoma who are not taking metformin.
Patients were entered into a secure database with Institutional Review Board (IRB) after patient informed consent. All patients undergoing an intended pancreaticoduodenectomy for pancreatic adenocarcinoma were evaluated from 1991-2013. After discharge, patients were prospectively followed.
Data were stored in Microsoft Excel (Microsoft Corp, Redmond, WA, USA) files. Statistical analysis utilized Graphpad Instat version 3.06 and Graphpad Prism 5 (Graphpad Software Inc., San Diego, CA, USA). Comparisons were undertaken using Mann-Whitney U-test or chi-squared test, and for contingency testing, Fisher’s Exact test was utilized for summing small p-values, where appropriate. Survival curve analyses were also undertaken on Graphpad Prism 5, which permitted the log-rank and Wilcoxon tests on the Kaplan-Meier survival curves. When appropriate, data are presented as median, mean ± standard deviation for illustrative purposes. Significance was accepted with 95% probability. The multiple combinations of medical therapy for their diabetes were stratified by R status, TNM score, AJCC stage, and survival for patients (Table 1).
| Diet Controlled | Metformin | Metformin + Sulfonylurea + Insulin | Sulfonylurea | Insulin | Sulfonylurea + Insulin | Metformin + Insulin | Metformin + Sulfonylurea | |
|---|---|---|---|---|---|---|---|---|
| Number of Patients | 35 | 18 | 3 | 14 | 34 | 7 | 5 | 16 |
| R status (R0/R1) | 30 (88%)/ 5 (12%) |
12 (67%)/ 6 (33%) |
2 (67%)/ 1 (33%) |
13 (93%)/ 1 (7%) |
25 (74%)/ 9 (36%) |
6 (86%)/ 1 (14%) |
4 (80%)/ 1 (20%) |
14 (88%)/ 2 (12%) |
| T-Criteria | ||||||||
| T1 | 1 (3%) | 1 (5%) | 0 (0%) | 1 (7%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| T2 | 10 (29%) | 3 (17%) | 0 (0%) | 3 (21%) | 6 (18%) | 0 (0%) | 0 (0%) | 5 (31%) |
| T3 | 22 (62%) | 13 (73%) | 3 (100%) | 10 (72%) | 27 (79%) | 7 (100%) | 5 (100%) | 11 (69%) |
| T4 | 2 (6%) | 1 (5%) | 0 (0%) | 0 (0%) | 1 (3%) | 0 (0%) | 0 (0%) | 0 (0%) |
| N-Criteria | ||||||||
| N0 | 14 (40%) | 6 (33%) | 2 (67%) | 6 (43%) | 12 (35%) | 2 (29%) | 0 (0%) | 8 (50%) |
| N1 | 21 (60%) | 12 (67%) | 1 (33%) | 8 (57%) | 22 (65%) | 5 (71%) | 5 (100%) | 8 (50%) |
| AJCC Staging | ||||||||
| IA | 1 (3%) | 1 (5%) | 0 (0%) | 1 (7%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| IB | 7 (20%) | 2 (11%) | 0 (0%) | 2 (14%) | 1 (3%) | 0 (0%) | 0 (0%) | 4 (25%) |
| IIA | 6 (17%) | 3 (17%) | 2 (67%) | 3 (21%) | 11 (32%) | 3 (43%) | 0 (0%) | 4 (25%) |
| IIB | 19 (54%) | 11 (62%) | 1 (33%) | 8 (56%) | 20 (59%) | 4 (57%) | 4 (80%) | 7 (44%) |
| III | 2 (6%) | 1 (5%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| IV | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 2 (6%) | 0 (0%) | 1 (20%) | 1 (6%) |
| Survival (Months) | 14 (27±28) | 14 (23±35) | 11 (12±2) | 20 (21±16) | 13 (13±8) | 28 (37±22) | 24 (34±26) | 11 (11±8) |
Table 1: Individualized diabetes treatment stratified by R status, T-criteria, N-criteria, AJCC stage, and survival. Where appropriate, data are presented as median (mean ± SD).
Pancreaticoduodenectomy was undertaken for 414 patients (184 men) with pancreatic adenocarcinoma with a median age of 68. One hundred and thirty-two (32%) patients had diabetes: 35 (27%) patients were diet-controlled, 18 (14%) were treated with metformin alone, 24 (18%) were treated with metformin in addition to insulin and or insulin-secretagogues (i.e. sulfonylureas), and 55 (42%) were treated with sulfonylureas and or insulin alone (Table 1). T-criteria, N-criteria and margin status were not significantly different for patients taking metformin when compared to patients taking sulfonylureas and/or insulin without metformin (Table 2). T-criteria, N -criteria and margin status did not differ for patients with diabetes who were taking sulfonylureas compared to patients not taking sulfonylureas (Table 3).
| Metformin (n=32 patients) |
Sulfonylureas/Insulin (n=55 patients) |
p-value | |
|---|---|---|---|
| T-Criteria | |||
| T1 | 2 (6%) | 1 (2%) | 0.69 |
| T2 | 5 (16%) | 9 (16%) | |
| T3 | 23 (72%) | 44 (80%) | |
| T4 | 2 (6%) | 1 (2%) | |
| N-Criteria | |||
| N0 | 11 (33%) | 20 (36%) | 0.82 |
| N1 | 21 (67%) | 35 (64%) | |
| Margin Status | |||
| R0 | 32 (76%) | 44(80%) | 0.79 |
| R1 | 10 (24%) | 11(20%) |
Table 2: Patients with diabetes taking metformin (n=32) did not have significantly different T-stage, N-stage or margin status, when compared to patients taking sulfonylureas and/or insulin without metformin (n=55).
| Sulfonylureas (Diabetic; n=patients) |
No Sulfonylureas (Diabetic; n=patients) |
p-value | No Sulfonylureas (All Patients; n=patients) |
p-value | |
|---|---|---|---|---|---|
| T-Criteria | |||||
| T1 | 1 | 2 | 0.19 | 23 | 0.46 |
| T2 | 8 | 19 | 75 | ||
| T3 | 31 | 37 | 297 | ||
| T4 | 0 | 4 | 18 | ||
| N-Criteria | |||||
| N0 | 18 | 32 | 0.33 | 152 | 0.39 |
| N1 | 22 | 60 | 262 | ||
| Margin Status | |||||
| R0 | 35 | 71 | 0.24 | 326 | 0.28 |
| R1 | 5 | 21 | 87 |
Table 3: Patients taking sulfonylureas did not have significantly different T-criteria, N-criteria or margin status, when compared to patients with diabetes not taking sulfonylureas or patients with or without diabetes not taking sulfonylureas.
Survival for patients with diabetes did not differ from patients without diabetes (Figure 1).
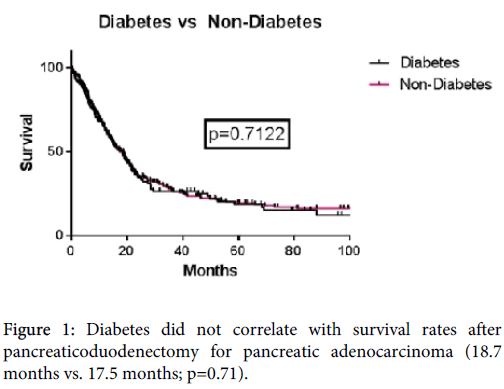
Figure 1: Diabetes did not correlate with survival rates after pancreaticoduodenectomy for pancreatic adenocarcinoma (18.7 months vs. 17.5 months; p=0.71).
Patients with diabetes treated with metformin did not have improved survival compared to patients with diabetes not treated with metformin (Figure 2).
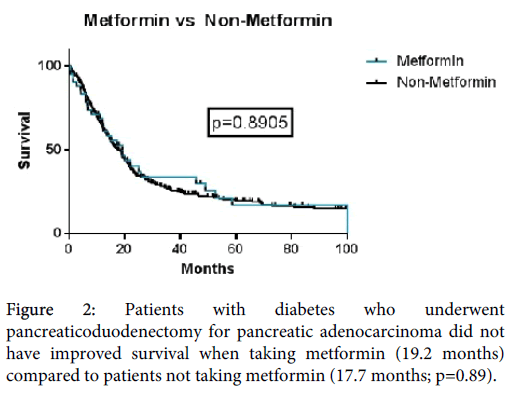
Figure 2: Patients with diabetes who underwent pancreaticoduodenectomy for pancreatic adenocarcinoma did not have improved survival when taking metformin (19.2 months) compared to patients not taking metformin (17.7 months; p=0.89).
The impact of insulin was not significant when compared to patients with diabetes not taking insulin (Figure 3).
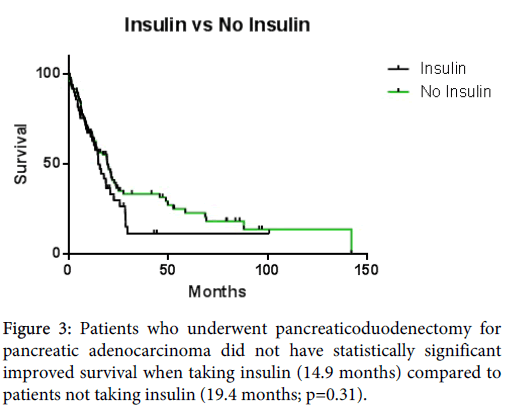
Figure 3: Patients who underwent pancreaticoduodenectomy for pancreatic adenocarcinoma did not have statistically significant improved survival when taking insulin (14.9 months) compared to patients not taking insulin (19.4 months; p=0.31).
Patients with diabetes who underwent pancreaticoduodenectomy for pancreatic adenocarcinoma treated with sulfonylureas had improved survival compared to patients not treated with sulfonylureas (27.5 months vs.14.6 months; p<0.05) (Figure 4).
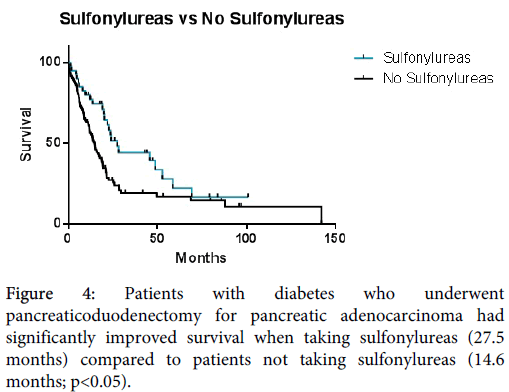
Figure 4: Patients with diabetes who underwent pancreaticoduodenectomy for pancreatic adenocarcinoma had significantly improved survival when taking sulfonylureas (27.5 months) compared to patients not taking sulfonylureas (14.6 months; p<0.05).
Patients who underwent pancreaticoduodenectomy for pancreatic adenocarcinoma with or without diabetes treated with sulfonylureas had significantly improved survival compared to patients not treated with sulfonylureas (27.5 months vs. 16.4 months; p<0.05) (Figure 5).
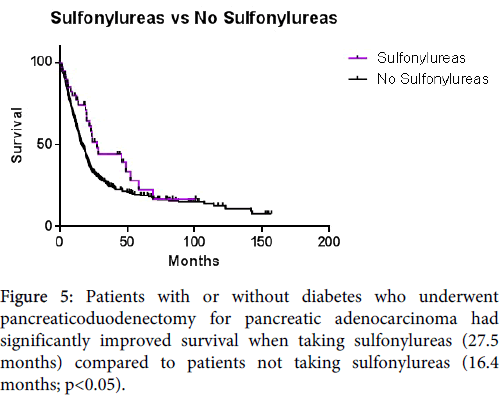
Figure 5: Patients with or without diabetes who underwent pancreaticoduodenectomy for pancreatic adenocarcinoma had significantly improved survival when taking sulfonylureas (27.5 months) compared to patients not taking sulfonylureas (16.4 months; p<0.05).
This study was undertaken to evaluate the potentially beneficial effect of metformin on survival for patients with resectable pancreatic adenocarcinoma. In undertaking this study, we concluded that patients who undergo pancreaticoduodenectomy for pancreatic adenocarcinoma who are taking sulfonylureas with or without other therapy have improved survival compared to patients not taking sulfonylureas. Metformin does not appear to be beneficial for patients with resectable disease, but may have a benefit for patients with unresectable and/or metastatic disease as prior studies showing survival benefits with metformin had patients with advanced disease. The patients in this series all underwent pancreaticoduodenectomy for resectable pancreatic adenocarcinoma. Our patient population was gender-balanced with a distribution being nearly equal. The age of patients was similar to that reported in other series. The majority of patients did not have diabetes and the majority of patients with diabetes were treated with sulfonylureas/insulin alone. Diabetes was not an independent predictor of survival.
Recently, with the availability of long-term data, the use of metformin for patients with diabetes has been found to be associated with a decreased risk for any cancer [17]. Furthermore, metformin is correlated with improved survival for patients with pancreatic adenocarcinoma; however, the vast majority of these patients studied have metastatic or locally advanced pancreatic cancer, which precluded resection [16]. Contradictory to the aforementioned study, our study shows there is no survival benefit for patients with diabetes taking metformin who underwent resection for pancreatic adenocarcinoma. Prior studies have shown that metformin use not only has a beneficial effect, but that sulfonylureas and/or insulin have a detrimental effect [18]. Therefore, in the early portions of our study, we grouped patients treated with sulfonylureas and/or insulin, as sulfonylureas have been postulated to impart the same risk as insulin since sulfonylureas are insulin-secretagogues [7,19]. When comparing patients without diabetes who have pancreatic cancer compared to patients with short-term (<2 years) or long-term (>2 years) diabetes, neither tumor size nor tumor location differ. However, pancreatic cancer in patients with long-term diabetes have an increased rate of resectability and the lowest rate of extrapancreatic extension of their tumors [20]. In our study, the salutary impact of metformin on survival for patients with pancreatic adenocarcinoma is lost when the cancers are resectable and the use of sulfonylureas is associated with longer survival. Tumor criteria and margin status continue to be the overriding predictors of survival for patients with resectable pancreatic adenocarcinoma when considering metformin therapy for patients with resectable disease.
The proposed mechanism for metformin as an anti-cancer agent is multifactorial. Metformin ameliorates hyperglycemia/hyperinsulinemia, activates the epidermal growth factor receptor (EGFR), and activates AMP/MAP-kinase, which therefore inhibits the mammalian target of rapamycin (mTor) pathway [21]. Metformin may be a potential adjunct to current chemotherapeutic strategies, particularly targeted therapy of the EGFR or mTor pathway. Combined approaches with EGFR inhibitors with metformin are potential synergistic novel therapeutic strategies for pancreatic adenocarcinoma. Results are pending of a phase II, randomized, placebo controlled study to evaluate the efficacy of the combination of gemcitabine, erlotinib and metformin for patients with locally advanced and/or metastatic pancreatic adenocarcinoma by a group in Amsterdam.
Reinventing currently administered medications can expedite the approval process for cancer therapy, as the safety profile has already been proven with historical data. Metformin is potentially the newest adjunct to cancer therapy by reinvention. For patients with resectable cancer, however, it appears that improvement is more dependent on previously known prognostic factors, such as margin status and TNM staging, and the potential benefits of metformin alone are lost for patients with resectable disease. Further investigation is warranted, however, for locally advanced and metastatic disease, as well as synergistic therapy with metformin for patients with resectable pancreatic adenocarcinoma, especially given its historically safe drug profile.
Obesity is epidemic in the United States and there is an associated rise in type II diabetes mellitus, and as previously stated, there is a relationship between diabetes and pancreatic cancer. There have been numerous reports of the detrimental effects of obesity, particularly visceral fat on cancer survival [22-24]. Furthermore, diabetes increases cardiovascular risks and has a particular interlaced relationship with pancreatic cancer diagnosis and prognosis. A recent meta-analysis identified a 31% reduction in overall cancer incidence or mortality when metformin is used as treatment for diabetes [25]; however, more studies are needed to define the impact metformin and other diabetic therapies have on survival.
This study is novel in that patients treated with sulfonylureas (not metformin) have an improved survival compared to patients not treated with sulfonylureas. Studies to date have suggested that metformin is associated with a better prognosis in patients with pancreatic adenocarcinoma and that sulfonylureas have an increased risk of cancer, although this has not been corroborated with randomized control trials [26]. Less is known, however, about the prognostic effect of sulfonylureas for patients with cancer and furthermore, specifically for pancreatic adenocarcinoma. The realm of diabetes and pancreatic adenocarcinoma continues to be complex and further investigation is warranted not only on the effects of obesity and diabetes, but also the effects of metformin and sulfonylureas on cancer-specific outcomes.