Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Review Article - (2016) Volume 6, Issue 2
Pancreatic transplant is increasingly being performed for management of diabetes. There are known complications, specifically related to exocrine drainage of the pancreas, with enteric versus bladder drainage being options. Here we present a unique complication of leakage of the pancreaticocystostomy, likely secondary to severe urethritis and obliteration of the urethra. Accumulation of pancreatic enzymes in the subcutaneous tissues led to fat necrosis of the scrotum and groin with severe systemic inflammatory response syndrome. Presentation mimicked an infectious soft tissue infection that failed antibiotic management. This highlights a unique clinical entity mimicking infection. This patient required debridement, urinary diversion, and a multidisciplinary approach to treatment.
<Keywords: Pancreas transplant, Leak, Subcutaneous, Fat necrosis, Bladder drainage
Pancreas transplant is becoming an increasingly effective option for treating diabetes mellitus. A variety of complications can result, including problems with exocrine drainage of the pancreas. We present a case of a leak from a bladder-drained, transplant-pancreas into the perineum causing extensive fat necrosis. To our knowledge, this is the first such report of this complication from bladder drainage of a pancreas transplant.
This is a case of a 51 year old male with a history of kidney-pancreas transplant who presented with erythema, warmth, and swelling of the scrotum for 2 months. His medical history includes end stage renal disease secondary to diabetes mellitus treated with a simultaneous kidney transplant with pancreaticocystostomy 14 years ago. He had a complicated surgical history, undergoing enteric conversion 7 years ago secondary to severe urethritis, and then conversion back to bladder drainage 1 year ago due to multiple intra-abdominal infections. His kidney was poorly functioning with decreasing urinary output in the month prior to presentation and the patient is undergoing tri-weekly dialysis via a tunnelled haemodialysis catheter. Pancreas function was good, and the patient did not require supplemental insulin.
History of present illness included multiple rounds of antibiotics at outside institutions for presumed scrotal cellulitis without resolution of his symptoms. He experienced subjective fevers at home, but otherwise felt well with only mild pain of the scrotum. On exam he was noted to have a severely oedematous scrotum and suprapubic fullness. His abdomen was otherwise soft and non-tender. Digital rectal exam revealed normal prostate. Initial laboratory analysis revealed leukocytosis of 14,300 /uL, urine amylase of 70,058 U/L, and serum amylase of 1,171 U/L. Initial blood and urine cultures were negative. Computerized axial tomography scan of the pelvis revealed scrotal thickening and multiloculated fluid collections of the scrotum and perineum (Figure 1 - left). A distended bladder was also noted.
A CT cystogram was also attempted to evaluate for an anastomotic leak, but a Foley catheter was unable to be placed by nursing staff and urology physicians at the bedside. Therefore catheter placement was attempted with bedside flexible cystoscopy that revealed strictures of the urethra with multiple false passages and extensive tissue destruction within the urethra. Scrotal edema worsened and new suprapubic fullness was noted immediately following the procedure suggesting that irrigation may be leaking into the perineal subcutaneous tissues. Plans were made for suprapubic catheter placement to divert his urine and pancreatic enzymes. In the interim, he became increasingly febrile to 102.2° F with tachycardia to 120 beats per minute and hypotensive to 82/47 mm Hg. His scrotal erythema spread to his right groin and thigh. Therefore he was taken to the operating room for debridement of the scrotum, right groin, and thigh as well as suprapubic catheter placement. Aerobic, anaerobic, acid-fast and fungal cultures of the debrided tissues were negative. Pathology of debrided tissues revealed fibroadipose tissue with fat saponification, extensive necrosis, and inflammation.
He remained hypotensive, on continuous renal replacement therapy and required intensive care for 48 hours post-operatively. This improved, and a diagnosis of pancreatic fat necrosis was considered. Antibiotics were stopped on post-operative day five. Approximately one week later he returned to the operating room for repeat cystoscopy and further debridement of his right thigh and left perineum. Debridement was once again consistent with fat necrosis and with bacterial cultures once again being negative. Rigid urethroscopy was significant for an obliterated bulbar urethra with multiple false passages and no apparent true lumen. Therefore, a retrograde urethrogram was performed to determine whether the urethra and the bladder were in continuity. Retrograde urethrogram did reveal a severe stenosis of the urethra with minimal contrast reaching the bladder (Figure 1 – right). Flexible cystoscopy via the prior suprapubic tract allowed the antegrade passage of a wire from the bladder to the urethra, and subsequent urethral catheter placement over the wire.
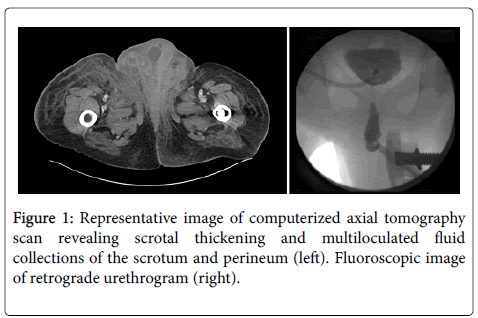
Figure 1: Representative image of computerized axial tomography scan revealing scrotal thickening and multiloculated fluid collections of the scrotum and perineum (left). Fluoroscopic image of retrograde urethrogram (right).
The remainder of his hospital course consisted of complex wound care (Figure 2) with intermittent debridements, continuation of Foley catheter bladder drainage, and increasing physical therapy. All blood, urine, and tissue cultures remained negative for microbes throughout his stay. Urine output improved significantly, with greater than one liter of urine output per day. Although amylase levels were not evaluated on his tissue biopsies, the presumed diagnosis in this patient was fat necrosis secondary to pancreatic enzyme leak from the damaged urethra or duodenocystostomy.

Figure 2: Debrided wound of the right groin.
With over 37,000 performed worldwide, the incidence of pancreas transplant for management of diabetes is increasing [1,2]. Controlling pancreatic exocrine secretion is a critical part of management. Bladder drainage allows physicians to monitor urinary amylase levels for signs of rejection. While bladder drainage is thought to be safer than enteric drainage, if a leak were to occur, is not without its own set of complications. Metabolic acidosis, recurrent urinary tract infections, and dehydration are frequent reasons for enteric conversions in up to one-third of patients [3]. Enteric drainage is sometimes preferred as it is considered more physiologic; however, it can be associated with bowel perforation, leakage of pancreatic enzymes and sepsis. Overall, complications associated with bladder drainage do not have as negative an impact on patient and pancreas graft survival when compared to enteric drainage [4].
Soft tissue infections occur more frequently in patients with diabetes and immune compromise [5]. The standard of care for soft tissue infections is drainage, microbial cultures, and appropriately tailored antimicrobials [6]. Pancreatic enzymes leaking into the subcutaneous tissues are an extremely rare phenomenon, but can present as a soft tissue infection. An alternative diagnosis of culturenegative infection is a possibility. This patient’s clinical scenario, fat saponification on tissue biopsy, and lack of improvement on previous antibiotics would suggest pancreatic fat necrosis. However, we do acknowledge atypical organisms are possible, especially in immunecompromised patients, and may not grow in routine culture media [7]. One should consider the diagnosis of pancreatic-enzyme fat necrosis, in the setting of pancreatic pathology, especially when patients fail to respond to antibiotics.
In conclusion, pancreatic transplant remains a valuable procedure for improving quality of life for those with type 1 diabetes. Several complications following pancreatic transplant beyond graft rejection have been previous described in the literature. However, this is a unique, rare case in which the exocrine leak from a transplanted pancreas resulted in extravasation into the surrounding soft tissues causing extensive fat necrosis. This patient will require a complex urethral reconstruction with possible buccal grafting to regain volitional urethral voiding. Given the aggressive and dangerous nature of this complication, health care practitioners should have a low threshold of suspicion when seeing patients with this kind of surgical history and clinical presentation.