Angiology: Open Access
Open Access
ISSN: 2329-9495
![]() +44 1478 350008
+44 1478 350008
ISSN: 2329-9495
![]() +44 1478 350008
+44 1478 350008
Research Article - (2018) Volume 6, Issue 4
Objective: Immersion induced hydrostatic pressure on thoracic cavity and limbs is one kind of cardiac overload model in simulating microgravity. We evaluated immersion hemodynamic parameters, investigated in vitro stretching induced aortic intact wall windkessel adaptations in whole-body immersion mice.
Method: Kunming mice were divided into immersion group (n=20) and control group (n=10) randomize. In immersion group, mice further divided into immersion group (n=10) and immersion with weight-bearing group (5% of body weight, n=10). The immersion kept 20 min/day in warm water and continues for 1 week. The hemodynamic parameters were collected by left carotid artery cannulation and analyzed by biological signal acquisition system. Calculi of percussion wave were calculated with integral mode to determine left ventricle stroke volume. In vitro aortic wall were prepared to a vascular ring and mechanical stretching the preparation to 1 g as the initial load. The preparations were further stretched by a micro-adjusting tuner with the interval of 5 min which gradually increasing 1 mm in each step. The stretching induced passive tension, where after, stress relaxation duration and myogenic spontaneous contraction were analyzed. In a separated preparation, myogenic contraction changes investigated in 0.05% Nitrendipine treated preparation.
Result: Mice carotid arterial pressure waveforms have significantly changed, however, mean arterial pressure were slightly increased but not significantly (immersion 9.14 ± 0.63 kPa, control 8.40 ± 0.97 kPa). The calculated stroke volume increased significantly (immersion 13.96 ± 0.12 μl/min, control 5.14 ± 0.69 μl/min, respectively). In vitro mechanical stretching induced less myogenic spontaneous contraction, stress relaxation period were shortening. Pre-treatment of 0.05% Nitrendipine induced more myogenic spontaneous contraction that revealed the spontaneous contraction was not solution Ca2+ influenced.
Conclusion: Immersion stress improved left ventricle functions that reflected in rapid ejection and isodiastolic period, suggested aortic windkessel properties were improved in microgravity simulation induced cardiac overload.
Keywords: Whole-body immersion; Dicrotic notch; Aortic windkessel properties
Whole-body immersion is an experimental method to simulate fluid redistribution in microgravity environment and to testing circulation overloading induced cardiovascular response during redistribution [1]. The immersion hydrostatic pressure enhanced thoracic cavity and limbs circulation volume and pressures, induced cardiac output and peripheral resistance increasing [2], pulse pressure increased [3], however, the heart rate were decreased. This also significantly influenced in respiratory circulation, increased volume return circulation volume enlarged inferior vena cava and diameter of brachial artery [4]. The developed computed tomography angiography (CTA) technologies indicated the possibility to obtain non-invasive high-quality imaging in diagnosis and grading of vascular stenosis induced local fluid redistribution relative fluid pressure variations, such as the skull base cerebrospinal fluid pressure monitoring [5,6]. Furthermore the time resolved imaging of contrast kinetics (TRICKS) MR angiography (MRA) imaging development traduced the possibility to evaluate vasculature of arteriovenous malformations in arteriovenous malformations induced local fluid redistribution [7]. All of such vascular malformation difference on imaging information and the vascular stiffness variations induced the local body fluid redistribution were harmed haemodynamic waveforms and relative to the onset of the pulse wave to the dicrotic notch of the aortic waveform [8,9].
Dicrotic pulse in aortic waveform is an important index for understanding ventricular ejection and aortic compliance. It is formed by ventricular ejection and aortic elastic contraction in cardiac cycle. The former is related to the characteristics of ventricular contraction, the latter is related to aortic wall Windkessel properties. The descending isthmus in the pressure waveform (dicrotic notch) is the most important index for understanding ventricular ejection and aortic Windkessel properties. Dicrotic notch, the descending point between two pressures, is the pressure rebound when the blood flow ejected from the left ventricle after aortic valve closure and meets the circumferential resistance flowing back to the ventricle. The dicrotic notch incisura is the intersection of left ventricular systolic and diastolic phases on the time axis. The formation of wave isthmus is because of resistance in reduced ejection phase and cardiac ventricle is shifting from reduced ejection phase to isovolumetric diastolic phase. This resistance to reduced ejection can reflect the magnitude of the peripheral resistance which represented cardiac ventricular afterload.
In this study, for understanding microgravity simulation induced ventricular ejection function and Windkessel property adaptation, we investigated hemodynamic pressure waveforms, evaluated the mechanical stretching induced Windkessel property adaptation in isolated aortic wall preparations in whole-body immersion exercise mice.
4-week-old male Kunming mice (Specific Pathogen Free) were randomly divided into immersion group (n=10), immersion with weight-bearing group (weight-bearing 5% of body weight, n=10) and control group (n=10). Mice were represented by Hainan Provincial Center for drug safety assessment and the animal feeding during immersion exercises were according to Hainan province regulations on management of medical laboratory animals. The experimental protocols were approved by the Animal Care and Protection Committee of Hainan Medical College. Immersion mice were placed in a water depth of 35 cm tank in 25°C. The mice lower limbs were touched by a rod to maintain its movement and kept the body floating for 20 minutes per day. The immersions exercised were continued for 1 week. The immersion weight-bearing mice were loaded by 5% of the body weight during immersion.
After the immersion exercised courses, mice were anesthetized with 3% pentobarbital sodium (0.1 mL/20 g body weight, intraperitoneal injection) and supine position fixed on the wood board. Left common carotid artery was cannulated to monitoring blood pressure and waveforms by BL420S biological signal acquisition system (Chengdu Taimeng Technology Co. Ltd., Chengdu, China). Systolic and diastolic pressure, heart rate and mean arterial pressure (MAP) were investigated by analyzing the waveform. According to the characteristic of cardiac stroke notch generated by aortic regurgitation at the end of inspiration and the beginning of expiration, left ventricle stroke volume was obtained by integral calculation of percussion waves at the end of inspiration and the beginning of expiration. The percussion waves were randomly selected to obtain the median value of the integral. The median value was taken as the reference value of the stroke volume of the left ventricle (SV).
In vitro aortic wall were harvested near the ventricular connected segment. Under binocular anatomical microscope (PXS-2040, Shanghai optical instrument factory, Shanghai, China). After removing connective tissue outer layer of aortic wall, the aorta wall ring was prepared and bath in Ringer’s solution, 37°C. The aortic wall mechanical stretching test system were consisted with a micro-step tuner, tension transducer (JZ-100, Beijing aerospace medical engineering institute, Beijing, China) and a cast iron stabilizer. The system is installed on a vibration isolation platform (ST10-08, Jiangxi Liansheng experimental equipment Co. Ltd., Shang Rao, China) to avoid environmental vibration interference. The stretching induced passive tension, stress relaxation duration and myogenic spontaneous contraction were analyzed by BL-420S biological signal acquisition and processing system.
The aortic wall preparations were directly fixed on two stainless hooks. The micro-step tuner was adjusted to keep the specimen relaxed horizontally for 5 minutes in Ringer 's solution. Adjusting the microstep tuning to stretch the aorta preparation until the preparation passive tension arrive to 1 g. The preparation length at this moment is the initial length (L0), and the 1 gram is the preload of the aorta preparation. The preparations were further mechanical stretched 1 mm in length along the horizontal direction (length L0+1). The active stretched maximum passive tension (PTmax), and the following sustained static stretch induced passive tension deceleration curves were recorded. The preparations were rapidly active stretched 10 steps with the length of 1 mm for each step, and stable for 5 min between each step. The sustained static stretch after PTmax induced deceleration time of the preparations in Ringer ’s solution (T), as well as in pretreated with 0.05% Nitrendipine (N-T) were evaluated; furthermore the sustained static stretch induced myogenic spontaneous rhythmic contraction maximum amplitude in Ringer ’s solution (SRCmax), as well as in 0.05% Nitrendipine pre-treated (N-SRCmax) and the relative compliance (C, C=ΔPT/L, in which ΔPT was the decelerated passive tension, L was the increased length by stretching) were evaluated.
Statistics
In the immersion exercise experiment, the mean ± SEM values of each haemodynamic parameter between normal immersion mice group (referred to as immersion group) and normal mice without immersion control group (referred to as control group), weightbearing immersion mice group (referred to as weight-bearing immersion group) and control group, as well as the difference between immersion group and weight-bearing immersion group were statistically compared by student t-test, statistically highly significant as p<0.001.
The percussion wave and dicrotic wave were distinguished from aortic wave during ventricular diastole and systole. The typical waves were as show in Figure 1a. The systolic and diastolic pressure waveforms of the common carotid artery in control group were regularly. However, the waveforms fluctuated up and down with tidal breathing strengthened percussion wave and dicrotic wave, so that at the end of inspiration and the beginning of expiration, the percussion wave and dicrotic notch incisura was the clearest, which can divided dicrotic wave from notch incisura (Figure 1b). Mice common arterial pressure waveforms in immersion group and immersion weightbearing group were different from those in control group, mainly manifested in prolongation of systolic and diastolic duration, increase of percussion wave amplitude and downward shift of dicrotic notch incisura (Figure 1c). Common arterial pressure (PA) were significantly increased in immersion groups.
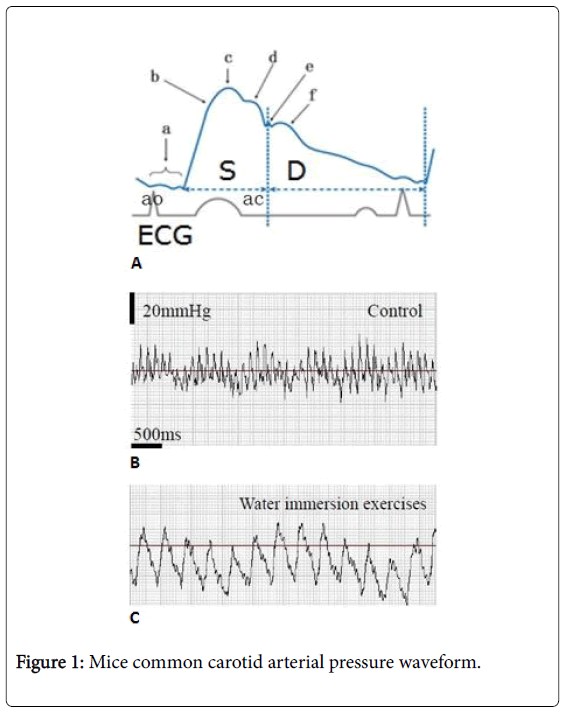
Figure 1: Mice common carotid arterial pressure waveform.
Mice MAP value in immersion group was slightly higher than that of control group, however there was no statistic significant difference between groups (Figure 2a). The relative left ventricular cardiac output (SV) were determined by integral calculated of common carotid pressure waveform. It was indicated that SV value were significantly increased in immersion groups (Figure 2b, a*** was the comparing between immersion group and control group, b*** was the comparing between immersion weight-bearing group and control group), however, the stroke volume in immersion groups were significantly increased (Table 1, ***c was immersion group compared with control group, ***d was immersion weight-bearing group compared with control group). The cardiac output is the parameter relative to the heart rate, the heart rate in immersion groups were decreased, however no significant different between immersion groups and control group.
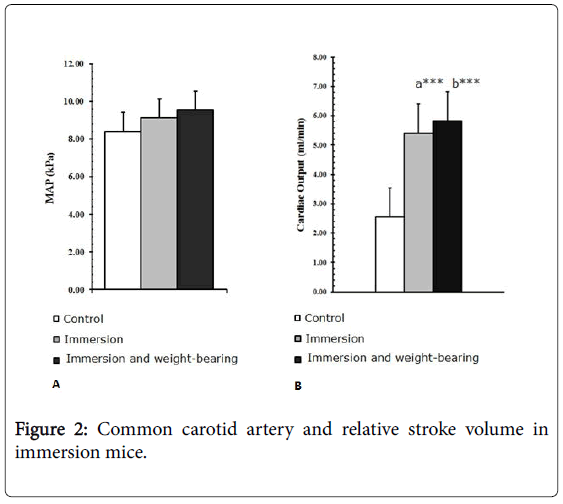
Figure 2: Common carotid artery and relative stroke volume in immersion mice.
| Item | Control (n=10) | Immersion (n=10) | Weight-bearing group immersion (n=10) |
|---|---|---|---|
| PA (SP/DP, kPa) |
11.37/6.31 | 14.62/6.95***a | 13.60/7.69***b |
| MAP (kPa) |
8.40 ± 0.97 | 9.14 ± 0.63 | 9.55 ± 0.83 |
| SV (μl/ml) |
5.14 ± 0.69 | 13.96 ± 0.12***c | 13.86 ± 0.21***d |
| HR | 495.87 ± 52.80 | 387.09 ± 32.41***,e | 420.12 ± 37.11 |
a,b were the significantly difference of systolic and diastolic pressure in common carotid artery that compared between immersion group and weight-bearing immersion group to the control group respectively; c, d were the significantly difference in left ventricle stroke volume that compared between immersion group and weight-bearing immersion group to the control group respectively; e was the heart rate significantly difference between immersion group and control group; *** means p<0.001.
In Table 1, the symbol *** was immersion group compared with control group, ***b was immersion weight-bearing group compared with control group.
Table 1: The hemodynamic parameters in immersion mice common carotid artery.
In the in vitro experiment of isolated aortic preparations in Ringer’s solution, the sustained static stretch induced passive tension deceleration time (T) was significantly shortened both in immersion group and weight-bearing immersion group. Figure 3 was the active stretch induced passive tension myograph in control and normal immersion mice in low and high active stretching conditions; panel A was the preparations in Ringer’s solution, panel B was in Nitrendipine pre-treated preparations. In Figure 3A, a) initial active stretch, b) low active stretch and c) high active stretch; however, e) and f) was the normal immersion mice aortic preparation myograph in low and high sustained static stretch condition. Table 2 was the summary of aortic preparation elasticity relative parameters. For understanding the aortic elastic variations in high preload stretch condition, we focused the stretch relative analysis in high sustained static stretch conditions. In Table 2, were the preparations in Ringer’s solution. Symbol ***a was the PT deceleration time (T) comparing between immersion group and control group preparations, ***b was the comparing between weight-bearing immersion group and control group preparations. In both type of immersion mice in high sustained static stretch, T were significantly shortened when comparing with control mice respectively (*** means p<0.001). The aortic preparation myogenic spontaneous rhythmic contraction maximum amplitude during PT deceleration (SRCmax) was significantly decreased in two type of immersion group in low sustained static stretch (L0+1), as well as in high sustained static stretch (L0+11). The symbols ***c and d in Table 2﴾1﴿ were the immersion and weight-bearing immersion mice preparations comparing to control mice respectively. The relative compliance value (C) was decreased in normal immersion mice preparations when comparing to control mice preparations (symbol e in Table 2﴾1﴿), however aortic preparations from weight-bearing immersion mice were significantly improved (symbol f in Table 2﴾1﴿ when comparing to control mice preparations).
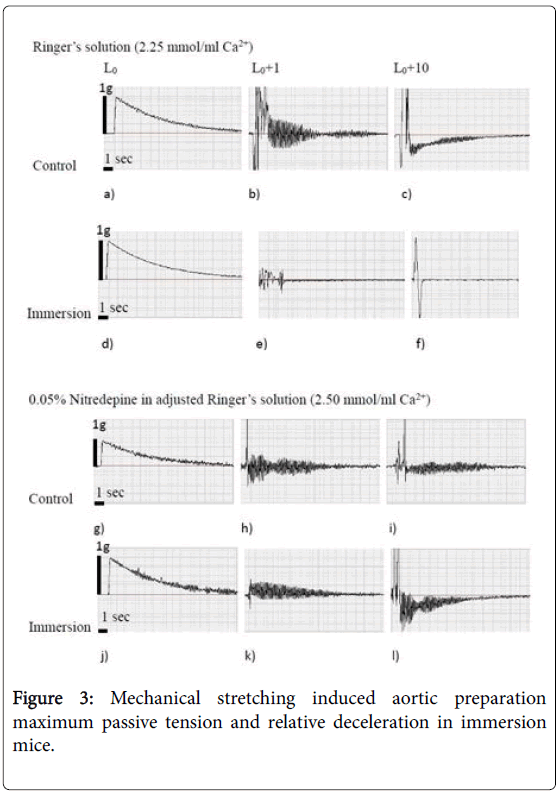
Figure 3: Mechanical stretching induced aortic preparation maximum passive tension and relative deceleration in immersion mice.
| Item | Control (n=5) | Immersion (n=5) | Weight-bearing immersion (n=5) | |||
|---|---|---|---|---|---|---|
| L0+1 | L0+11 | L0+1 | L0+11 | L0+1 | L0+11 | |
| ﴾ 1﴿ T(sec) | 6.56 ± 1.10 | 10.88 ± 1.95 | 3.38 ± 0.91 | 1.98 ± 0.32***a | 3.84 ± 0.21 | 2.16 ± 0.25***b |
| ﴾ 2﴿ N-T (sec) | 8.17 ± 1.88 | 10.02 ± 0.92 | 9.74 ± 1.19 | 9.20 ± 0.42 | 9.18 ± 0.91 | 8.14 ± 0.67 |
| ﴾ 1﴿ SRCmax(g) | 0.81 ± 0.02 | 0.32 ± 0.09 | 0.05 ± 0.01 | 0.04 ± 0.01***c | 0.04 ± 0.01 | 0.03 ± 0.01***d |
| ﴾ 2﴿ N-SRCmax (g) | 0.60 ± 0.03 | 0.75 ± 0.69 | 0.58 ± 0.11 | 0.83 ± 0.16 | 0.60 ± 0.19 | 0.77 ± 0.15 |
| ﴾ 1﴿ C | 0.32 ± 0.07 | 1.87 ± 0.39 | 0.46 ± 0.10 | 0.48 ± 0.12***e | 0.52 ± 0.85 | 1.91 ± 0.61***f |
| ﴾ 2﴿ N-C | 0.34 ± 0.11 | 1.82 ± 0.22 | 0.35 ± 0.33 | 9.17 ± 0.43***¶ | 0.48 ± 0.22 | 1.79 ± 0.31 |
In Table 2, the symbols ﴾ 1﴿ was the measurement of parameters of aortic wall preparations in Ringer's solution; ﴾ 2﴿ was in 0.05% Nitrendipine pre-treated; N-T: passive tension deceleration time in Nitrendipine pre-treated preparations, N-SRCmax: myogenic spontaneous rhythmic contraction maximum amplitude in Nitrendipine pre-treated preparations, N-C: the preparation compliance of Nitrendipine pre-treated.
The citation symbol a and b were the preparation from immersion mice and weight-bearing immersion mice that compared to control group respectively. A shortening of T value were significantly indicated in immersion and weight-bearing immersion mice in high static sustained stretch condition; c and d indicated significantly decreasing of SRCmax value in immersion and weight-bearing mice when comparing with control mice in high static sustained stretch condition; However, Nitrendipine significantly improved immersion mice preparation compliance in high static sustained stretch condition when comparing with control (symbol $); ***p<0.001.
Figure 2: Common carotid artery and relative stroke volume in immersion mice.
In the in vitro experiment of isolated aortic preparations pre-treated with 0.05% Nitrendipine for 5 minutes, the sustained static stretch induced passive tension deceleration time (N-T) were no significantly changes in immersion groups (the myograph were in Figure 3B, comparing between waveform of k and h, l and i). In Table 2, ﴾2﴿ was the immersion and weight-bearing immersion aortic preparations elasticity relative parameters that were pre-treated with 0.05% Nitrendipine. Both immersion type mice preparation N-T (PT deceleration time after Nitrendipine pre-treated) had no significant difference when comparing with control respectively. Nitrendipine slightly decreased the N-SRCmax (aortic preparation myogenic spontaneous rhythmic contraction maximum amplitude during PT deceleration after Nitrendipine pre-treated) in control mice preparation (comparing between Figure 3B and 3A; h to b, i to c). However, Nitrendipine was significantly increasing N-SRCmax in immersion mice preparation both in low and high sustained static stretch (Figure 3B, the immersion mice preparation k, l comparing to control mice preparation h, i in low and high sustained static stretch condition respectively; ***means p<0.001). Nitrendipine pre-treated aortic preparation compliance (N-Cmax) were significantly improved in immersion mice. In Table 2﴾2﴿, N-SRCmax value significantly increased in normal immersion mice aortic preparations when comparing with control mice (symbol , ***means p<0.001), however, no significantly improve in weight-bearing immersion mice preparations.
In systemic circulation system, mean arterial pressure reflects the blood perfusion volume in cardiovascular system [10]. The mice simulation experiment suggested that 1 week whole-body immersion did not significantly increasing the total blood volume in cardiovascular system. However the stroke volume significantly increased, because of blood return volume increased (Table 1c,d). This increased blood volume was recognized increased hydrostatic pressure by whole-body immersion. The same results were also observed in heart failure patient water gymnastics report [11]. The mice experiment data revealed that whole-body immersion induced redistribution decreased the heart rate, which further increased the stroke volume (Figure 2b). The immersion induced heart rate decreasing was frequently reported in diving workers. The so-called diving reflexes were through the vagus afferent route [12] to generate the negative chronotropic action, further decreased cardiac output [13]. In our experiment the decreased heart rate were observed in normal immersion mice; however, the statistic difference were not found. Immersion induced significantly increasing of mice left ventricular stroke volume. This further enhanced aorta Windkessel properties and stabled the peripheral resistance. In diastole and systole pressure wave circles, dicrotic waves were generated by the blood flow in aorta in ventricle diastolic phase directly after blood ejection [14]. Dicrotic waves were because of the elasticity of the aorta wall and recoils back the blood flow to peripheral for maintain the systemic pressure. When the elastic recoil of expanded aorta overcome the decreasing pressure in the left ventricle, aortic valve closed and this gives rise to dicrotic notch and this property is known as Windkessel effect. In whole-body immersion mice, blood redistribution induced diastole volume overload further improved aortic elasticity and Windkessel properties. This is characterized by significantly declined dicrotic notch incisura and obviously a positive effect on systemic pressure stable during diastole phase.
The aorta wall passive mechanics depend on integrity of elastic fiber, vascular smooth muscle and intima to realize the Windkessel effect [15]. The aorta wall preparation elasticity were varied under different length stretch preload. When the preparation were settled under server mechanical stretching conditions, its elasticity and compliance were reflected by its maximum passive tension created tension decelerations. During the tension attenuation, stretched elastic aorta wall were coupled to the rigid stainless hooks to obtain an explicit decelerations curve that included several important information about aortic wall elastic properties. In this mice immersion model, aorta elastic properties derived Windkessel function exhibit a critical role in adaptation to cardiac overload caused by blood redistribution in immersion mice. First is the aortic wall tension deceleration time, after rapid length stretching and transient maximum passive tension, was significantly shortened in whole-body immersion mice, moreover an enhancing of myogenic spontaneous contractions were observed during deceleration. Although the myogenic spontaneous during deceleration were potentially generated during mechanical stretch and easily evoked by blocking L-type calcium channel and other voltagedependent calcium channels (0.05% Nifedipine pre-treated). The aortic wall accommodated to the blood volume overload through attenuating stiffness and evoking myogenic spontaneous tension to fit the stretching overloading. The second is aortic wall represented an enhanced dicrotic notch amplitude and a downward shift of incisura at beginning of diastole in vivo .
Considering the significant increase of left ventricular stroke volume and the dicrotic notch amplitude and a downward shift of incisura in immersion mice, it can be concluded that the aortic compliance of mice in vivo was improved (C value becomes to larger, Table 2), especially under the increased length stretch preload (for example, at the length of L0+10).
The function of elastic reservoir of aorta is related to myogenic spontaneous contraction [16]. Although the myogenic spontaneous contraction in immersion mice aortic decreased significantly, Nifedipine blockade evoked the myogenic activity in this kind of preparation. In some previously reports it was suggested that blocking calcium channel receptor were functional correlation to inhibition of portal vein myogenic activity [17], but the mechanisms were not clear. In our aortic preparations, the Nifedipine evoked myogenic spontaneous contraction responses either in low stretch loading or in high loading. The evoked myogenic activities not only in immersion mice but also presented in control mice. Nitrendipine was a nonselected calcium channel blockade, which blocked L-type calcium channel and other voltage-dependent calcium channels. Nifedipine has additionally been found to act as an antagonist of the mineralocorticoid receptor, or as an antimineralocorticoid [18]. Some reports suggested that mineralocorticoid receptor antagonist did not reduce vascular smooth muscle myogenic tone, but prevented Ca2+ influx through L-type voltage-gated Ca2+ channels [19]. This indicates that the change of Ca2+ permeability in aortic smooth muscle was not the only pathway to increasing myogenic spontaneous contraction in stressed aorta. There were other signalling pathway to increasing the aortic wall myogenic activities and improving aortic Windkessel functions.
In this simulation model, water temperature was not important for investigating the blood redistribution [20]. However, hydrostatic pressure was the major factor for blood returning. Strengthen underwater exercise may cause a sharp increase in central blood flow, reduce aortic compliance, impair left ventricular diastolic function, and even reduce ventricular contraction and cardiac output [21-23]. For getting the better blood redistribution effect, monitoring of respiratory movement was also important because positive pressure breathing in water can lead to a decrease in mean arterial pressure and cardiac output and an increase in peripheral resistance [24]. The ascending branch of aorta has the closest relationship with ventricular ejection. Its elastic reservoir index is an important reference parameter for observing the changes of systemic circulation blood pressure. The mechanical stretching experiment is a good method for understand aortic elasticity and Windkessel functions in vitro .
In this study, we concluded that whole-body immersion is a good model for understanding blood redistribution relative cardiac volume overload and this extended problem of aortic elasticity response. Whole-body immersion induced aortic wall adaptations were included improved myogenic activities and the passive tension relative decelerations. All of these in vitro measured parameters were helpful for understand aorta mechanical stretch adapt to increased left ventricular ejection volume.
This research was supported by Hainan Key R&D programs (ZDYF2017121), Hainan student innovation and entrepreneurship training project (201811810066). Zhongguancun science park high technology enterprise authenticated belt and road innovation and entrepreneurship project (20152010634902).
The authors declare that there is no conflict of interests regarding the publication of this article.