Pancreatic Disorders & Therapy
Open Access
ISSN: 2165-7092
ISSN: 2165-7092
Review Article - (2015) Volume 5, Issue 3
Objective: New research on Acute Pancreatitis (AP) led to new classifications of this unpredictable disease and presently two of them are disputing the supremacy. Our aim is to compare the Atlanta 2012 Classification with the Determinant Based Classification in terms of clinical applicability and accuracy.
Method: We performed retrospective analysis of all consecutive cases of AP managed in our tertiary, universityaffiliated emergency center during a period of 12 months. The patients were divided into severity groups according to the Atlanta 2012 and the Determinant-Based Classification. The main outcomes that we used for evaluation were hospital length of stay (H_LOS), intensive care unit (ICU) admission, ICU length of stay (ICU_LOS) and mortality.
Results: 226 patients met the inclusion criteria. Most of the patients are male (61.9%), on the sixth decade of life (mean age: 53.8), biliary stones being the most common etiology of AP (39.4%). Using the aria under the curve (AUC) to compare the predictive accuracy of ICU Admission we found that AUC for the Determinant Based Classification is higher compared to AUC for the Atlanta 2012 (0.973 versus 0.961). AUC is similar for both the Atlanta 2012 Classification and DBC in predicting mortality (0.986 and 0.984 respectively). Both classifications provided similar results considering H_LOS and ICU_LOS.
Conclusions: The Atlanta 2012 and the DBC both predict with increased accuracy the clinical prognosis of patients with AP. The Determinant Based Classification has a slight advantage over the Atlanta 2012 Classification because it succeeded in offering a better prediction for the ICU Admission and ICU_LOS. Although their clinical applicability is similar, there are few aspects that can be improved and worldwide consensus is necessary for uniformity of scientific research.
<Keywords: Acute pancreatitis; Classification; Prognosis
Acute pancreatitis (AP) remains a challenging disease by its various etiologies, multiple clinical aspects and unpredicted evolution. The first major contribution to standardize AP was the 1992 Atlanta Classification [1] but, since then, new information and research emerged as an attempt to eliminate some confusion, to improve severity assessment and to facilitate scientific communications between physicians and different institutions. This improved knowledge led to new classifications: Atlanta 2012 [2] and Determinant Based Classification (DBC) [3]. Both of them make a distinction between the morphological aspect of AP (fluid collection, pancreatic necrosis, etc.) and the systemic impact of AP (transient/permanent organ failure) and they grade AP severity according to these aspects. Thus, Atlanta 2012 and DBC are not entirely alike and, in specific cases, this could lead to different results. If we can take, for example, a patient with AP and peripancreatic fluid collection without necrosis or organ failure, they can be categorized as Severe Acute Pancreatitis (Atlanta 1992), Moderately-Severe Acute Pancreatitis (Atlanta 2012) or Mild Acute Pancreatitis (DBC), which can be really confusing when two clinicians are talking to each other or report their scientific data. Both these two classifications were presented at the end of 2012 and, since then; a new series of articles was published in an attempt to decide which one is more accurate and more useful for clinical use. But the balance does not favor either yet [4-13]. One thing is certain: that both these classifications are better than Atlanta 1992 with regard to outcome measures [10,12,14]. The aim of the current research is to compare Atlanta 2012 Classification with Determinant Based Classification in terms of clinical applicability and accuracy.
We performed retrospective analysis of all consecutive cases of Acute Pancreatitis admitted into the General Surgery Department of our tertiary, university-affiliated emergency center during a period of 12 months (August 2014 to July 2015). We defined patients with AP according to Atlanta 2012 (two out of three criteria): abdominal pain suggestive of AP, serum lipase or amylase activity at least three times greater than the upper limit and characteristic findings on contrasted enhanced computed tomography (CECT) or magnetic resonance imaging (MRI) or transabdominal ultrasonography (US) [2]. The patients were divided into severity groups according to Atlanta 2012 and the Determinant-Based Classification. The main outcomes that we used for evaluation were hospital length of stay (H_LOS), intensive care unit (ICU) admission, ICU length of stay (ICU_LOS) and mortality. Organ failure was assessed according to the modified Marshall scoring system for organ dysfunction [2]. Frequencies and percentage were used as categorical variables. Means and standard deviation were applied for continuous variables. For each classification, testing between grades of severity was done by using Fisher’s exact test and Kruskal-Wallis or One-Way ANOVA as appropriate. To evaluate for normality of distribution we used the Kolmogorov-Smirnov test. To describe the accuracy of each classification system, we used ROC Curve with AUC (area under the curve), Somer’s D and Kendall’s tau correlation. A level of p < 0.05 was used to declare statistical significance. For statistical analysis, we used IBM SPSS Statistics software, version 20.
226 patients with AP met the inclusion criteria. Most of the patients are male (61.9%), on the sixth decade of life (mean age: 53.8), biliary stones being the most common etiology of AP (39.4%). Overall characteristics of patients are described in Table 1. The most common local complications encountered are ANC (acute necrotic collection – 19.5%) and APFC (acute peripancreatic fluid collection – 17.7%). Regarding the persistent organ failure (organ failure more than 48 hours), the most frequent were respiratory (7 patients – 3%) and renal failure (6 patients – 2.6%). Intensive Care Unit (ICU) admission rates are detailed in Tables 2 and 3.
| Count (%) | Mean (Standard Deviation) | ||
|---|---|---|---|
| Gender | Male | 140 (61.9%) | |
| Female | 86 (38.1%) | ||
| Age | 53.85 (14.71) | ||
| Etiology | Biliary | 89 (39.4%) | |
| Idiopathic | 82 (36.3%) | ||
| Alcohol | 40 (17.7%) | ||
| Metabolic | 10 (4.4%) | ||
| ERCP | 2 (0.9%) | ||
| Postoperative | 2 (0.9%) | ||
| Other | 1 (0.4%) | ||
| Local Complication | No | 127 (56.2%) | |
| APFC | 40 (17.7%) | ||
| Pseudocyst | 13 (5.8%) | ||
| ANC | 44 (19.5%) | ||
| WON | 0 (0%) | ||
| Gastric Outlet Dysfunction | 0 (0%) | ||
| Splenic-Portal Thrombosis | 1 (0.4%) | ||
| Colonic Necrosis | 0 (0%) | ||
| Multiple | 1 (0.4%) | ||
| Pancreatic & Peripancreatic Necrosis |
No | 179 (79.2%) | |
| Sterile | 38 (16.8%) | ||
| Infected | 9 (4%) | ||
| Systemic Complication | No | 205 (90.7%) | |
| Yes | 21 (9.3%) | ||
| Organ Failure | No | 192 (85%) | |
| Transient | 20 (8.8%) | ||
| Persistent | 14 (6.2%) | ||
| Intensive Car Unit Admission | No | 212 (93.8) | |
| Yes | 14 (6.2%) | ||
| Intensive Care Unit Length Of Stay | 14 (6.2%) | 8.86 (5.72) | |
| Hospital Length Of Stay | 226 (100%) | 10.30 (10.26) | |
| Mortality | No | 217 (96%) | |
| Yes | 9 (4%) | ||
ERCP – Endoscopic Retrograde Colangiopancreatography; APFC – Acute Peripancreatic Fluid Collection; ANC – Acute Necrotic Collection; WON – Walled-Off Necrosis; ICU – Intensive Care Unit; LOS – Length Of Stay.
Table 1: Patients’ characteristics.
| Atlanta 2012 Classification | Total | |||||
|---|---|---|---|---|---|---|
| Mild | Moderately Severe | Severe | ||||
| Intensive Care Unit (ICU) admission | NO | Count (%) | 116a | 93a | 3b | 212 |
| % within ICU_Admission | 54,7% | 43,9% | 1,4% | 100,0% | ||
| YES | Count | 0a | 2a | 12b | 14 | |
| % within ICU_ Admission | 0,0% | 14,3% | 85,7% | 100,0% | ||
Each subscript letter denotes a subset of ATLANTA 2012 CLASSIFICATION categories whose column proportions do not differ significantly from each other at the ,05 level.
Table 2: Intensive Care Unit (ICU) admission rates according to Atlanta 2012 Classification for patients with acute pancreatitis.
The differences between severity groups in Atlanta 2012 Classification appear only between the moderate severe group and the severe group (Pearson Chi-Square test, p=0.001), while between the mild and the moderate severe groups there is no statistical difference. Applying directional measures (Somers’d) on Atlanta 2012 Classification, we can also observe that the more severe forms are more prone to have ICU admission (d=0.257, p=0.001).
If we split patients according to the Determinant Based Classification and analyze ICU admission rates, we can observe that there are significant differences between the first three groups of severity Mild, Moderate and Severe (p=0.001). The Severe and Critical categories do not differ significantly from each other.
Also applying directional measures (Somers’d) on the Determinant Based Classification, we can observe that the more severe forms are more prone to have ICU admission (d=0.946, p=0.001).
Using the aria under the ROC curve (AUC) to compare the predictive accuracy of ICU Admission, we found that AUC for Determinant Based Classification is higher compared to AUC for Atlanta 2012 (0.973 vs. 0.961) (Figure 1 and Table 6).
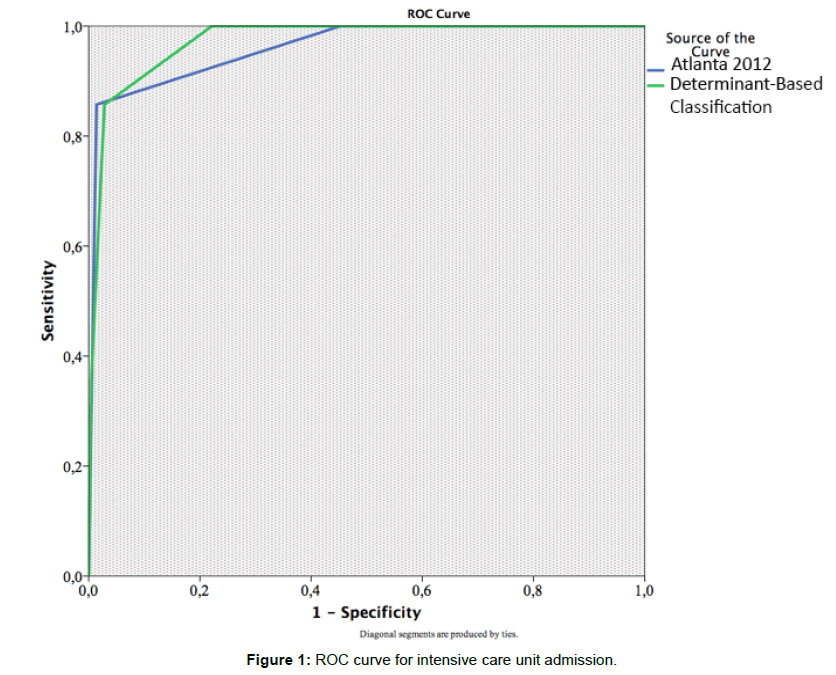
Figure 1: ROC curve for intensive care unit admission.
For the Atlanta 2012 classification, there are no deaths recorded in the Mild and Moderate Severe groups and the significant differences appear only between the Severe and Moderately Severe groups (p=0.001) (Table 3). This aspect is also statistically significant when we apply directional measure (d=0.972, p=0.001).
| Determinant based Classification | Total | ||||||
|---|---|---|---|---|---|---|---|
| Mild AP | Moderate AP | Severe AP | Critical AP | ||||
| Intensive Care Unit (ICU) admission | NO | Count | 165a | 41b | 5c | 1c | 212 |
| % within ICU_ADMISION | 77,8% | 19,3% | 2,4% | 0,5% | 100,0% | ||
| YES | Count | 0a | 2b | 7c | 5c | 14 | |
| % within ICU_ADMISION | 0,0% | 14,3% | 50,0% | 35,7% | 100,0% | ||
Each subscript letter denotes a subset of Determinant Based Classification categories whose column proportions do not differ significantly from each other at the ,05 level.
Table 3: Intensive Care Unit (ICU) admission rates according to Determinant Based Classification for patients with acute pancreatitis.
For the Determinant Based Classification, there are no deaths recorded in the first two groups (Mild and Moderate). The cases of deceased patients are almost equally split between the last two groups of severity (Severe and Critical) (Figure 5). The point of significant statistical deference is between the Moderate and Severe groups (p=0.001) and the trend is also upward: the higher the severity group, the higher the death rate (d=0.968, p=0.001).
The Area under the Curve (AUC) is similar for both Atlanta 2012 Classification and DBC in predicting mortality (0.986 and 0.984 accordingly) (Figure 2 and Table 6).
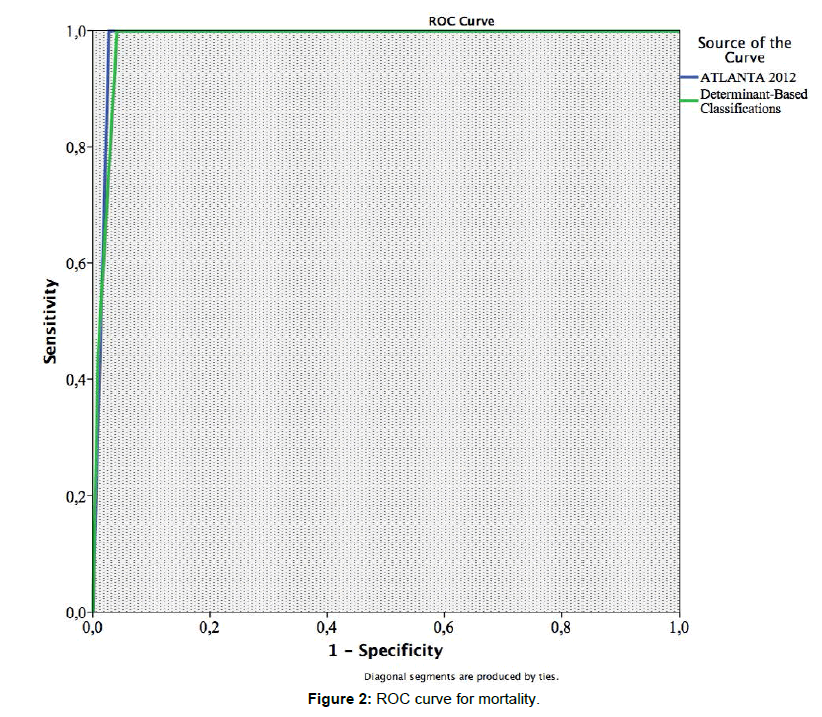
Figure 2: ROC curve for mortality.
The Intensive Care Unit Length of Stay (ICU_LOS) and the Hospital Length of Stay (H_LOS) are other two outcome parameters that we analyzed. The results are detailed in Table 4 for Atlanta 2012 Classification and Table 5 for Determinant Based Classification.
| N | Mean | Std. Deviation | 95% CI for Mean | |||
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| ICU_LOS | Mild | 116 | ,00 | ,000 | ,00 | ,00 |
| Moderately_S | 95 | ,09 | ,685 | -,04 | ,23 | |
| Severe | 15 | 7,67 | 6,532 | 4,05 | 11,28 | |
| Total | 226 | ,55 | 2,544 | ,22 | ,88 | |
| H_LOS | Mild | 116 | 6,35 | 3,672 | 5,68 | 7,03 |
| Moderately_S | 94 | 12,04 | 6,814 | 10,65 | 13,44 | |
| Severe | 15 | 29,87 | 26,568 | 15,15 | 44,58 | |
| Total | 225 | 10,30 | 10,261 | 8,95 | 11,65 | |
Table 4: Intensive Care Unit (ICU) and Hospital (H) length of stay (LOS) according to Atlanta 2012 Classification for patients with acute pancreatitis.
| N | Mean | Std. Deviation | 95% CI for Mean | |||
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| ICU_LOS | Mild AP | 165 | ,00 | ,000 | ,00 | ,00 |
| Moderate AP | 43 | ,21 | 1,013 | -,10 | ,52 | |
| Severe AP | 12 | 5,50 | 6,749 | 1,21 | 9,79 | |
| Critical AP | 6 | 8,17 | 6,555 | 1,29 | 15,05 | |
| H_LOS | Mild AP | 164 | 7,65 | 5,256 | 6,84 | 8,46 |
| Moderate AP | 43 | 12,65 | 5,928 | 10,83 | 14,48 | |
| Severe AP | 12 | 21,50 | 11,517 | 14,18 | 28,82 | |
| Critical AP | 6 | 43,50 | 36,429 | 5,27 | 81,73 | |
Table 5: Intensive Care Unit (ICU) and Hospital (H) length of stay (LOS) according to Determinant Based Classification for patients with acute pancreatitis (AP).
For the Atlanta 2012 Classification, the patients in the Mild group have no ICU admission, the patients in the Moderately severe group spent only a few days in ICU (an average of 0.09 days) while patients from the Severe group spent the most time in ICU (an average of 7.67 days) (Table 4 and Figure 3). These differences for ICU_LOS are also statistically significant (p=0.001).
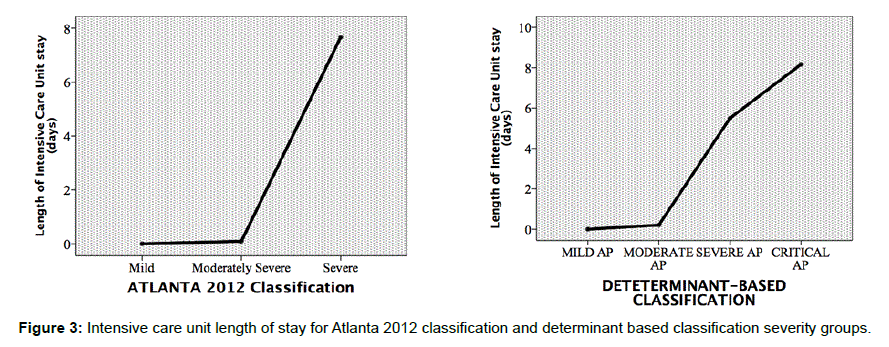
Figure 3: Intensive care unit length of stay for Atlanta 2012 classification and determinant based classification severity groups.
The same results and statistical significance are also recorded for the H_LOS: the patients in the Mild group have an average of 6.35 days of hospital stay, the patients in the Moderately Severe group spent an average of 12.04 days in the hospital and those in the Severe group have an average of 29.87 days for H-LOS (Table 4 and Figure 4); (p=0.001)
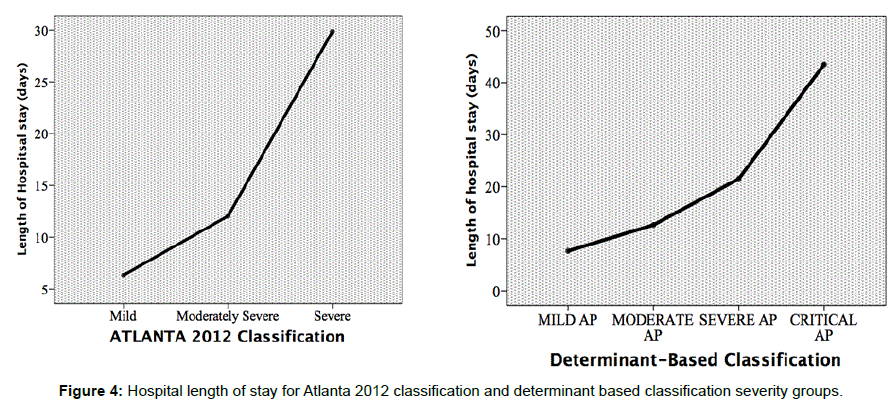
Figure 4: Hospital length of stay for Atlanta 2012 classification and determinant based classification severity groups.
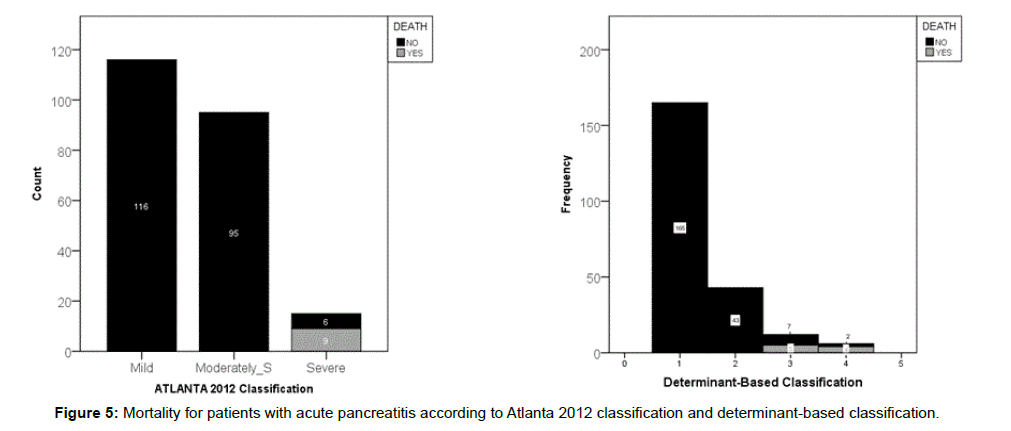
Figure 5: Mortality for patients with acute pancreatitis according to Atlanta 2012 classification and determinant-based classification.
For the Determinant Based Classification, the patients in the Mild group have no ICU admission neither, those in the Moderate group spent an average of 0.21 days in ICU, for the Severe group, there was an average of 5.5 days in ICU and, finally, the Critical group had an average of 8.17 days in ICU – Table 5 and Figure 3. These differences in ICU_LOS are also significant (p=0.001).
Splitting the patients according to the DBC severity groups and analyzing the Hospital Length of Stay (H_LOS), we found similar results: the patients in the Mild group have an average of 7.65 days for H_LOS, those in the Moderate group spent an average of 12.65 days in the hospital, while the last two groups, Severe and Critical, have an average of 21.5 days and 43.5 days H_LOS accordingly – Table 5 and Figure 4; These differences between the groups also reached statistical significance (p=0.001).
In order to compare these two classifications systems (Atlanta 2012 and DBC) we performed a nonparametric correlations using Kendall correlation coefficient for each classification and ICU_LOS and H_LOS (Table 6). All the correlation are statistically significant (p=0.01). For ICU_LOS Kendall correlation coefficient was higher for BDC (0.490) than for Atlanta 2012 (0.417). Analyzing the H_LOS we find the opposite situation: Kendall correlation coefficient was higher for Atlanta 2012 (0.437) than for DBC (0.389).
| OUTCOMES | CLASSIFICATION SYSTEMS | |
|---|---|---|
| Atlanta 2012 | DBC | |
| ICU Admission | ||
| AUC | 0.973 | 0.961 |
| Mortality | ||
| AUC | 0.986 | 0.984 |
| ICU_LOS | ||
| Kendall Correlation Coefficient | 0.417 | 0.490 |
| H_LOS | ||
| Kendall Correlation Coefficient | 0.437 | 0.389 |
Table 6: Prediction of clinical outcomes for Atlanta 2012 and Determinant-Based Classifications.
The demographic data of our study does not bring any particularities, as most of our patients are males (around 50 years old) and the main etiology for AP is the biliary one. As a particular aspect, we mention the idiopathic etiology of AP, which came in second position; this could hide a number of alcohol induced AP as our patients have the tendency to not recognize their alcohol consumption or to misinterpret the amount of alcohol they consume.
The Atlanta 2012 Classification is not just a new classification, but it also includes a clearer definition of the local and systemic complications and it makes a difference between the early and the late phase of AP and it looks like a system for classifying the disease. DBC seems more easy to use as it requires remembering only two aspects: the status of the pancreatic necrosis (absent, sterile or infected) and the organ failure (absent, transient or persistent) but it requires a contrast-enhanced computed tomography (CECT) to completely characterize the patients.
Comparing the results for the ICU Admission, we can observe that for the Atlanta 2012 Classification the first two categories (Mild and Moderately Severe) did not differ significantly. This could be explained by the fact that in the Moderately Severe category there are included not only the patients with pancreatic necrosis but also those with fluid collection. The patients without acute necrosis have a general tendency to have an easier course of disease. The difference appears when the severe category is compared to the Moderately Severe one, mainly because in the severe group there are patients with persistent organ failure that really needs intensive care.
Using the Determinant Based Classification, the need for the ICU Admission is more accurately detected because the statistical differences appear between the first three groups (Mild, Moderate and Severe). The last two groups (Severe and Critical) had the same ICU Admission rate maybe because all patients admitted to this category need intensive care (either they have persistent organ failure or infected necrosis). Comparing these two classification systems by using the ROC curve, the BDC is more accurate because it has a larger AUC. The results are specific to our study because in other papers, authors find a similarity between the classifications [10] or favored the Atlanta 2012 Classification [15].
Mortality analyses also provided similar results. In the Atlanta 2012 Classification, the first two categories (Mild and Moderate Severe) record no deaths and the significance appears only when the Severe category is taken into account. Analyzing the four categories of severity of the Determinant Based Classification for Mortality, we noticed that there are also no significant differences between the first two categories (Mild and Moderate – “the easy ones”, with no deaths) and the last two categories (Severe and Critical – “the difficult ones”, each had the same number of deaths).
From this point of view, both classifications can draw a clear mortality line between specific categories. This fact is confirmed by the same AUC for ROC curve when mortality is analyzed. Similar results appear in recent studies [10,16].
Nevertheless, our results suggest that there is room for a few possible improvements. Considering the Atlanta 2012 Classification, a better distinction between the Mild and the Moderate Severe categories should be done and, for DBC, the last two categories (Severe and Critical) are very similar so maybe they will be combined into a single group in the future [8]. The need for further improvement of these two classifications is also emphasized by other authors [7,16]. The other two outcomes that we analyzed (ICU LOS and Hospital LOS) didn’t offer any surprises. Both classifications (Atlanta 2012 and DBC) manage to split the patients into severity groups that differ from each other in a statistically significant way, which is consistent with recent literature [4,10]. Nevertheless, when we compare the correlation between these two classification systems we find out that Atlanta 2012 offers a better prediction of H_LOS and DBC is more accurate in predicting ICU_ LOS. This result is also similar with an article published in 2013 [10].
Overall, higher grades of severity are significantly associated with worse clinical outcome for both classifications.
The Atlanta 2012 and the DBC both predict with increased accuracy the clinical prognosis of patients with AP. Because it provides a better prediction for ICU Admission and ICU_LOS and it is easier to use on clinical setting, we believe that the Determinant Based Classification is better than the Atlanta 2012 Classification. Although their clinical applicability is similar, there are few aspects that can be improved and a worldwide consensus is necessary for uniformity of scientific research.
This paper is financed by the project The Excellence Program for Doctoral and Postdoctoral Multidisciplinary Research on Chronic Diseases (contract no: POSDRU/159/1.5/S/133377); this project is co-financed by the European Social Fund through Human Resources Development Sector Operational Program.