Journal of Fertilization: In Vitro - IVF-Worldwide, Reproductive Medicine, Genetics & Stem Cell Biol
Open Access
ISSN: 2375-4508
ISSN: 2375-4508
Research Article - (2016) Volume 4, Issue 2
Objective: To evaluate the effectiveness of fallopian tube embolization on in vitro fertilization and embryo transfer in patients with hydrosalpinx.
Methods: In total, 174 IVF-ET treatment cycles in patients with hydrosalpinges that pretreated with fallopian tube embolization and 696 cycles in age-matched patients with bilateral tubal obstruction were involved in this study. Compare clinical pregnancy rate, live birth delivery rate, ectopic pregnancy rate, abortion rate, preterm birth rate and fetal malformation rate between the two groups.
Results: (1) There was no statistically significant difference in patient age, years of infertility, basal FSH value, Gn dosage; oocyte number in fresh cycles and number of embryos transferred between the two groups. (2) The fertilization, cleavage, and good quality embryo rates were higher in the embolization group than the control group (76.3% vs. 72.9%, P = 0.006; 97.2% vs. 95.3%, P = 0.004; and 24.8% vs. 20.6%, P = 0.001); the abortion rate in the embolization group was significantly lower than the control group (2.3% vs. 7.8%, P = 0.01). Clinical pregnancy (38.5% vs. 37.8%, P = 0.86), live birth delivery (33.3% vs. 28.7%, P = 0.24), ectopic pregnancy (2.3% vs. 1.4%, P = 0.42), and preterm birth rates (20.7% vs.21.5%, P = 0.90) were not significantly different between the two groups, and the tube embolization technique did not increase the incidence of fetal malformations.
Conclusions: (1) Tubal embolization does not affect the clinical pregnancy rate of in vitro fertilization–embryo transfer, what is more it reduce the abortion rate. (2) Tubal embolization is a safe and effective method and worthy of clinical application.
<Keywords: Hydrosalpinx, Fallopian tube embolization, IVF-ET, Pregnancy outcomes
The most common manifestation of tubal disease is hydrosalpinx, which occurs in 10%–30% of infertile couples suffering from tubal factors [1]. In addition, hydrosalpinx exert an adverse effect on the outcome of in vitro fertilization by reducing the probability of implantation and by increasing the risk of early pregnancy loss [2,3].
The mechanisms of how hydrosalpinx negatively affect the implantation rate are yet to be identified. A number of underlying pathogenic mechanisms have been proposed, as follows: the effects of bacterial toxins in the hydrosalpingeal fluid on gametes or embryos; reduced expression of cytokines and integrins; changes in the endometrial receptivity; and the possible mechanical flushing of the embryo from the endometrium [4-6].
The Practice Committee of the American Society for Reproductive Medicine in collaboration with The Society of Reproductive Surgeons concluded “…of six women with hydrosalpinx, after pretreatment at least one will get pregnant before IVF” [7]. Currently, pretreatments for hydrosalpinx include salpingectomies, salpingostomies, proximal tubal ligation, ultrasound-guided hydrosalpinx aspiration, and interventional tubal occlusion [8-12]. A recent Cochrane review concluded that laparoscopic salpingectomy or tubal occlusion before IVF increases the probability of pregnancy [5]. Salpingectomy has been shown to be an effective option and has the advantage of removing the risk of pelvic inflammatory. In contrast, the drawbacks of salpingectomy include the invasiveness of the procedure, the difficulty of the procedure in the presence of dense adhesions, and the need for anesthesia. A salpingectomy may damage the fallopian-ovarian aortic arch, resulting in reduced blood supply to the ovaries, and reduced ovarian gonadotropin reactivity [10,13]. Vaginal ultrasound-guided aspiration has obvious advantages, such as simplicity, efficacy, less invasive, and less expensive; vaginal ultrasound-guided aspiration has a high recurrent rate ranging from 22.2% to 30.8% [14,15]. Tubal embolism refers to the mechanical embolization with a micro-spring commonly used in interventional embolization therapy by selective tubal cannulation through the microcatheter into the coil and interstitial tubal isthmus. The mechanism underlying tubal embolism is as follows: (1) complete mechanical blockage of the fallopian tube lumen; and (2) necrotic tissue accumulation due to mechanical compression of materials formed following the release of alkaline phosphatase and changes in the microenvironment embolism consisting of helper lymphocyte aggregation and fibrovascular tissue with increased tubal obstruction [11]. Tubal embolism represents a promising alternative to salpingectomy, especially in patients in whom the pelvic anatomy is distorted. Tubal embolism is less invasive, easier to perform, and faster. The effects of embolism coils on the success of IVF are uncertain. If pregnancy is achieved, the risk of the microinsert to the patient, fetus, and continuation of pregnancy are still unclear.
Nowadays researches about tubal embolism are limited. The application of tubal embolism is not prevailing yet. This paper mainly discussed the impact of tubal embolization on pregnancy outcomes, in order to demonstrate the value of tubal embolism.
The study had been approved by the Institutional Review Board of Shengjing Hospital Affiliated to China Medical University (2015PS125K). A total of 174 cycles in patients with hydrosalpinx who received interventional tubal embolization before IVF–ET between January 2009 and December 2013 served as the experimental group. A total of 696 cycles in age-matched patients with bilateral tubal obstruction received IVF–ET and served as the control group. The study inclusion criteria were as follows: (1) age, 25–39 years; (2) menstrual regularity with normal hormone levels; (3) no evidence of endometriosis, uterine malformations, polycystic ovary syndrome, or diseases that could affect pregnancy; (4) normal semen analysis and no sperm–egg binding barriers; and (5) fresh embryos for transfer. The exclusion criteria were as follows: (1) age, older than 40 years; (2) unexplained infertility, endometriosis, uterine malformations, or polycystic ovary syndrome; (3) oligospermia or asthenospermia; (4) hydrosalpinx pretreated with other methods (such as salpingectomies, salpingostomies).
Patients were placed in lithotomy position followed with sterilization of perineum, vagina and cervix. Under digital subtraction angiography monitoring, we delivered a double balloon hysterosapingography catheter into the uterine cavity and fixed it, then observed not only the shape and size of the uterine cavity, but also the position, shape and degree of hydrosalpinx of the bilateral fallopian tubes after the injection of contrast medium. After the operation above, we delivered the catheter to the affected cornua uteri and delivered a 3F catheter (Cook, USA) to the isthmic portion under the guidance of a microguidewire, then injected saline with antibiotic to release the adhered fimbrial portion and pushed the platinum micro-coils (Cook, USA) into the interstitial portion to occlude the proximal tube through the 3F catheter [16] (Figure 1). According to the baseline endocrine level and antral follicle count, we adopted an individualized ovarian hyperstimulation program. When the dominant follicle reached a diameter of approximately 18-20 mm, we retrieved eggs under the guidance of ultrasound approximately 36 h after an intramuscular injection of human chorionic gonadotropin (HCG; approximately 5000–10,000 IU). Progesterone (60 mg intramuscular injection) and estradiol (2 mg oral once daily) were administered after retrieving eggs for luteal support by starting day 1. Fourteen days after embryo transfer, blood HCG testing and an ultrasonogram evaluation were performed to visualize the gestational sac, confirm cardiac activity, and rule out an ectopic gestation.
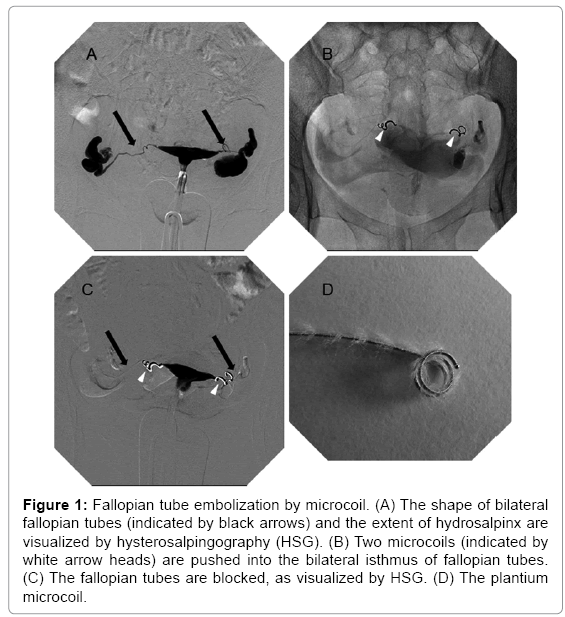
Figure 1: Fallopian tube embolization by microcoil. (A) The shape of bilateral fallopian tubes (indicated by black arrows) and the extent of hydrosalpinx are visualized by hysterosalpingography (HSG). (B) Two microcoils (indicated by white arrow heads) are pushed into the bilateral isthmus of fallopian tubes. (C) The fallopian tubes are blocked, as visualized by HSG. (D) The plantium microcoil.
The following clinical data were compared in the two groups: age; duration of infertility; basal FSH values; Gn dosage; oocyte number in fresh cycles; number of embryos transferred; and the fertilization rate (total number of fertilized eggs / total number of oocytes); cleavage rate (total cleavage embryos / total number of fertilized eggs), good quality embryo rate (total quality embryos / total number of fertilized eggs), clinical pregnancy rate (the number of clinical pregnancies / transfer cycles [including ectopic pregnancies]), live birth delivery rate (live births and birth / total number of transfer cycles [twin delivery times by calculation]); ectopic pregnancy rate (ectopic pregnancy / total number of transfer cycles); abortion rate (abortions / total number of transfer cycles); preterm birth rate (the number of preterm / live births); and fetal malformation rate.
Using SPSS (IBM, Armonk, NY, USA, version 22.0), a Student’s t-test, Mann-Whitney U test and χ2 test were used for statistical analysis. P<0.05 was considered statistically significant.
The general clinical indicators of the two groups of patients, including the age, duration of infertility; basal FSH values; Gn dosage; oocyte number in fresh cycles; and number of embryos transferred, were not statistically significant (P>0.05; Table 1).
| Embolization Group Mean ± RSEa/Median (QR)b 95%CI | Control Group Mean ± RSEa/ Median (QR)b 95%CI | P-value | |
|---|---|---|---|
| Age (year) | 31.48 ± 3.47 30.96-32.00 |
32.07 ± 3.78 31.79-32.35 |
0.07 |
| Duration of infertility (year) | 4 (2-6) 4.39-5.37 |
4 (2-6) 4.41-4.92 |
0.15 |
| Basal FSH value (IU/L) | 7.67 ± 2.25 7.34-8.01 |
7.80 ± 2.27 7.64-7.98 |
0.48 |
| Gn dosage | 27.43 ± 11.68 25.68-29.18 |
27.28 ± 11.61 26.42-28.15 |
0.88 |
| Oocyte number | 8 (5-12) 8.31-9.99 |
8 (5-13) 8.77-9.60 |
0.83 |
| Number of embryos transferred | 2 (2-3) 2.10-2.78 |
2 (2-3) 2.11-2.20 |
0.58 |
aNormally distributed data
bNon-normally distributed data
Table 1: Demographics of the Embolism Group and Control Group.
As shown in Figure 1, the fallopian tube was blocked after embolization by the microcoil (Figure 1D), visualized by hysterosalpingography.
The clinical outcomes of the two patient groups receiving IVF–ET treatment were as follows (Table 2): among the 174 treatment cycles with embolization, there were 67 clinical pregnancies, 58 live births, 12 premature births, four ectopic pregnancies, four abortions, and no fetal malformations; among the 696 control treatment cycles, there were 263 clinical pregnancies, 200 live births, 43 premature births, ten ectopic pregnancies, 54 abortions, and no fetal malformations.
| Embolization Group | Control Group | P-value | |
|---|---|---|---|
| Fertilization rate(%) | 76.3 | 72.9 | 0.006 |
| Cleavage rate(%) | 97.2 | 95.3 | 0.004 |
| Good quality embryo rate(%) | 24.8 | 20.6 | 0.001 |
| Clinical pregnancy rate (%) | 38.5 | 37.8 | 0.86 |
| Live birth rate (%) | 33.3 | 28.7 | 0.24 |
| Ectopic pregnancy rate(%) | 2.3 | 1.4 | 0.42 |
| Abortion rate (%) | 2.3 | 7.8 | 0.01 |
| Preterm birth rate(%) | 20.7 | 21.5 | 0.90 |
Table 2: The clinical outcomes of fallopian tube embolization.
The good quality embryo, clinical pregnancy, and live birth rates were compared between the embolization and control groups. The main outcomes in our study were the clinical pregnancy and live birth rates. Based on a χ2 test, the embolization group exhibited higher fertilization, cleavage, and good quality embryo rates than the control group, although no significant difference was observed in the clinical pregnancy and live birth rates. The rate of early pregnancy loss was significantly lower in the experimental group than the control group (2.3% vs. 7.8%, P = 0.01, Table 2).
Li et al. [11] first reported the outcome of fallopian tube embolization in IVF-ET patients with hydrosalpinx. It was found that the clinical pregnancy rate was slightly higher in the patients group underwent embolization, as compared to the patients underwent fallopian tube occlusion, though the difference was not statistically significant. The tubal pregnancy and pregnancy loss rates were significantly lower in the embolization group than those of the control group. Lu et al. [16] compared three different treatment methods (salpingectomies, salpingostomies and fallopian tube embolization) of hydrosalpinx before IVF-ET. They found that the embolization group had better clinical pregnancy rate and implantation rate, and lowered abortion rate and tubal pregnancy rate. Our prior work published in 2012 [16] found that fallopian tube embolization before IVF-ET had a higher clinical pregnancy rates than hydrosalpinx without a treatment. Fallopian tube embolization does not affect ovarian blood supply, nor by the intraperitoneal adhesion effect. For hydrosalpinx cases with severely abdominal adhesions has important clinical application value. However, the risks of the microinsert to the patient, the fetus, and continuation of the pregnancy were unclear. So in order to discuss the safety of fallopian tube embolization, we continued to enroll some patients that met the inclusion criteria and excluded the patients that not received IVF-ET in Shengjing Hospital. In the current study, we showed that there were no significant differences in the number of oocytes retrieved, the fertilization rate, and the cleavage rate between the embolization and control groups, indicating that embolization does not affect the tubal ovarian response to gonadotropins, or the quality of oocytes. In addition, the good quality embryo rate of the embolization group was significantly higher (P<0.001) than that in the control group. The clinical pregnancy and live birth rates of the embolization group were higher as compared to the control group, although the difference was not statistically significant. We thus conclude that tubal embolization did not negatively affect the outcome of IVF. In the past, if pregnancy was achieved, the risks of the microinsert to the patient, the fetus, and continuation of the pregnancy were unclear; however, based on our study the risks in the embolization group did not exceed the risks in the control group.
The potential relationship between the embolization coils protruding into the uterine cavity and obstetric complications is an important theoretical concern. In our study, the early pregnancy loss rate was lower in the embolization group (2.3% vs. 7.8%, P = 0.01), indicating the beneficial effect of embolization to the outcome of IVF. In addition, the babies born in the embolization group did not appear abnormal at all.
There were only a few researches published before about tubal embolism. Most studies focused on the contrast between tubal embolization, operation and hydrosalpinx without pretreatment [16,17]. In our study, we aimed to compare the outcome of IVF-ET between tubal embolization and bilateral tubal obstruction (as “normal” patients in IVF-ET). Though the results did not show a better pregnant outcome, we could at least conclude that tubal embolization is a safe and effective option for the patients diagnosed with hydrosalpinx.
The limitation of the study was that the sample size was not large enough, and the follow-up after birth was not included. To evaluate the safety of tubal embolization needs more studies and longer time follow-ups.
Interventional treatment with tubal embolism is a new method for pre-processing hydrosalpinx. Compared with other methods currently in use clinically, tubal embolism requires no surgery and does not cause anesthetic complications. It is simple, safe, and economical. Tubal embolism does not increase the clinical abortion, premature birth, and fetal malformation rates, and is an effective method worthy of clinical application.
The authors thank Huai L Feng for his constructive suggestions.